|
What is already known on this topic? The largest U.S. mumps outbreak since 2006 began at a summer camp in New York in June 2009. By October 30, 2009, the outbreak included 179 confirmed and probable cases, primarily among members of certain highly vaccinated, tradition-observant Jewish communities. What is added by this report? As of January 29, 2010, the outbreak included 1,521 cases, 97% of which had occurred in members of the same tradition-observant religious community. Among patients for whom vaccination status was reported, 88% had received at least 1 dose of mumps-containing vaccine, and 75% had received 2 doses. What are the implications for public health practice? Although vaccination alone does not prevent all mumps outbreaks, maintaining high measles, mumps, and rubella (MMR) vaccination coverage remains the most effective way to prevent outbreaks and limit their size when they occur. |
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Update: Mumps Outbreak --- New York and New Jersey, June 2009--January 2010
Please note: An erratum has been published for this article. To view the erratum, please click here.
State and local health departments, in collaboration with CDC, continue to investigate a mumps outbreak that began in New York in June 2009 (1). The index case occurred in a boy aged 11 years who had returned on June 17 from a trip to the United Kingdom, where approximately 7,400 reports of laboratory-confirmed mumps were received by the Health Protection Agency in 2009.* He then attended a New York summer camp for tradition-observant Jewish boys, where he became symptomatic on June 28. Subsequently, other camp attendees and a staff member were reported to have mumps, and transmission continued in multiple locations when the camp attendees returned home. As of January 29, 2010, a total of 1,521 cases had been reported, with onset dates from June 28, 2009, through January 29, 2010, a substantial increase from the 179 cases reported as of October 30, 2009 (1). The outbreak has remained confined primarily to the tradition-observant Jewish community, with <3% of cases occurring among persons outside the community. The largest percentage of cases (61%) has occurred among persons aged 7--18 years, and 76% of the patients are male. Among the patients for whom vaccination status was reported, 88% had received at least 1 dose of mumps-containing vaccine, and 75% had received 2 doses. This is the largest mumps outbreak that has occurred in the United States since 2006 (2). Although mumps vaccination alone was not sufficient to prevent this outbreak, maintaining high measles, mumps, and rubella (MMR) vaccination coverage remains the most effective way to prevent outbreaks and limit their size when they occur.
Mumps cases included in this report were reported by January 29, 2010. Cases were classified according to the 2008 case definition of the Council of State and Territorial Epidemiologists†; only cases of probable and confirmed mumps are included in this report. In the United States, the Advisory Committee on Immunization Practices (ACIP) recommends that children receive 2 doses of measles, mumps, and rubella (MMR) vaccine, with the first dose administered at 12--15 months and the second dose near the time of school entry (at 4--6 years).§ Methods used to obtain the vaccination status of patients have included parental report, review of vaccination cards, and verification from health-care providers.
The 1,521 outbreak-related mumps cases have been reported from several counties in New York and New Jersey; local transmission is continuing (Figure). The majority (675 [44%]) of cases have been reported from New York City (primarily Brooklyn), followed by Orange County, New York (364 [24%]); Rockland County, New York (298 [20%]); and four counties in New Jersey (159 [10%]). Twenty-five (2%) cases (reported during June 28--September 8) were associated with the summer camp in Sullivan County, New York; however, no additional cases occurred in the county after the camp ended in late August. Of the 1,521 patients, 1,477 (97%) are members of the tradition-observant Jewish community. Of the 44 cases not associated with this religious community, 33 have been reported from New York City; seven from New Jersey; two from Orange County, New York; and two from Rockland County, New York. Many of these outside cases have occurred among persons who have reported regular contact with members of the affected community.
Diagnostic laboratory testing for mumps (i.e., detection of mumps immunoglobulin M antibodies by various methods, detection of mumps RNA by real-time reverse transcription--polymerase chain reaction, or isolation of mumps virus in cell culture) has been performed for 761 (50%) cases. Of these, 385 (51%) cases are laboratory confirmed.
