Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Influenza-Associated Pediatric Deaths --- United States, September 2010--August 2011
Influenza-associated pediatric mortality has been a nationally notifiable condition since October 2004. This report summarizes the 115 cases of influenza-associated pediatric mortality reported to CDC that occurred from September 1, 2010, through August 31, 2011. Deaths occurred in 33 states. Nearly half of the deaths (46%) occurred in children aged <5 years. Of the children who died, 49% had no known Advisory Committee on Immunization Practices (ACIP)--defined* high-risk medical conditions, and 35% died at home or in the emergency department. Of the 74 children aged ≥6 months for whom vaccination data were available, 17 (23%) had been fully vaccinated. ACIP recommends that all children aged ≥6 months receive vaccination against influenza annually (1,2). These findings underscore the importance of vaccinating children to prevent influenza virus infection and its potentially severe complications. Health-care providers should develop a comprehensive strategy to increase vaccination coverage among children.
A case is defined as a death from a clinically compatible illness confirmed to be influenza by a diagnostic test in a U.S. resident aged <18 years, with no period of complete recovery between illness and death. Cases are identified by state and local health departments, which collect demographic, clinical, and laboratory information using a standard form and transmit the information to CDC via a secure, web-based interface for data entry. Confirmatory influenza testing methods include commercial rapid diagnostic tests, viral culture, fluorescent antibody, enzyme immunoassay, reverse transcription--polymerase chain reaction, and immunohistochemistry. Although influenza vaccination of women during pregnancy has been shown to be effective in reducing hospitalizations (1) and deaths among infants aged <6 months (3), data on maternal vaccination during pregnancy were not available for infants aged <6 months.
Of the 115 influenza-associated pediatric deaths reported, 72 (63%) occurred in males (Table). The majority of cases were in non-Hispanic white children (52%), followed by non-Hispanic black (18%) and Hispanic (15%) children. The highest numbers of deaths occurred in late January and early February 2011 (Figure 1). The median age of patients was 6 years, and 53 cases (46%) were in children aged <5 years (Table). Seventy-one (62%) of these cases were associated with influenza A virus infection: 30 (26%) 2009 influenza A (H1N1), 21 (18%) influenza A (H3N2), and 20 (18%) influenza A viruses for which the subtype was not determined. The remaining 44 (38%) cases were associated with influenza B virus infections. In comparison, U.S. national viral surveillance data from World Health Organization (WHO) and National Respiratory and Enteric Virus Surveillance System (NREVSS) collaborating laboratories indicated that 74% of circulating viruses were influenza A and 26% were influenza B viruses.†
Nearly half of the children who died (49%) had no known ACIP-defined high-risk medical conditions, 57 (50%) children were reported with medical conditions recognized by ACIP that placed them at increased risk for influenza-related complications, and the medical history of two children was unknown (2%) (Table). Of the 57 children with at least one ACIP-defined high-risk condition, 31 (54%) had a neurologic disorder, 17 (30%) had pulmonary disease, 14 (25%) had a chromosomal abnormality or genetic disorder, 11 (19%) had congenital heart disease or other cardiac disease, and 11 (19%) had asthma or reactive airway disease. Obesity was reported in two (4%) of the 57 children.
Information on the location of death was available for 114 children; 20 (18%) died outside the hospital, 20 (18%) died in the emergency department, and 74 (65%) died in the hospital after admission (Table). Duration of illness ranged from 0 to 57 days (Figure 2); 33 (31%) children died within 3 days of illness onset, and 69 (65%) died within 7 days. When compared with pediatric deaths among children with at least one ACIP-defined high-risk condition, children without high-risk conditions were significantly more likely to die at home or in the emergency department (p<0.01 by chi-square test). The median illness duration before death was 7 days among children with at least one ACIP-defined high-risk condition and 4 days among children without a high-risk condition (p<0.01 by Wilcoxon rank-sum test).
