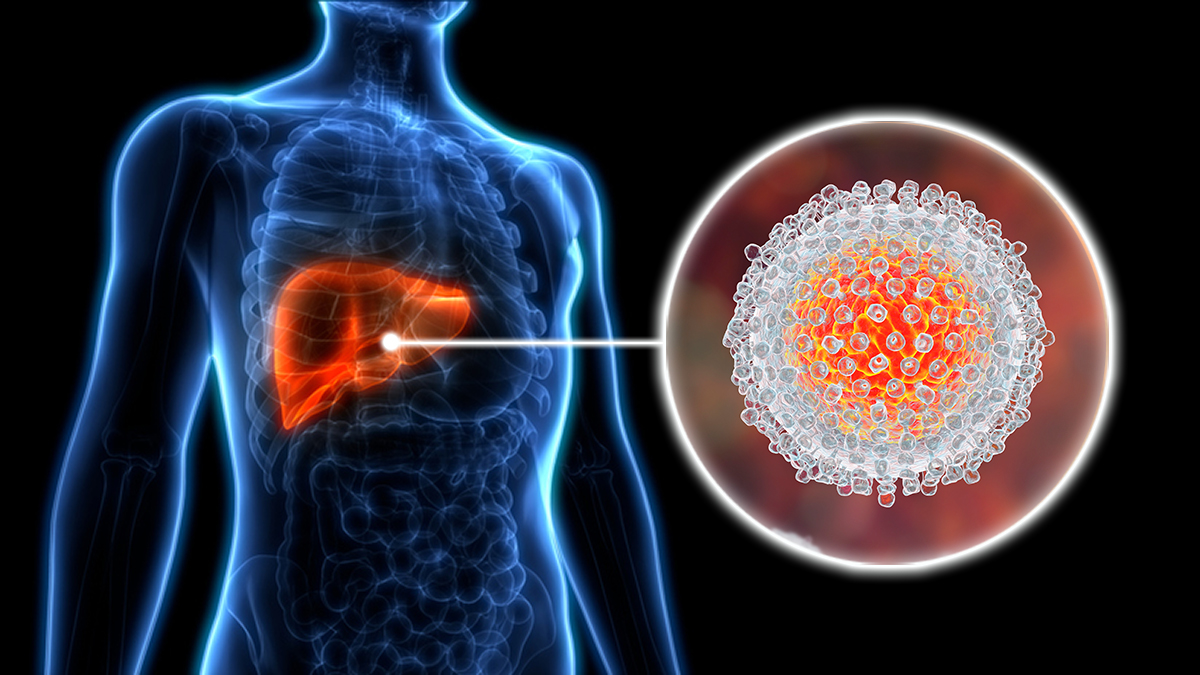
Learn the basics about hepatitis C, including symptoms, spread, testing, and treatment.

Learn about hepatitis C prevention, how hepatitis C spreads, and who is at risk of being infected.