Of the 1,518 patients whose age is known, 1,385 (91%) are aged >6 years (Figure). The median age of patients is 15 years (range 3 months--90 years) and is similar in all areas with ongoing transmission except New Jersey, where the median age is 17 years. Of the 1,489 patients whose sex is known, 1,136 (76%) are male. Sixty-five reports of complications from mumps have been received: orchitis (55 cases), pancreatitis (five cases), aseptic meningitis (two cases), transient deafness (one case), Bell's palsy (one case), and oophoritis (one case). Nineteen hospitalizations from mumps have been reported; no deaths have occurred.
Vaccination status is known for 1,115 patients: 966 (91%) of 1,062 patients aged ≤18 years and 149 (33%) of 456 patients aged ≥19 years (Table). Of these patients, 976 (88%) had received at least 1 dose of mumps-containing vaccine before the outbreak, and 839 (75%) had received 2 doses. Among patients aged 7--18 years, the age group with the majority of cases and for whom 2 doses of MMR vaccine is recommended, 93% had received at least 1 dose, and 85% had received 2 doses. The vaccination status of the patients varies by location. The percentage of patients aged >6 years (for whom vaccination status is known) who had received 2 doses of mumps vaccine is highest in Orange County, New York (86%), followed by New York City (83%), New Jersey (76%), and Rockland County, New York (73%).
Public health response measures in all affected areas have continued throughout the outbreak. Health-care providers have been notified about the ongoing outbreak, the importance of verifying that children have received all recommended vaccinations, and the need to offer vaccinations to adults with unknown vaccination status who do not have a history of mumps. State and local health departments also have worked with affected schools to enhance vaccination policies, including policies to exclude unvaccinated children from school during outbreaks and to isolate children at home for 5 days after onset of parotitis. Certain jurisdictions have encouraged providers to offer a second dose of MMR vaccine to children aged 1--4 years; however, this strategy has not been a focus of the public health response because of the small proportion (4.9%) of cases reported in this age group.
Beginning on January 19, 2010, in Orange County, New York, public health officials began offering a third dose of MMR vaccine in three schools where, despite documentation of a high level of 2-dose coverage among students, transmission had continued for >2 months. This intervention is being carried out under an Institutional Review Board--approved protocol that provides for an evaluation of the impact of the intervention.
Reported by
P High, MHS, Ocean County Health Dept, EF Handschur, MPH, OS Eze, MD, B Montana, MD, C Robertson, MD, C Tan, MD, New Jersey Dept of Health and Senior Svcs. JB Rosen, MD, KP Cummings, MPH, MK Doll, MPH, JR Zucker, MD, CM Zimmerman, MD, New York City Dept of Health and Mental Hygiene; T Dolinsky, Rockland County Dept of Health; S Goodell, MPH, B Valure, Orange County Health Dept; C Schulte, D Blog, MD, E Rausch-Phung, MD, P Smith, MD, New York State Dept of Health. A Barskey, MPH, G Wallace, MD, P Kutty, MD, H McLean, PhD, K Gallagher, DSc, R Harpaz, MD, GL Armstrong, MD, L Lowe, MS, R McNall, PhD, J Rota, MPH, P Rota, PhD, C Hickman, PhD, WJ Bellini, PhD, Div of Viral Diseases, National Center for Immunization and Respiratory Diseases. I Ogbuanu MD, A Apostolou, PhD, EIS officers, CDC.
Editorial Note
The mumps outbreak in the New York-New Jersey area has grown substantially, and anecdotal reports from certain affected areas suggest that the rate of new cases is not decreasing; the appearance of a downward trend in recent weeks (Figure) is partly a result of reporting delays. The outbreak is occurring almost exclusively in a specific religious community, and no cases outside this community have resulted in sustained transmission.
Like the mumps outbreaks that occurred in 2006 (2), much of the current outbreak is occurring in congregate settings, where prolonged, close contact among persons might be facilitating transmission. Within the affected religious community, cases have occurred predominantly among school-aged boys, who attend separate schools from girls. The higher rate among boys might be a result of the additional hours that boys in this community spend in school compared with girls, including long periods in large study halls, often face-to-face with a study partner.
In addition, transmission in the community overall might be facilitated by relatively large household sizes. According to the 2000 U.S. Census, the mean household size in one of the affected communities was 5.7, compared with a mean U.S. household size of 2.6. The limited transmission to persons outside the community might be a result of the relatively less interpersonal contact between persons inside and outside the community.
