Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Prevention and Control of Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2011
On August 18, 2011, this report was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr).
This document provides updated guidance for the use of influenza vaccines in the United States for the 2011--12 influenza season. In 2010, the Advisory Committee on Immunization Practices (ACIP) first recommended annual influenza vaccination for all persons aged ≥6 months in the United States (1,2). Vaccination of all persons aged ≥6 months continues to be recommended. Information is presented in this report regarding vaccine strains for the 2011--12 influenza season, the vaccination schedule for children aged 6 months through 8 years, and considerations regarding vaccination of persons with egg allergy. Availability of a new Food and Drug Administration (FDA)--approved intradermally administered influenza vaccine formulation for adults aged 18 through 64 years is reported. For issues related to influenza vaccination that are not addressed in this update, refer to the 2010 ACIP statement on prevention and control of influenza with vaccines and associated updates (1,2).
Methodology for the formulation of the ACIP annual influenza statement has been described previously (1). The ACIP Influenza Work Group meets every 2--4 weeks throughout the year. Work Group membership includes several voting members of the ACIP, as well as representatives from ACIP Liaison Organizations. Meetings are held by teleconference and include discussion of influenza-related issues, such as vaccine effectiveness and safety, coverage in groups recommended for vaccination, feasibility, cost-effectiveness, and anticipated vaccine supply. Presentations are requested from invited experts, and published and unpublished data are discussed. CDC's Influenza Division provides influenza surveillance and antiviral resistance data, and the Immunization Safety Office and Immunization Services Division provide information on vaccine safety and distribution and coverage, respectively.
Vaccine Strains for the 2011--12 Influenza Season
The 2011--12 U.S. seasonal influenza vaccine virus strains are identical to those contained in the 2010--11 vaccine. These include A/California/7/2009 (H1N1)-like, A/Perth/16/2009 (H3N2)-like, and B/Brisbane/60/2008-like antigens. The influenza A (H1N1) vaccine virus strain is derived from a 2009 pandemic influenza A (H1N1) virus (3).
Recommendations for Vaccination
Routine annual influenza vaccination is recommended for all persons aged ≥6 months (1). To permit time for production of protective antibody levels (4,5), vaccination should optimally occur before onset of influenza activity in the community, and providers should offer vaccination as soon as vaccine is available. Vaccination also should continue to be offered throughout the influenza season.
Although influenza vaccine strains for the 2011--12 season are unchanged from those of 2010--11, annual vaccination is recommended even for those who received the vaccine for the previous season. Although in one study of children vaccinated against A/Hong Kong/68 (H3N2) virus, vaccine efficacy remained high against this strain 3 years later, the estimated efficacy of vaccine decreased over the seasons studied (6). Moreover, several studies have demonstrated that postvaccination antibody titers decline over the course of a year (7--10). Thus, annual vaccination is recommended for optimal protection against influenza.
Vaccine Doses for Children Aged 6 Months Through 8 Years
Children aged 6 months through 8 years require 2 doses of influenza vaccine (administered a minimum of 4 weeks apart) during their first season of vaccination to optimize immune response. In a study of children aged 5 through 8 years who received trivalent inactivated vaccine (TIV) for the first time, the proportion of children with protective antibody responses was significantly higher after 2 doses than after 1 dose (11).