Of 64 children who had specimens collected for bacterial culture from normally sterile sites (including 58 blood cultures), 25 (39%) had positive cultures; Staphylococcus aureus was detected in nine (36%) patients (six with methicillin-resistant S. aureus, two with methicillin-sensitive S. aureus, and one with unknown sensitivity), Streptococcus pneumoniae was detected in six patients, and Group A streptococcus was detected in three. Of the 25 cases with positive cultures, 17 (68%) were in children without high-risk conditions. When compared with children with at least one ACIP-defined high-risk condition, children without a high-risk condition were significantly more likely to have a positive bacterial culture from a sterile site (p<0.01 by chi-square test).
The most frequent complications reported were radiographically confirmed pneumonia (62%), shock or sepsis (40%), and acute respiratory distress syndrome (34%). Encephalopathy or encephalitis was reported in 12 children (14%). The antiviral medications approved by the Food and Drug Administration (FDA) for treatment of influenza are oseltamivir for children aged ≥1 year and zanamivir for children aged ≥7 years (4). Of the 47 children who received antiviral therapy, three (6%) died in the emergency department, and 44 (94%) died after being admitted to the hospital. All three children who died in the emergency department received oseltamivir. Of the children who died after being admitted to the hospital, 41 received oseltamivir only, two received oseltamivir and zanamivir, and one received zanamivir only.
Information about influenza vaccination was available for 74 children aged ≥6 months; 17 (23%) received influenza vaccine in the appropriate number of doses at least 14 days before illness onset. Of 39 vaccine-eligible children with ACIP-defined high-risk medical conditions who had vaccination data available, 12 (31%) had been vaccinated according to 2010 ACIP recommendations (1).
Reported by
World Health Organization Collaborating Center for Surveillance, Epidemiology, and Control of Influenza. Lenee Blanton, MPH, Rosaline Dhara, MPH, Lynnette Brammer, MPH, Joseph Bresee, MD, Nancy Cox, PhD, Lyn Finelli, DrPH, Influenza Div, National Center for Immunization and Respiratory Diseases; Karen K. Wong, MD, EIS officer, CDC. Corresponding contributor: Karen K. Wong, CDC, kwong@cdc.gov, 404-639-3747.
Editorial Note
Nearly half of the children who died from influenza virus infections during the 2010--11 influenza season and whose deaths were reported to CDC had no known ACIP-defined high-risk medical conditions. Of children with ACIP-defined high-risk medical conditions, neurologic disorders and pulmonary disease were identified most frequently. The underlying reason for the vulnerability of patients with neurologic disorders remains unclear but likely is attributable, in part, to compromised respiratory function and decreased ability to handle secretions (5). These data are consistent with findings from the 2004--05 through 2008--09 influenza seasons (5--7). Children with no high-risk conditions had a shorter interval between illness onset and death (4 days versus 7 days), and were more likely to die at home or in the emergency department, and were more likely to have a positive bacterial culture from a sterile site. In children with no high-risk conditions, the development of a secondary bacterial coinfection might have been the immediate cause for seeking medical care. Physicians of children with ACIP-defined high-risk conditions might have been more likely to hospitalize their patients early in their illness, given their perceived greater risk of influenza-related complications. Health-care providers should be aware that severe complications of influenza can occur in children without high-risk medical conditions. Information for parents, including guidance on influenza vaccination and danger signs in children with influenza-like illness symptoms, is available at http://www.cdc.gov/flu/pdf/freeresources/family/a_flu_guide_for_parents.pdf.
This report highlights several important points about influenza epidemiology, vaccination, and treatment in children. Although influenza-associated pediatric mortality is rare, influenza B was identified in a disproportionate number of pediatric influenza-associated deaths (38%). During the 2010--11 influenza season, only 26% of circulating influenza viruses were influenza B. In previous seasons, the percentage of influenza B viruses among children with influenza-associated mortality has been comparable to or higher than the percentage of influenza B viruses circulating for that season (6,7).
