|
TABLE. Annual drug overdose death rates* for selected substances --- Florida, 2003--2009 |
||||||||
|---|---|---|---|---|---|---|---|---|
|
Substance |
Year |
% change 2003 to 2009§ |
||||||
|
2003 |
2004 |
2005 |
2006 |
2007 |
2008 |
2009† |
||
|
Prescription drugs |
7.3 |
8.2 |
8.6 |
9.5 |
11.0 |
11.9 |
13.4 |
84.2 |
|
Benzodiazepines |
2.2 |
2.6 |
3.2 |
3.5 |
4.0 |
5.0 |
5.9 |
168.4 |
|
Alprazolam |
1.3 |
1.8 |
2.3 |
2.5 |
3.1 |
3.8 |
4.4 |
233.8 |
|
Opioid analgesics |
6.7 |
7.7 |
7.9 |
8.8 |
10.3 |
11.0 |
12.5 |
86.1 |
|
Oxycodone |
1.7 |
2.0 |
1.9 |
2.7 |
3.8 |
5.1 |
6.4 |
264.6 |
|
Methadone |
2.2 |
3.2 |
3.5 |
3.9 |
4.3 |
3.8 |
3.9 |
79.2 |
|
Hydrocodone |
1.1 |
1.3 |
1.2 |
1.3 |
1.4 |
1.5 |
1.4 |
34.9 |
|
Morphine |
1.3 |
1.2 |
1.4 |
1.2 |
1.4 |
1.6 |
1.6 |
26.2 |
|
Other prescription drugs¶ |
0.3 |
0.5 |
0.6 |
0.5 |
0.6 |
0.6 |
0.8 |
141.6 |
|
Illicit drugs |
4.3 |
4.4 |
4.9 |
5.1 |
5.1 |
4.1 |
3.4 |
-21.4 |
|
Heroin |
1.4 |
0.9 |
0.6 |
0.4 |
0.5 |
0.6 |
0.5 |
-62.2 |
|
Cocaine |
3.2 |
3.4 |
4.1 |
4.5 |
4.6 |
3.5 |
2.8 |
-10.8 |
|
Other illicit drugs** |
0.3 |
0.6 |
0.5 |
0.4 |
0.3 |
0.3 |
0.2 |
-4.1 |
|
Ethanol (alcohol) |
1.5 |
1.6 |
1.7 |
1.8 |
2.3 |
2.4 |
2.8 |
81.4 |
|
All substances†† |
10.6 |
11.7 |
12.1 |
13.1 |
14.3 |
14.6 |
15.7 |
47.5 |
|
* Per 100,000 population. Based on U.S. Census resident population estimates. Available at http://www.census.gov/popest/states/states.html. † The addition of buprenorphine, oxymorphone, and zolpidem to the list of monitored drugs resulted in small numbers of additional deaths in 2009, including 12 among all substances. § Except for cocaine (p = 0.06) and other illicit drugs (p = 0.9), all the changes from 2003 to 2009 were statistically significant (p<0.05). Percentage change might not match calculations based on table data because of rounding. ¶ Includes amphetamine, carisoprodol/meprobamate, ketamine, and zolpidem. ** Includes methamphetamine, inhalants, ecstasy, hallucinogens, and other illicit drugs. †† Many deaths had several drugs contributing to the death; thus, the sum of the rates in each column exceeds the total death rate. |
||||||||
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Drug Overdose Deaths --- Florida, 2003--2009
In the United States in 2007, unintentional poisonings were the second leading cause of injury death (after motor-vehicle crashes) (1); approximately 93% of all unintentional poisoning deaths were caused by drug poisoning, also known as drug overdose (2). From 1990 to 2001 in Florida, the nonsuicidal poisoning death rate increased 325% (3). To characterize recent trends in drug overdose death rates in Florida, CDC analyzed data from the Florida Medical Examiners Commission. This report summarizes the results of that analysis, which found that, from 2003 to 2009, the number of annual deaths in which medical examiner testing showed lethal concentrations of one or more drugs increased 61.0%, from 1,804 to 2,905, and the death rate increased 47.5%, from 10.6 to 15.7 per 100,000 population. During 2003--2009, death rates increased for all substances except cocaine and heroin. The death rate for prescription drugs increased 84.2%, from 7.3 to 13.4 per 100,000 population. The greatest increase was observed in the death rate from oxycodone (264.6%), followed by alprazolam (233.8%) and methadone (79.2%). By 2009, the number of deaths involving prescription drugs was four times the number involving illicit drugs. These findings indicate the need to strengthen interventions aimed at reducing overdose deaths from prescription drugs in Florida. Medical examiner records are a timely, population-based source for data regarding overdose deaths from specific drugs. The data in this report and subsequent analyses can be used to design and measure the effectiveness of interventions.