Although the school settings and large household sizes might be promoting transmission, the high vaccination coverage in the affected community likely is limiting the size of the outbreak. In addition, high vaccination coverage in surrounding communities is the most plausible reason that the few cases outside of the affected community have not caused other outbreaks.
In this outbreak, as in other recent mumps outbreaks among highly vaccinated populations (3), most cases have occurred in vaccinated persons. The mumps vaccine has greatly reduced the incidence of mumps in the United States. From 1967, when the mumps vaccine was first licensed, to the early 2000s, the number of reported cases decreased from 186,000 to <500 annually (2). Nonetheless, the effectiveness of the mumps component of the MMR vaccine is lower than that of the measles and rubella components. Estimates of the effectiveness of the mumps vaccine have varied in previous studies, ranging from 73% to 91% after 1 dose and from 79% to 95% after 2 doses (3--5). At least one study found 2 doses to be more effective than 1 dose (6).
Public health officials began offering a third dose of vaccine to students in certain schools in Orange County, New York, because mumps transmission had continued among students, despite their high rate of 2-dose coverage. Although a previous study indicated that a third dose of MMR vaccine for seronegative college students resulted in rapid seroconversion with a low rate of IgM response, which is indicative of an anamnestic immune response (7), ACIP has not recommended a third dose, and no data exist on the effectiveness of a third dose in either reducing the risk for mumps or altering the course of an outbreak. Data obtained from use of the third dose of MMR vaccine in Orange County might be used to guide future options for mumps outbreak control in settings with high 2-dose coverage.
This outbreak emphasizes that mumps outbreaks can occur in highly vaccinated populations. Although several factors play a role in mumps control in the United States (Box), maintenance of high 2-dose MMR vaccine coverage remains the most effective way to prevent and limit the size of mumps outbreaks.
References
- CDC. Mumps outbreak---New York, New Jersey, Quebec, 2009. MMWR 2009;58:1270--4.
- Barskey AE, Glasser JW, LeBaron CW. Mumps resurgences in the United States: a historical perspective on unexpected elements. Vaccine 2009;27:6186--95.
- Dayan GH, Rubin S. Mumps outbreaks in vaccinated populations: are available mumps vaccines effective enough to prevent outbreaks? Clin Infect Dis 2008;47:1458--67.
- Hviid A, Rubin S, Muhlemann K. Mumps. Lancet 2008;371:932--44.
- Marin M, Quinlisk P, Shimabukuro T, et al. Mumps vaccination coverage and vaccine effectiveness in a large outbreak among college students---Iowa, 2006. Vaccine 2008;26:3601--7.
- Cohen C, White JM, Savage EJ, et al. Vaccine effectiveness estimates 2004--2005 mumps outbreak, England. Emerg Infect Dis 2007;13:12--7.
- Date AA, Kyaw MH, Rue AM, et al. Long-term persistence of mumps antibody after receipt of 2 measles-mumps-rubella (MMR) vaccinations and antibody response after a third MMR vaccination among a university population. J Infect Dis 200815;197:1662--8.
- CDC. Updated recommendations of the Advisory Committee on Immunization Practices (ACIP) for the control and elimination of mumps. MMWR 2006;55:629--30.
* Available at http://www.hpa.org.uk/hpr/archives/2010/news0210.htm#mmps.
† An illness with acute onset of unilateral or bilateral tender, self-limited swelling of the parotid or other salivary glands, lasting at least 2 days, and without other apparent cause. Probable case: a case that meets the clinical case definition without laboratory confirmation and is epidemiologically linked to a clinically compatible case. Confirmed case: a case that 1) meets the clinical case definition or occurs in a patient with a clinically compatible illness and 2) is either laboratory confirmed or is epidemiologically linked to a confirmed case. Available at http://www.cdc.gov/ncphi/disss/nndss/casedef/mumps_2008.htm.
§ ACIP recommends 2 doses of mumps-containing vaccine for all school-aged children (i.e., grades K--12) and for adults at high risk for disease (i.e., persons who work in health-care facilities, international travelers, and students at post--high school educational institutions). Health-care workers born in or after 1957 without laboratory evidence of immunity should receive 2 doses of mumps-containing vaccine, and those born before 1957 without laboratory evidence of immunity should consider receiving 1 dose. During outbreaks, ACIP recommends offering a second dose of vaccine to children aged 1--4 years (8).