The importance of vaccine priming might depend more on the similarity of the antigenic composition between the priming and second dose than the temporal interval between doses. From the 2003--04 to 2004--05 influenza seasons, the A(H1N1) virus antigen remained unchanged; however, the A(H3N2) virus antigen changed to a drifted strain, and the B virus antigen changed more substantially to a different lineage. In a study conducted over those two seasons, influenza-vaccine naïve children aged 6 through 23 months who received 1 dose of TIV in the spring of their first year of vaccination followed by a second dose in the fall were less likely to have protective antibody responses to the A(H3N2) and B virus antigens when compared with children who received 2 doses of identical vaccine in the fall (12). Response to the unchanged A(H1N1) virus antigen was comparable between the groups. In another study conducted over the same two seasons, unprimed children aged 10 through 24 months who received 1 dose of TIV during the fall of each season had similar responses to the unchanged A(H1N1) virus antigen as well as to the drifted A(H3N2) virus antigen when compared with children aged 6 through 24 months who received 2 doses of the same TIV during the latter season; however, the first group had significantly lower response to the B virus antigen (13). During two seasons in which all influenza vaccine virus antigens were identical, unprimed children aged 6 through 23 months had similar responses when they received 1 dose in the spring followed by a second dose in the fall, as compared with 2 doses received 1 month apart in the fall (14). Studies of inactivated monovalent pandemic 2009 (H1N1) vaccine in children aged <9 years also have demonstrated improved response to this antigen when 2 doses are administered (15--17).
Vaccination providers should note that, in previous seasons, children aged 6 months through 8 years who received only 1 dose of influenza vaccine in their first year of vaccination required 2 doses the following season. However, because the 2011--12 vaccine strains are unchanged from the 2010--11 season, children in this age group who received at least 1 dose of the 2010--11 seasonal vaccine will require only 1 dose of the 2011--12 vaccine. Children in this age group who did not receive at least 1 dose of the 2010--11 seasonal influenza vaccine, or for whom it is not certain whether the 2010--11 seasonal vaccine was received, should receive 2 doses of the 2011--12 seasonal influenza vaccine (Figure 1). Recommendations regarding the number of doses for this age group might change for the 2012--13 season if vaccine antigens change.
Available Vaccine Products and Indications
Multiple influenza vaccines are expected to be available during the 2011--12 season (Table). All contain the same antigenic composition. Package inserts should be consulted for information regarding additional components of various vaccine formulations.
TIV preparations, with the exception of Fluzone Intradermal (Sanofi Pasteur), should be administered intramuscularly. For adults and older children, the deltoid is the preferred site. Infants and younger children should be vaccinated in the anterolateral thigh. Specific guidance regarding site and needle length can be found in the ACIP's General Recommendations on Immunization (18).
A new intradermally administered TIV preparation, Fluzone Intradermal, was licensed in May 2011. This vaccine is indicated for persons aged 18 through 64 years and contains less antigen than intramuscular TIV preparations (9 µg rather than 15 µg of each strain per dose) in a smaller volume (0.1mL rather than 0.5 mL). The vaccine is administered intradermally via a single-dose, prefilled microinjection syringe. The preferred site for administration is over the deltoid muscle (19). The most common adverse reactions include injection-site erythema, induration, swelling, pain, and pruritus. With the exception of pain, these reactions occurred more frequently than with intramuscular vaccine, but generally resolved within 3--7 days. This vaccine is an alternative to other TIV preparations for those in the indicated age range, with no preferential recommendation.
As during the 2010--11 season, a vaccine containing 60 µg of hemagglutinin per vaccine strain (rather than 15 µg per strain as in other intramuscular TIV preparations), Fluzone High-Dose (Sanofi Pasteur), is available as an alternative TIV for persons aged ≥65 years. No preference is indicated for this TIV versus other TIV preparations (1).
The intranasally administered live attenuated influenza vaccine (LAIV), FluMist (MedImmune) is indicated for healthy, nonpregnant persons aged 2 through 49 years. Within the indicated groups specified for each vaccine in the package inserts, no preference is indicated for LAIV versus TIV (1).
Vaccination of Persons Reporting Allergy to Eggs
Allergy to eggs must be distinguished from allergy to influenza vaccine. Severe allergic and anaphylactic reactions can occur in response to a number of influenza vaccine components, but such reactions are rare. A review of reports to the Vaccine Adverse Events Reporting System (VAERS) of adverse events in adults noted four reports of death caused by anaphylaxis following influenza vaccine during 1990--2005; the vaccine components potentially responsible for these reactions were not reported (20). A prior severe allergic reaction to influenza vaccine, regardless of the component suspected to be responsible for the reaction, is a contraindication to receipt of influenza vaccine.