Florida has a system of regional state medical examiners whose jurisdiction includes all drug-related deaths. Drug overdose data were obtained for the period 2003--2009 from datasets of the Florida Medical Examiners Commission, which contain information on 34 types of drugs frequently abused, including ethanol (grain or beverage alcohol), prescription drugs, and illicit drugs (4). Drug-related deaths are divided into two categories: 1) drug-caused deaths, for which postmortem medical examiner toxicology testing determined that drugs were present in lethal amounts; and 2) drug-present deaths, for which drugs were found in nonlethal amounts. This analysis included only drug-caused deaths, referred to in this report as drug overdose deaths.
Using U.S. Census resident population estimates, annual drug overdose death rates per 100,000 population were calculated for all drugs, prescription drugs, illicit drugs (including specifically heroin and cocaine), opioid analgesics (including specifically methadone, hydrocodone, oxycodone, and morphine), benzodiazepines (including specifically alprazolam), and ethanol. To test for the statistical significance of changes in death rates from 2003 to 2009, z-tests were conducted in categories with annual counts >100, and examination of overlapping confidence intervals from gamma distributions was used with counts <100.
During 2003--2009, a total of 16,550 drug overdose deaths were recorded by Florida medical examiners. The annual number of deaths increased 61.0%, from 1,804 to 2,905, and the death rate increased 47.5%, from 10.6 to 15.7 per 100,000 population. In 2009, approximately eight drug overdose deaths occurred each day. During 2003--2009, 85.9% of drug overdose deaths were unintentional, 11.1% were suicides, 2.6% were of undetermined intent, and 0.4% were homicides or pending. Prescription medications were implicated in 76.1% of all drug overdose deaths, and illicit drugs were implicated in 33.9% of deaths; in 10.0% of deaths, both prescription and illicit drugs were found in lethal concentrations.
In 85.5% of all drug overdose deaths, at least one of the seven specific drugs examined in this study was detected at a lethal concentration. Analysis of drug-specific death rates revealed different trends for different drugs during 2003--2009 (Table, Figure).
The death rate for prescription drugs increased 84.2%, from 7.3 to 13.4 per 100,000 population from 2003 to 2009. The greatest increase in death rate was observed for the prescription drug oxycodone (264.6%), followed by alprazolam (233.8%), methadone (79.2%), hydrocodone (34.9%), and morphine (26.2%). Conversely, the death rate for heroin decreased 62.2% from 2003 to 2009, and the death rate for cocaine increased until 2007 and then decreased 39.1% from 2007 to 2009 (Table).
In 2003, among the seven specific drugs examined, the highest death rate was for cocaine (3.2 per 100,000 population), followed by methadone (2.2), oxycodone (1.7), heroin (1.4), morphine and alprazolam (1.3), and hydrocodone (1.1). In 2009, the number of deaths involving prescription drugs was four times the number involving illicit drugs, and the highest death rate was for oxycodone (6.4 per 100,00 population), followed by alprazolam (4.4), methadone (3.9), cocaine (2.8), morphine (1.6), hydrocodone (1.4), and heroin (0.5) (Figure).