Annual influenza vaccination for all children aged ≥6 months is recommended and is the most effective way to prevent influenza and its complications. Influenza vaccination campaigns should proceed for all persons (children and adults) as soon as vaccine is available. Since 2010, ACIP has recommended annual influenza vaccination for all persons aged ≥6 months, and children with ACIP-defined high-risk medical conditions should be specially targeted for vaccination (1,2). Healthy children aged 2--18 years may receive either live, attenuated influenza vaccine (LAIV) or trivalent inactivated influenza vaccine (TIV) (1). Children aged 6--23 months and those aged 2--4 years who have asthma or wheezing, or who have medical conditions that put them at higher risk for influenza complications should receive TIV (1). Children aged 6 months--8 years who did not receive at least 1 dose of the 2010--11 seasonal influenza vaccine should receive 2 doses of the 2011--12 seasonal influenza vaccine administered at least 4 weeks apart. Children in this age group who did receive at least 1 dose of the 2010--11 vaccine, as well as persons aged ≥9 years, should receive 1 dose of the 2011--12 vaccine (2).
In the United States, influenza vaccination coverage for the 2010--11 season was estimated at 49% in children aged 6 months--17 years.§ Among children who died from influenza described in this report, 23% were vaccinated. Vaccination coverage was higher among children with ACIP-defined high-risk medical conditions than among children without high-risk medical conditions (31% versus 12%). These findings emphasize the need to improve vaccination coverage among all children, especially those at increased risk for influenza-related complications. To protect infants aged <6 months who are too young to be vaccinated, ACIP recommends that pregnant women (3) and household contacts and out-of-home caregivers of such infants receive vaccination against influenza (1). Because influenza vaccination of women during pregnancy has been shown to be effective in reducing hospitalizations (1) and deaths among infants aged <6 months (3), improving vaccination rates among pregnant women is a priority.
Half of the children described in this report received influenza antiviral therapy. Early and aggressive treatment with oseltamivir or zanamivir¶ is recommended as soon as possible after symptom onset in a patient with confirmed or suspected influenza who is hospitalized; who has severe, complicated, or progressive illness; or who is at higher risk for influenza complications,** even if influenza testing is negative (4). In outpatients without risk factors for complications, influenza antiviral treatment should be considered if treatment can be initiated within 48 hours of symptom onset. Results of one randomized, controlled trial of oseltamivir treatment among children aged 1--3 years indicated that when oseltamivir was started within 24 hours of illness onset, the median time to illness resolution was shortened by 3.5 days compared with placebo (8). Treatment with influenza antiviral therapy of any person with confirmed or suspected influenza who requires hospitalization is recommended, even if the patient enters care >48 hours after illness onset (4,9). S. aureus, S. pneumoniae, and Group A streptococcus were the pathogens most commonly identified in children with invasive bacterial coinfection. Empiric antibiotic therapy and early influenza antiviral therapy are recommended in patients with community-acquired pneumonia and suspected influenza coinfection (4). In 2010, ACIP recommended the use of the 13-valent pneumococcal polysaccharide-protein conjugate vaccine for all children aged 2--59 months and children aged 60--71 months with underlying medical conditions that increase their risk for pneumococcal disease or complications (10).
The findings in this report are subject to at least four limitations. First, the actual burden of influenza-associated pediatric mortality likely is underestimated because the current surveillance method will only detect those patients who are tested for influenza, who have a positive test, and who are reported to the surveillance system. Second, some data about medical conditions, vaccination status, clinical course, and treatment were missing; these data depend on the thoroughness and consistency of case reporting. Third, invasive bacterial testing is not performed systematically for all children and therefore depends on testing being part of clinical care or autopsy. Finally, determination of obesity as a high-risk medical condition did not use height and weight data, which might lead to underestimation of obesity among children.
This report emphasizes the importance of continued surveillance for influenza-associated pediatric mortality. State health departments should notify the Influenza Division at CDC of laboratory-confirmed influenza-associated pediatric deaths that occur in their jurisdiction as soon as possible by submitting the web-based case report form. Surveillance provides information about risk factors associated with severe disease and death that can be used to monitor the impact of influenza on children, plan interventions, inform policy and resource allocation decisions, develop vaccination recommendations, and provide information to public health professionals, the media, and the general public regarding the severity of the influenza season. Health-care providers should be mindful of the potential for severe outcomes of influenza in children. Although antiviral medications are a valuable adjunct to preventing and reducing the impact of influenza, vaccination remains the primary prevention tool against influenza-associated complications.