Learn about hepatitis C symptoms and how hepatitis C symptoms can be mild or nonexistent.
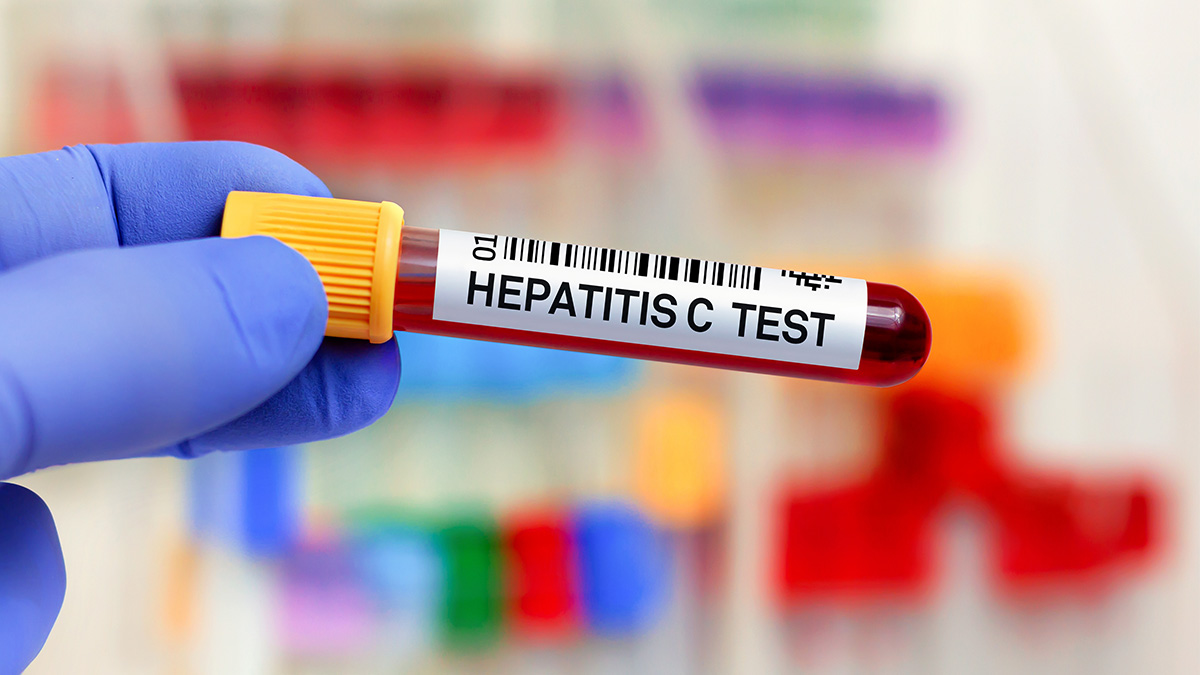
Learn about hepatitis C testing, who should be tested, and what kinds of tests are available.
For Professionals

For health professionals, find hepatitis C statistics, transmission, symptoms, and treatment info.

Find hepatitis resources for health pros, including fact sheets, online training, and guidelines.
Learn about hepatitis C symptoms, onset time, and how long they typically last.
Check CDC & USPSTF guidelines for hepatitis C screening among adults and the testing sequence.
Find guidelines for potential exposures to hepatitis C and outbreak prevention.
See the 2023 Viral Hepatitis Surveillance Report, published by CDC’s Viral Hepatitis Program
Healthcare-associated hepatitis B virus (HBV) and hepatitis C virus (HCV) outbreaks reported to CDC...
Viral Hepatitis