Reported by
Bruce Goldberger, PhD, W.R. Maples Center for Forensic Medicine, Univ of Florida College of Medicine. Jon Thogmartin, MD, State of Florida District Six Medical Examiner. Hal Johnson, MPH, Substance Abuse Program Office, Florida Dept of Children and Families. Leonard Paulozzi, MD, Rose Rudd, MSPH, Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control; Aybaniz Ibrahimova, MD, EIS Officer, CDC. Corresponding contributor: Leonard Paulozzi, lpaulozzi@cdc.gov.
Editorial Note
This report documents an increasing problem with fatal overdoses of prescription drugs, based on Florida medical examiner data, which are more timely and specific than national data available from death certificates. Recent national data indicate increasing numbers of deaths involving opioid analgesics and cocaine through 2006 (5). This report indicates a worsening problem in Florida with overdoses involving prescription drugs, especially oxycodone and alprazolam, and a recent sharp decline in cocaine-related deaths. Large national increases in rates of emergency department visits involving oxycodone and alprazolam occurred during 2004--2009 (6).
Similar recent changes in drug-specific death counts have been reported by the Office of the State Medical Examiner in Kentucky. From 2007 to 2009, the number of deaths involving oxycodone in Kentucky doubled, the number involving alprazolam increased tenfold, and the numbers involving cocaine or methadone declined (7). Whether these specific trends with oxycodone and alprazolam are nationwide, regional, or indicative of common risk factors in Florida and Kentucky is unknown.
Since 2007, Florida has seen the proliferation of hundreds of pain clinics that prescribe large quantities of oxycodone and alprazolam, some of which is ultimately used for nonmedical purposes. Many of the customers of such clinics reportedly reside in Appalachian states such as Kentucky, and travel to Florida to obtain drugs for resale in their home states (8). In 2009, Florida passed legislation establishing standards for pain management clinics (9). The new legislation established more stringent licensure requirements, put a limit on the amount that could be prescribed when patients pay cash, and required tamper-resistant prescription forms. The impact of this legislation has not yet been determined. The dispensing of frequently abused prescription drugs, such as opioid analgesics and benzodiazepines, by pharmacies can be tracked using state prescription drug monitoring programs, now operational in 35 states (10). However, Florida does not yet have an operational prescription drug monitoring program.
The findings in this report are subject to at least five limitations. First, the analysis did not include all drug overdose deaths in Florida because the Florida Medical Examiners Commission collects data only on frequently abused drugs. Second, the death rates did not include Florida residents who died out of state but did include a small number of nonresidents who died in Florida. Third, reporting of deaths might have been incomplete from some medical examiner jurisdictions. Fourth, a few drugs were included in 2009 totals that were not tracked during 2003--2008. Finally, although the availability and scope of toxicologic testing were unchanged during 2003--2009, testing protocols among the nine laboratories in Florida providing the service are not standardized.
To address the increase in drug overdose deaths from prescription drugs, states need to implement surveillance systems that are able to track patterns of drug use and the impact of prevention measures. In addition, tighter regulation of pain clinics in all states might be necessary to prevent the migration of unethical clinics to jurisdictions without adequate regulation. Controls placed on wholesale distributors of frequently abused prescription drugs might prevent them from supplying unethical pain clinics. State and urban medical examiners can publish drug-specific overdose statistics to improve the timeliness of drug mortality surveillance.
References
- CDC. Web-based Injury Statistics Query and Reporting System (WISQARS). Available at http://www.cdc.gov/injury/wisqars/index.html. Accessed June 30, 2011.
- CDC. CDC Wide-Ranging Online Data for Epidemiologic Research (WONDER). Available at http://wonder.cdc.gov. Accessed June 30, 2011.
- CDC. Unintentional and undetermined poisoning deaths---11 states, 1990--2001. MMWR 2004;53:233--8.
- Florida Department of Law Enforcement. Drugs identified in deceased persons by Florida medical examiners. Tallahassee, FL: Florida Department of Law Enforcement; 2010. Available at http://www.fdle.state.fl.us/content/getdoc/036671bc-4148-4749-a891-7e3932e0a483/publications.aspx. Accessed June 30, 2011.
