Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Infant Lead Poisoning Associated with Use of Tiro, an Eye Cosmetic from Nigeria — Boston, Massachusetts, 2011
Lead is highly toxic and can damage the brain, kidneys, bone marrow, and other body systems; high levels can cause convulsions, coma, and death (1). Young children are especially susceptible to lead exposures because of their floor-hand-mouth activity, greater gut absorption, and developing central nervous systems. In June 2011, a male infant aged 6 months of Nigerian descent was referred to the Pediatric Environmental Health Specialty Unit (PEHSU) at Boston Children's Hospital because of an elevated blood lead level (BLL). An investigation found no lead exposure except for "tiro," a Nigerian cosmetic that also is used as a folk remedy to promote visual development. The tiro applied to the infant's eyelids contained 82.6% lead. Products similar to tiro, such as "surma" and "kajal" in Asia and kohl in the Middle East, also might contain lead. This case adds to the medical literature documenting nonpaint lead sources as causes of elevated BLLs in children (2,3) and highlights persons of certain immigrant populations as a risk group. Educational efforts are needed to inform immigrants from Africa, Asia, and the Middle East that tiro and similar products can cause lead poisoning in children. Health-care providers and public health workers should ask about eye cosmetics and folk remedies when seeking a source of exposure in children with elevated BLLs from certain immigrant populations.
In June 2011, during a well-child visit of a male infant aged 6 months born in the United States to Nigerian parents, the physician noted that an imported cosmetic had been applied to the child's eyelids. Capillary blood testing performed by the physician indicated a BLL of 13 µg/dL, more than twice the CDC's reference value of 5 µg/dL, based on the 97.5th percentile of the BLL distribution in U.S. children aged 1–5 years. The next day, a confirmatory venous BLL measured by graphite furnace atomic absorption spectroscopy was 12 µg/dL. Additional laboratory evaluation revealed a normal hemoglobin level and 2+ erythrocyte microcytosis on an automated blood smear. In accordance with CDC recommendations aimed to help reduce the absorption of lead and mitigate the severe adverse health effects of lead exposure,* the pediatrician prescribed supplemental iron, contacted the Massachusetts Department of Public Health, and referred the family to the regional PEHSU.
When the infant was brought to the PEHSU 1 week later, his venous BLL, as measured by the same laboratory, was 13 µg/dL. His whole blood zinc protoporphyrin (30 µg/dL whole blood [normal: 0–35 µg/dL]), hemoglobin (12.1 g/dL [normal: 10.4–12.5 g/dL]), erythrocyte mean cell volume (74.2 fL [normal: 68.0–83.1 fL]), plasma iron (81 µg/dL [normal: 40–100 µg/dL]), and ferritin (65.0 ng/mL [normal: 10.0–75.0 ng/mL]) were in the normal range for his age. A manual blood smear showed 2+ erythrocyte microcytosis. The parents reported no health concerns for the infant, and a detailed review of systems was normal. The infant had no relevant past medical history, was growing well, and had met all developmental milestones. No other children lived in the home. Both parents had sickle cell trait; the infant had a normal hemoglobin electrophoresis. No abnormalities were noted on the physical examination.
Since 2008, the family had lived in a townhouse originally built in 2004. PEHSU staff members inspected the residence and found it to be in excellent condition, without lead hazards. Other sources of lead exposure were ruled out, including take-home exposure from parental occupations, kitchenware, family hobbies, and diet. The infant was breastfed exclusively and did not consume any imported herbs, spices, or dietary supplements. Additional questioning revealed that since age 2 weeks, a Nigerian cosmetic and folk remedy had been applied to the infant's eyelids three to four times weekly to improve attractiveness and promote visual development. A grandparent had purchased the powder, called tiro (Figure 1), from a street vendor in Ilorin, a city in Kwara State, Nigeria. The PEHSU recommended immediately discontinuing the use of tiro on the infant and continuing iron supplementation. The parents agreed to submit the suspected tiro powder for laboratory analysis.
Quantitative analysis by the PEHSU showed that the tiro consisted of 82.6% lead. A single application of 10 mg of tiro would deliver 8 mg of lead to the infant's eyelids. The most likely routes of exposure were eyelid-hand-mouth and absorption from the conjunctival surfaces of the eyes or in ingested tears. Analysis of the tiro by the U.S. Geological Survey, using scanning electron microscopy (SEM), showed that the sample was dominated by lead sulfide, known as galena (Figure 2), which has relatively low bioavailability (1). No other minerals were observed by SEM, although small amounts of other minerals commonly found as microscopic inclusions in lead sulfide might have escaped detection.