FIGURE. Number (n = 1,494*) of reported confirmed or probable mumps cases,† by week of illness onset and age group --- New York and New Jersey, June 2009--January 2010§
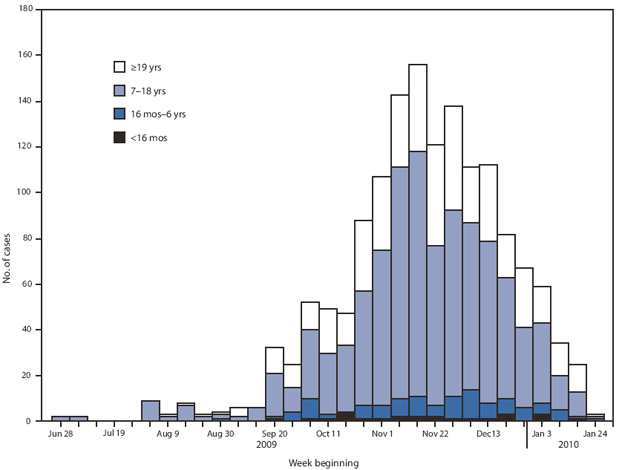
* Total cases reported: N = 1,521. Date of illness onset or age was missing for 27 cases (date of onset missing for 25 cases, age for two cases, and both date and age for one case).
† Case definitions available at http://www.cdc.gov/ncphi/disss/nndss/casedef/mumps_2008.htm.
§ Case total with onset date through January 29, 2010. The outbreak is ongoing; the appearance of a downward trend in recent weeks is partly a result of reporting delays.
Alternate Text: The figure above shows the number (n = 1,494) of reported confirmed or probable mumps cases, by week of illness onset and age group in New York and New Jersey during an outbreak which occurred from June 2009 to January 2010. The 1,521 outbreak-related mumps cases were reported from several counties in New York and New Jersey; local transmission is continuing.
|
TABLE. Vaccination status of patients with confirmed or probable mumps,* by age group and number of mumps-containing vaccine doses received --- New York and New Jersey, June 2009--January 2010† |
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
No. of doses |
Age group |
Total |
||||||||||
|
<16 mos |
16 mos--6 yrs |
7--18 yrs |
≥19 yrs |
Unknown |
||||||||
|
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%) |
|
|
0 |
21 |
(80.8) |
32 |
(29.9) |
56 |
(6.0) |
30 |
(6.6) |
0 |
--- |
139 |
(9.1) |
|
1 |
3 |
(11.5) |
33 |
(30.8) |
72 |
(7.8) |
29 |
(6.4) |
0 |
--- |
137 |
(9.0) |
|
2 |
0 |
--- |
36 |
(33.6) |
713 |
(76.7) |
90 |
(19.7) |
0 |
--- |
839 |
(55.2) |
|
Unknown |
2 |
(7.7) |
6 |
(5.6) |
88 |
(9.5) |
307 |
(67.3) |
3 |
(100.0) |
406 |
(26.7) |
|
Total |
26 |
(100.0) |
107 |
(100.0) |
929 |
(100.0) |
456 |
(100.0) |
3 |
(100.0) |
1,521 |
(100.0) |
|
* Case definitions available at http://www.cdc.gov/ncphi/disss/nndss/casedef/mumps_2008.htm. † Case total with onset date through January 29, 2010. The outbreak is ongoing. |
||||||||||||
|
• Timely vaccination with 2 doses of measles, mumps, and rubella (MMR) vaccine. • High awareness among health-care providers that mumps can occur, even in communities with high 2-dose MMR vaccination coverage. • Ongoing surveillance and prompt reporting of mumps cases to public health officials. • Isolation of persons with suspected and confirmed mumps for 5 days after onset of parotitis. • In congregate settings such as colleges and schools where mumps can spread rapidly: early recognition, diagnosis, and public health intervention. • During outbreaks: 1 dose of MMR vaccine for adults and children whose vaccination status is unknown or who have not received the number of MMR doses recommended by the Advisory Committee on Immunization Practices; consideration of a second dose of MMR vaccine for children aged 1--4 years and adults who have received 1 dose (8). |
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