All currently available influenza vaccines are prepared by inoculation of virus into chicken eggs. Hypersensitivity to eggs has been listed as a contraindication to receipt of influenza vaccine on most package inserts. However, several recent studies have documented safe receipt of TIV in persons with egg allergy (21--29), and recent revisions of some TIV package inserts note that only a severe allergic reaction (e.g., anaphylaxis) to egg protein is a contraindication. In general, these studies include relatively fewer persons reporting a history of anaphylactic reaction to egg, compared with less severe reactions. Several documents providing guidance on use of influenza vaccine in persons with egg allergy have been published recently (30--32).
The quantity of egg protein in vaccine is expressed as the concentration of ovalbumin per dose or unit volume. Among studies in which the ovalbumin content of the administered vaccine was reported, up to 1.4 µg/mL (0.7 µg/0.5 mL dose) was tolerated without serious reactions (22,23,25--29); however, a safe maximum threshold of ovalbumin, below which no anaphylactic reactions would be expected, is not known.
Although ovalbumin content is not required to be disclosed on package inserts for vaccines used in the United States, manufacturers either report maximum albumin content in the package inserts or will provide this information on request. Ovalbumin concentration can vary from season to season and from lot to lot for a given vaccine. Independent assessments of ovalbumin content of commercially available vaccines have noted lower concentrations than those listed on package inserts (33,34).
In several studies evaluating influenza vaccine in persons with egg allergy, additional safety measures have been taken, such as skin prick testing with vaccine (21--24,26,28,29) and administering the vaccine in 2 doses (e.g., 10% of the dose initially, followed by the remaining 90% if no reaction has occurred during a 30-minute observation period) (22,24--29). Skin prick testing with vaccine was poorly predictive of allergic reactions in these studies (22--24,26). In general, administration of both full doses and split doses have been well-tolerated without serious reactions, although systemic reactions (e.g., wheezing, eczema exacerbation, and hives on face/chest) were observed with the initial 10% dose among six (3.5%) of 171 participants in one study (24).
Recommendations Regarding Persons with Egg Allergy
Each of the following recommendations applies when considering influenza vaccination of persons who have or report a history of egg allergy.
1. Persons who have experienced only hives following exposure to egg should receive influenza vaccine with the following additional measures (Figure 2):
a) Because studies published to date involved use of TIV, TIV rather than LAIV should be used.
b) Vaccine should be administered by a health-care provider who is familiar with the potential manifestations of egg allergy.
c) Vaccine recipients should be observed for at least 30 minutes for signs of a reaction following administration of each vaccine dose.
Other measures, such as dividing and administering the vaccine by a two-step approach and skin testing with vaccine, are not necessary.
2. Persons who report having had reactions to egg involving angioedema, respiratory distress, lightheadedness, or recurrent emesis, or persons who required epinephrine or other emergency medical intervention, particularly those that occurred immediately or within minutes to hours after egg exposure are more likely to have a serious systemic or anaphylactic reaction upon reexposure to egg proteins. Before receipt of vaccine, such persons should be referred to a physician with expertise in the management of allergic conditions for further risk assessment (Figure 2).
3. All vaccines should be administered in settings in which personnel and equipment for rapid recognition and treatment of anaphylaxis are available. ACIP recommends that all vaccination providers be familiar with the office emergency plan (18).
4. Some persons who report allergy to egg might not be egg allergic. Those who are able to eat lightly cooked egg (e.g., scrambled eggs) without reaction are unlikely to be allergic. Conversely, egg-allergic persons might tolerate egg in baked products (e.g., bread or cake); tolerance to egg-containing foods does not exclude the possibility of egg allergy (35). Egg allergy can be confirmed by a consistent medical history of adverse reactions to eggs and egg-containing foods, plus skin and/or blood testing for immunoglobulin E antibodies to egg proteins.