References
- CDC. Prevention and control of influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR 2010;59(No. RR-8).
- CDC. Prevention and control of influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2011. MMWR 2011;60:1128--32.
- Zaman K, Roy E, Arifeen SE, et al. Effectiveness of maternal influenza immunization in mothers and infants. N Engl J Med 2008;359:1555--64.
- CDC. Antiviral agents for the treatment and chemoprophylaxis of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2011;60(No. RR-1).
- Cox CM, Blanton L, Dhara R, Brammer L, Finelli L. 2009 pandemic influenza A (H1N1) deaths among children---United States, 2009--2010. Clin Infect Dis 2011;52(Suppl 1):S69--74.
- Peebles PJ, Dhara R, Brammer L, Fry AM, Finelli L. Influenza-associated mortality among children---United States: 2007--2008. Influenza Other Respi Viruses 2011;5:25--31.
- Finelli L, Fiore A, Dhara R, et al. Influenza-associated pediatric mortality in the United States: increase of Staphylococcus aureus coinfections. Pediatrics 2008;122:805--11.
- Heinonen S, Silvennoinen H, Lehtinen P, et al. Early oseltamivir treatment of influenza in children 1--3 years of age: a randomized controlled trial. Clin Infect Dis 2010;51:887--94.
- Harper SA, Bradley JS, Englund JA, et al. Seasonal influenza in adults and children---diagnosis, treatment, chemoprophylaxis, and institutional outbreak management: clinical practice guidelines of the Infectious Diseases Society of America. Clin Infect Dis 2009;48:1003--32.
- CDC. Prevention of pneumococcal disease among infants and children --- use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2010;59(No. RR-11).
* Children receiving long-term aspirin therapy who might be at risk for experiencing Reye syndrome after influenza virus infection or those with chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, hematologic, or metabolic disorders (including diabetes mellitus), and children with immunosuppression (including immunosuppression caused by medications or by human immunodeficiency virus) or any neurologic condition (e.g., cognitive dysfunction, spinal cord injuries, seizure disorders, or other neuromuscular disorders) that can compromise respiratory function or the handling of respiratory secretions or that can increase the risk for aspiration. Morbid obesity is a risk factor for adults.
† Data available at http://www.cdc.gov/flu/weekly.
§ Data available at http://www.cdc.gov/flu/professionals/vaccination/vaccinecoverage.htm.
¶ Oseltamivir is FDA-approved for treatment and chemoprophylaxis of influenza among children aged ≥1 year. Zanamivir is FDA-approved for treatment of influenza among children aged ≥7 years. Zanamivir is approved for chemoprophylaxis of influenza among children aged ≥5 years.
** Persons at higher risk include children aged <5 years (especially those aged <2 years); adults aged ≥65 years; persons with chronic pulmonary (including asthma), cardiovascular (except hypertension alone), renal, hepatic, hematologic (including sickle cell disease), metabolic disorders (including diabetes mellitus), or neurologic and neurodevelopment conditions (including disorders of the brain, spinal cord, peripheral nerve, and muscle, such as cerebral palsy, epilepsy [seizure disorders], stroke, intellectual disability [mental retardation], moderate to severe developmental delay, muscular dystrophy, or spinal cord injury); persons with immunosuppression, including that caused by medications or by human immunodeficiency virus infection; women who are pregnant or postpartum (within 2 weeks after delivery); persons aged ≤18 years who are receiving long-term aspirin therapy; American Indians/Alaska Natives; persons who are morbidly obese (i.e., body mass index ≥40); and residents of nursing homes and other chronic-care facilities.
What is already known on this topic?
Since influenza-associated pediatric deaths became a nationally notifiable condition in 2004, the number of deaths reported to CDC has ranged from 46 during the 2005--06 influenza season to 282 during the 2009--10 season.
What is added by this report?