Three months after the family stopped applying tiro to the infant's eyelids, his venous BLL had fallen from 13 µg/dL to 8 µg/dL.
Reported by
Abdulsalami Nasidi, MD, Nigeria Centre for Disease Control. Mateusz Karwowski, MD, Alan Woolf, MD, Pediatric Environmental Health Specialty Unit; Mark Kellogg, PhD, Terence Law, Dept of Laboratory Medicine, Boston Children's Hospital, Boston, Massachusetts. Marissa Scalia Sucosky, MPH, Rose M. Glass-Pue, MA, Mary Jean Brown, ScD, Div of Emergency and Environmental Health Svcs, National Center for Environmental Health; Behrooz Behbod, MBChB, EIS Officer, CDC. Corresponding contributor: Behrooz Behbod, bbehbod@cdc.gov, 770-488-0788.
Editorial Note
Although the primary source of lead exposure in the United States is lead-based paint, nonpaint sources of lead increasingly are being identified in lead poisoning cases (2,3). These nonpaint exposures include recent travel to a foreign country, take-home exposure when persons exposed to lead at their workplace contaminate their homes or vehicles, and use of imported products such as spices, food, candy, cosmetics, health remedies, ceramics or pottery, and jewelry.
This report describes an eye cosmetic and folk remedy as the source of lead poisoning in a child of Nigerian descent; a similar case has been reported in the United Kingdom (4,5). Although Nigeria switched to unleaded gasoline by the end of 2003, Nigerian children might also be exposed to the lead that remains in the soil from years of use of leaded gasoline. In addition, lead contamination resulting from gold mining has caused many child deaths in Nigerian villages where artisanal gold ore processing takes place (6,7).
Tiro is the Yoruba name for this eye cosmetic implicated in the case described in this report. In another Nigerian language, Hausa, it is called "tozali" or "kwalli." Similar products intended to darken the eyes are known as kohl in English and Arabic and as "surma" or "kajal" in languages spoken in India and Pakistan. These preparations are not standardized, and not all contain lead. One alternative to lead sulfide is another toxic compound, antimony sulfide. Imported cosmetics are one of the relatively few sources of significant lead exposure for infants too young to crawl or walk; however, exposure to lead in tiro represents an additional burden to groups who might be exposed to other sources of lead. The contribution that tiro might make to the cumulative burden of lead poisoning should not be overlooked.
This fine powder is applied to the dermal surfaces of the eyelid. In addition to its use by the patient's family for improving attractiveness and promoting visual development, tiro has been used to ward off "the evil eye"; to relieve eyestrain, pain, or soreness; to prevent infection of the umbilical stump or a circumcision wound by local application; and to prevent sun glare (8,9).
This case identifies tiro as a potential lead exposure among not only Nigerians living in the United States, but also among African, Asian, and Middle Eastern populations who use similar products. Public health educational campaigns can help identify and prevent further cases (10).† Obstetricians, pediatricians, midwives, and allied health-care professionals should discuss this potential risk factor during prenatal and early childhood medical visits by families for whom these cultural practices might apply. Although CDC recommends blood lead testing for internationally adopted and refugee children,§ blood lead testing in children of certain immigrant populations also might be important because of the increased risk for exposure to lead-containing foreign products.
The Nigeria Centre for Disease Control is working with the vendors of products such as tiro to find possible safer alternatives. Discussions involve the perceived benefit of tiro, and evidently, strong beliefs are attached to its use. The Nigeria Centre for Disease Control plans to launch a national public health awareness campaign.
Acknowledgment
Geoffrey S. Plumlee, PhD, US Geological Survey, Crustal Geophysics and Geochemistry Science Center, Denver, Colorado.
References
- Agency for Toxic Substances and Disease Registry. Toxicological profile for lead. Atlanta, GA: US Department of Health and Human Services, CDC, Agency for Toxic Substances and Disease Registry; 2007. Available at http://www.atsdr.cdc.gov/toxprofiles/tp13.pdf. Accessed July 26, 2012.
- Gorospe EC, Gerstenberger SL. Atypical sources of childhood lead poisoning in the United States: a systematic review from 1966–2006. Clin Toxicol (Phila) 2008;46:728–3.
- CDC. Childhood lead poisoning associated with tamarind candy and folk remedies—California, 1999–2000. MMWR 2002;51:684–6.
- Warley MA, Blackledge P, O'Gorman P. Lead poisoning from eye cosmetic. Brit Med J 1968;1:117.