Learn about viral hepatitis, statistics, surveillance, resources, populations and impact.
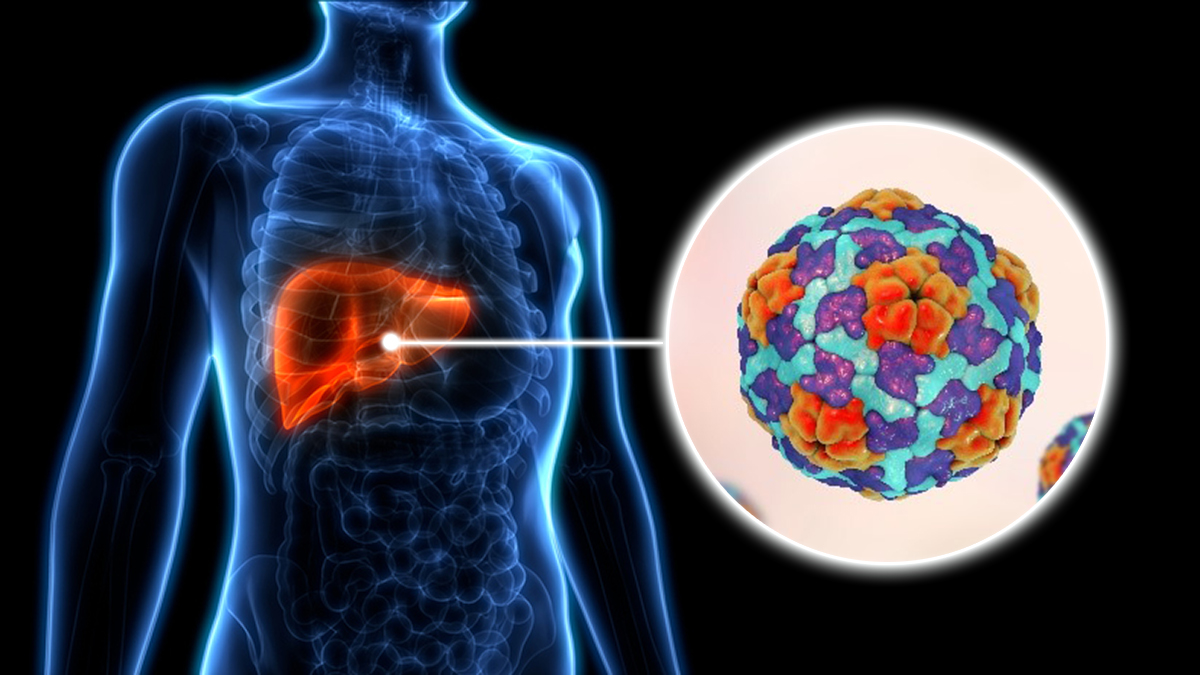
Learn about hepatitis A, including prevention, symptoms, and treatment.
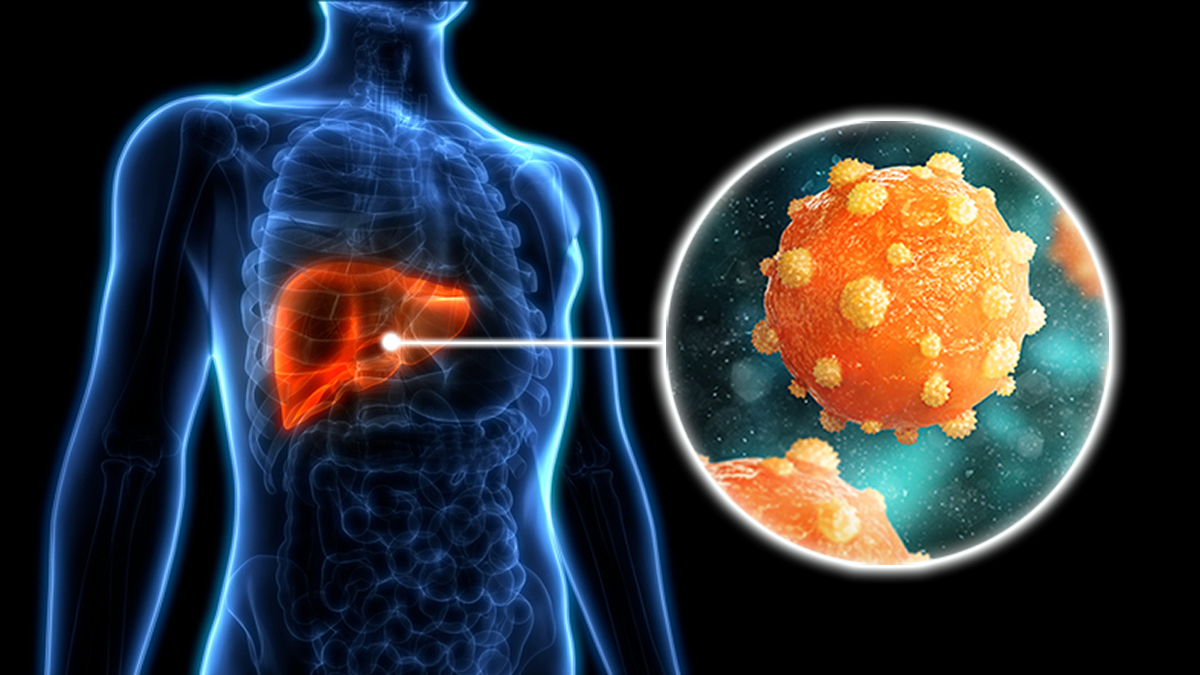
Learn more about hepatitis B, a vaccine-preventable liver infection caused by the hepatitis B virus.