- Warner M, Chen LH, Makuc DM. Increase in fatal poisonings involving opioid analgesics in the United States, 1999--2006. NCHS data brief No. 22. Hyattsville, MD: US Department of Health and Human Services, CDC, National Center for Health Statistics; 2009. Available at http://www.cdc.gov/nchs/data/databriefs/db22.htm. Accessed July 6, 2011.
- Office of Applied Studies, Substance Abuse and Mental Health Services Administration. The DAWN report: highlights of the 2009 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2010. Available at http://oas.samhsa.gov/2k10/dawn034/edhighlights.cfm. Accessed June 30, 2011.
- Office of the Medical Examiner. 2009 calendar year annual report. Louisville, KY: Office of the Medical Examiner; 2010.
- Satz MJ. Interim report of the Broward County Grand Jury: the proliferation of pain clinics in South Florida. Ft. Lauderdale, FL: Seventeenth Judicial Circuit; 2009. Available at http://sao17.state.fl.us/pill%20mill%20grand%20jury.pdf. Accessed June 30, 2011.
- Florida Department of Health. Pain clinic registration. Tallahassee, FL: Florida Department of Health; 2011. Available at http://www.doh.state.fl.us/mqa/medical/me_pain.html. Accessed June 30, 2011.
- Alliance of States with Prescription Monitoring Programs. About the Alliance. Available at http://www.pmpalliance.org/node/2. Accessed July 6, 2011.
What is already known on this topic?
In the United States in 2007, unintentional poisonings were the second leading cause of injury death. Approximately 93% of all unintentional poisoning deaths were caused by drug overdose. From 1990 to 2001 in Florida, the nonsuicidal poisoning death rate increased 325%.
What is added by this report?
The death rate from overdoses of prescription drugs in Florida increased 84.2% from 2003 to 2009, whereas the death rate from heroin overdose declined 62.2% and the death rate from cocaine overdose increased until 2007 and then declined 39.1% from 2007 to 2009. Among prescription drugs, the death rates for oxycodone and alprazolam increased 264.6% and 233.8%, respectively.
What are the implications for public health practice?
To address the increase in drug overdose deaths caused by prescription drugs, regulatory and public health agencies can implement surveillance systems that are able to count drug overdoses, describe patterns of drug use, and assess the impact of drug overdose prevention measures.
FIGURE. Annual drug overdose death rates* for selected prescription and illicit drugs --- Florida, 2003--2009
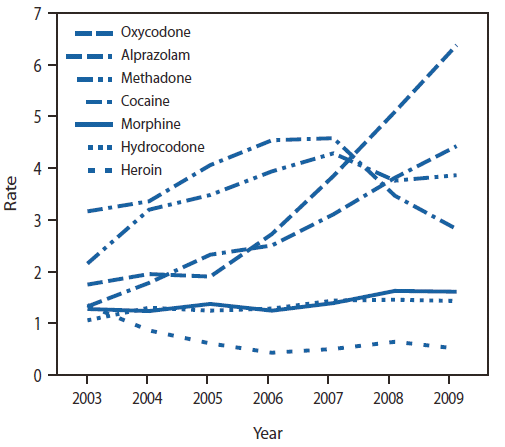
* Per 100,000 population. Based on U.S. Census resident population estimates. Available at http://www.census.gov/popest/states/states.html.
Alternate Text: The figure above shows the annual drug overdose death rates for selected prescription and illicit drugs in Florida for 2003-2009. Among seven specific drugs examined, in 2003 the highest death rate was for cocaine (3.2 per 100,000 population), followed by methadone (2.2), oxycodone (1.7), heroin (1.4), morphine and alprazolam (1.3), and hydrocodone (1.1). In 2009, the number of deaths involving prescription drugs was four times the number involving illicit drugs, and the highest death rate was for oxycodone (6.4 per 100,00 population), followed by alprazolam (4.4), methadone (3.9), cocaine (2.8), morphine (1.6), hydrocodone (1.4), and heroin (0.5).
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