- Healy MA, Aslam M, Bamgboye OA. Traditional medicine and lead-containing preparations in Nigeria. Public Health 1984;98:26–32.
- CDC. Notes from the field: Outbreak of acute lead poisoning among children aged <5 years—Zamfara, Nigeria, 2010. MMWR 2010;59:846.
- Dooyema CA, Neri A, Lo YC, et al. Outbreak of fatal childhood lead poisoning related to artisanal gold mining in northwestern Nigeria, 2010. Environ Health Perspect 2012;120:601–7.
- Al-Hawi SA, Wafai MZ, Kalaagi MR, Al-Ugum WA. Light of the eyes and the collector of arts, vol. 1286. Riyadh, Saudi Arabia: King Faisal Center for Research and Islamic Studies; 1980:142.
- Hardy AD, Vaishnav R, Al-Kharusi SSZ, Sutherland HH, Worthing MA. Composition of eye cosmetics (kohls) used in Oman. J Ethnopharmacol 1998;60:223–34.
- Woolf AD, Hussain J, McCullough L, Petranovic M, Chomchai C. Infantile lead poisoning from an Asian tongue powder: a case report & subsequent public health inquiry. Clin Toxicol (Phila) 2008;46:841–4.
* Recommendations available at http://www.cdc.gov/nceh/lead/casemanagement/casemanage_chap4.htm.
† Examples of such campaigns are described at http://www.nyc.gov/html/doh/html/lead/lead-import-eyecos.shtml.
§ Guidelines available at http://www.cdc.gov/nceh/lead/tips/populations.htm.
What is already known on this topic?
Although the most common source of lead poisoning for young children in the United States is lead-based paint, nonpaint sources of lead are being identified increasingly in lead poisoning cases, particularly in immigrant communities.
What is added by this report?
A male infant aged 6 months was found to have an elevated blood lead level (BLL) attributed to application of "tiro," a Nigerian eye cosmetic, to his eyes by his parents. Tiro, also known as "tozali" and "kwalli" in Nigeria, is similar to kohl, "surma," and "kajal" used in the Middle East, India, and Pakistan. These products often are made with lead. In this case, the lead content was 82.6%. This case adds to the medical literature documenting nonpaint lead sources as causes of elevated BLLs in children and highlights persons of certain immigrant populations as a risk group.
What are the implications for public health practice?
Educational and other primary prevention efforts are needed to inform immigrants from Africa, Asia, and the Middle East that tiro and similar products can cause lead poisoning in children. Health-care providers and public health workers should ask about eye cosmetics and folk remedies when seeking a source of exposure in children with elevated BLLs from certain immigrant populations.
FIGURE 1. The Nigerian tiro container and the powder that was applied to the lead-poisoned child's eyelids — Boston, Massachusetts, 2011

Photo/Pediatric Environmental Health Specialty Unit, Boston Children's Hospital
Alternate Text: The figure above shows the Nigerian tiro container and the powder that was applied to the lead-poisoned child's eyelids in Boston, Massachusetts, in 2011.
FIGURE 2. Scanning electron microscopy* of the tiro eye cosmetic powder that was applied to the lead-poisoned child's eyelids, revealing the presence of cubic shapes and stair-step cleavage, both of which indicate presence of lead sulfide (also known as galena) — Boston, Massachusetts, 2011
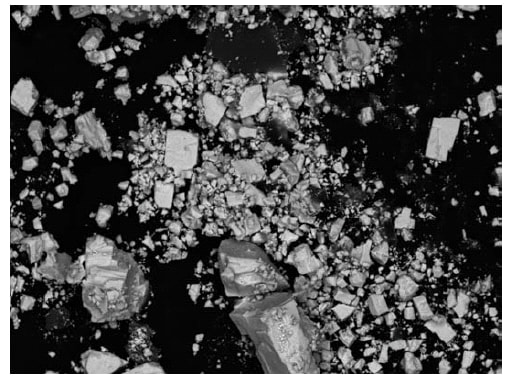
Photo/U.S. Geological Survey, Crustal Geophysics and Geochemistry Science Center
* Field of view is approximately 100 µm wide.
Alternate Text: The figure above shows scanning electron microscopy of the tiro eye cosmetic powder that was applied to the lead-poisoned child's eyelids in Boston, Massachusetts, during 2011, revealing the presence of cubic shapes and stair-step cleavage, both of which indicate presence of lead sulfide. Analysis of the tiro by the U.S. Geological Survey, using scanning electron microscopy, showed that the sample was dominated by lead sulfide, which has relatively low bioavailability.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