A total of 115 influenza-associated pediatric deaths were reported to CDC that occurred from September 1, 2010 to August 31, 2011. Fifty-six (49%) children who died from influenza virus infections during the 2010--11 influenza season had no reported Advisory Committee on Immunization Practices (ACIP)--defined high-risk medical conditions. Children without high-risk conditions had a shorter interval between illness onset and death (4 days versus 7 days), were more likely to die at home or in the emergency department, and were more likely to have a positive bacterial culture from a sterile site. Among children who died from influenza, few (23%) were vaccinated, and 50% received antiviral therapy.
What are the implications for public health practice?
Continued efforts are needed to ensure annual influenza vaccination in all persons aged ≥6 months, and children with high-risk medical conditions should be specially targeted for vaccination. Health-care providers should be aware that severe complications of influenza can occur in children without high-risk medical conditions. Early and aggressive treatment with oseltamivir or zanamivir is recommended as soon as possible after symptom onset in patients with confirmed or suspected influenza who are hospitalized; who have severe, complicated, or progressive illness; or who are at a higher risk for influenza complications.
|
TABLE. (Continued) Number and percentage of children who died from influenza-associated illness (N = 115), by selected characteristics --- United States, September 1, 2010--August 31, 2011 |
||
|---|---|---|
|
Characteristic |
No. |
(%) |
|
Location of death§ |
||
|
Outside hospital (i.e., at home or in transit) |
20 |
(18) |
|
Emergency department |
20 |
(18) |
|
Hospital, admitted¶ |
74 |
(65) |
|
Duration of disease (days)** |
6 (0--57) |
|
|
Duration of disease ≤3 |
33 |
(31) |
|
Duration of disease ≤7 |
69 |
(66) |
|
≥1 high-risk condition, median (range) |
7 (0--57) |
|
|
No high-risk condition, median (range) |
4 (0--21) |
|
|
Bacterial testing from sterile site performed |
||
|
Yes |
64 |
(56) |
|
No |
43 |
(37) |
|
Unknown |
8 |
(7) |
|
≥1 bacterial coinfection†† |
25 |
(39) |
|
Bacteria isolated from sterile site§§ |
||
|
Staphylococcus aureus |
9 |
(36) |
|
Methicillin-resistant S. aureus |
6 |
(24) |
|
Methicillin-sensitive S. aureus |
2 |
(8) |
|
Sensitivity testing not performed |
1 |
(4) |
|
Streptococcus species¶¶ |
||
|
Streptococcus pneumoniae |
6 |
(24) |
|
Group A streptococcus |
3 |
(12) |
|
Group B streptococcus |
2 |
(8) |
|
Group C streptococcus, beta hemolytic |
1 |
(4) |
|
Group D streptococcus, non-hemolytic |
1 |
(4) |
|
Viridans group streptococcus*** |
2 |
(8) |
|
Other or not specified streptococcus††† |
2 |
(8) |
|
Pseudomonas aeruginosa |
2 |
(8) |
|
Complications during acute illness |
||
|
Yes |
85 |
(74) |
|
No |
19 |
(17) |
|
Unknown |
11 |
(10) |
|
Complications§§§ |
||
|
Pneumonia |
53 |
(62) |
|
Shock or sepsis |
34 |
(40) |
|
Acute respiratory distress syndrome |
29 |
(34) |
|
Other complication |
19 |
(22) |
|
Encephalopathy/Encephalitis |
12 |
(14) |
|
Seizures |
11 |
(13) |
|
Hemorrhagic pneumonia/pneumonitis |
5 |
(6) |
|
Croup |
4 |
(5) |
|
Cardiomyopathy/Myocarditis |
3 |
(4) |
|
Bronchiolitis |
2 |
(2) |
|
Received antibiotic therapy¶¶¶ |
49 |
(52) |
|
Received antiviral therapy¶¶¶ |
47 |
(50) |
|
Received oseltamivir |
46 |
(49) |
|
Received zanamivir |
3 |
(3) |
|
TABLE. (Continued) Number and percentage of children who died from influenza-associated illness (N = 115), by selected characteristics --- United States, September 1, 2010--August 31, 2011 |
||
|---|---|---|
|
Characteristic |
No. |
(%) |
|
Vaccination status |
||
|
Ineligible for vaccine |
16 |
(14) |
|
Eligible for vaccine |
99 |
(86) |
|
Fully vaccinated**** |
17 |
(23) |
|
Not vaccinated**** |
57 |
(77) |
|
Eligible for vaccine, ≥1 ACIP-defined high-risk condition†††† |
||
|
Fully vaccinated |
12 |
(31) |
|
Not fully vaccinated |
27 |
(69) |
|
Eligible for vaccine, no ACIP-defined high-risk condition†††† |
||
|
Fully vaccinated |
4 |
(12) |
|
Not fully vaccinated |
30 |
(88) |
|
Unknown vaccination status |
25 |
(22) |
|
Abbreviation: ACIP = Advisory Committee on Immunization Practices. * Children receiving long-term aspirin therapy who might be at risk for experiencing Reye syndrome after influenza virus infection or those with chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic, hematologic, or metabolic disorders (including diabetes mellitus), and children with immunosuppression (including immunosuppression caused by medications or by human immunodeficiency virus) or any neurologic condition (e.g., cognitive dysfunction, spinal cord injuries, seizure disorders, or other neuromuscular disorders) that can compromise respiratory function or the handling of respiratory secretions or that can increase the risk for aspiration. Morbid obesity is a risk factor for adults. † Percentage reported out of 113 children with a known medical history; conditions are not mutually exclusive. § Location of death was known for 114 children. ¶ Includes inpatient ward (10), intensive-care unit (62), operating room (one), and hospice (one). ** Illness onset date was not available for nine deaths. †† Percentage reported out of 64 children with specimen collected for bacterial culture from a normally sterile site. §§ Percentage reported out of 25 children with positive bacteria culture from a normally sterile site. ¶¶ More than one Streptococcus species could be isolated from each patient. *** Includes one Streptococcus parasanguinis and one not specified. ††† Includes one non-hemolytic and one alpha-hemolytic. §§§ Percentage reported out of 85 children with known complications; complications were not mutually exclusive. ¶¶¶ Percentage reported out of 94 children who died in a health-care facility. **** Percentage reported out of 74 children who had a known vaccination history and were eligible for vaccine. †††† Percentage reported out of children with known vaccination status. |
||
FIGURE 1. Number of influenza-associated pediatric deaths (N = 115), by week of death and type of influenza virus --- United States, September 1, 2010--August 31, 2011
Alternate Text: The figure above shows the number of influenza-associated pediatric deaths (N = 115), by week of death and type of influenza virus in the United States during September 1, 2010-August 31, 2011. The highest numbers of deaths occurred in late January and early February 2011.
FIGURE 2. Number of influenza-associated pediatric deaths (N = 106),* by number of days from influenza illness onset until death --- United States, September 1, 2010--August 31, 2011
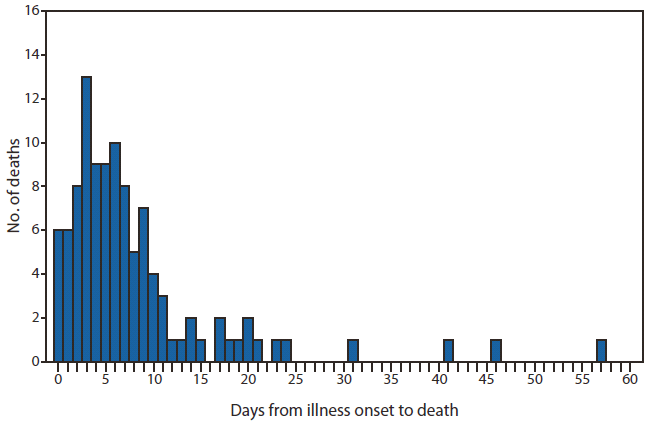
* Illness onset date not available for nine deaths.
Alternate Text: The figure above shows the number of influenza-associated pediatric deaths (N = 106), by number of days from influenza illness onset until death in the United States during September 1, 2010-August 31, 2011. Duration of illness ranged from 0 to 57 days.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