5. A previous severe allergic reaction to influenza vaccine, regardless of the component suspected to be responsible for the reaction, is a contraindication to receipt of influenza vaccine.
Reported by
Lisa Grohskopf, MD, Timothy Uyeki, MD, Joseph Bresee, MD, Nancy Cox, PhD, Influenza Div; Carolyn Bridges, MD, Immunization Services Div, National Center for Immunization and Respiratory Diseases, CDC. Corresponding contributor: Lisa Grohskopf, lgrohskopf@cdc.gov, 404-639-2552.
Acknowledgments
Members of the Advisory Committee on Immunization Practices (ACIP), July 2010--June 2011.* ACIP Influenza Work Group. John Kelso, MD, Div of Allergy, Asthma, and Immunology, Scripps Clinic, San Diego California. Matthew Greenhawt, MD, Div of Allergy and Clinical Immunology, Univ of Michigan Health System. Neal Halsey, MD, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland. Clinical Immunization Safety Assessment Network Hypersensitivity Working Group. Matthew Fenton, PhD, Marshall Plaut, MD, National Institute of Allergy and Infectious Diseases, National Institutes of Health.
References
- CDC. Prevention and control of influenza with vaccines. Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2010. MMWR 2010;59(No. RR-8).
- CDC. Update: recommendations of the Advisory Committee on Immunization Practices (ACIP) regarding use of CSL seasonal influenza vaccine (Afluria) in the United States during 2010-11. MMWR 2010;59:989--92.
- Food and Drug Administration. February 25, 2011: Vaccines and Related Biological Products Advisory Committee meeting transcript. Rockville, Maryland: Food and Drug Administration; 2011.
- Gross PA, Russo C, Dran S, Cataruozolo P, Munk G, Lancey SC. Time to earliest peak serum antibody response to influenza vaccine in the elderly. Clin Diagn Lab Immunol 1997;4:491--2.
- Brokstad KA, Cox RJ, Olofsson J, Jonsson R, Haaheim LR. Parenteral influenza vaccination induces a rapid systemic and local immune response. J Infect Dis 1995;171:198--203.
- Foy HM, Cooney MK, McMahan R. A/Hong Kong influenza immunity three years after immunization. JAMA 1973;226:758--61.
- Ochiai H, Shibata M, Kamimura K, Niwayama S. Evaluation of the efficacy of split-product trivalent A(H1N1), A(H3N2), and B influenza vaccines: reactogenicity, immunogenicity, and persistence of antibodies following two doses of vaccines. Microbiol Immunol 1986;30:1141--9.
- Künzel W, Glathe H, Engelmann H, Van Hoecke C. Kinetics of humoral antibody response to trivalent inactivated split influenza vaccine in subjects previously vaccinated or vaccinated for the first time. Vaccine 1996;14:1108--10.
- Song JY, Cheong HJ, Hwang IS, et al. Long-term immunogenicity of influenza vaccine among the elderly: risk factors for poor immune response and persistence. Vaccine 2010;28:3929--35.
- Ambrose CS, Yi T, Walker RE, Connor EM. Duration of protection provided by live attenuated influenza vaccine in children. Pediatr Infect Dis J 2008;27:744--8.
- Neuzil KM, Jackson LA, Nelson J, et al. Immunogenicity and reactogenicity of 1 versus 2 doses of trivalent inactivated influenza vaccine in vaccine-naive 5--8-year-old children. J Infect Dis 2006;194:1032--9.
- Walter EB, Neuzil KM, Zhu Y, et al. Influenza vaccine immunogenicity in 6- to 23-month-old children: are identical antigens necessary for priming? Pediatrics 2006;118:e570--8.
- Englund JA, Walter EB, Gbadebo A, Monto AS, Zhu Y, Neuzil KM. Immunization with trivalent inactivated influenza vaccine in partially immunized toddlers. Pediatrics 2006;118:e579--85.
- Englund JA, Walter EB, Fairchok MP Monto AS, Neuzil KM. A comparison of 2 influenza vaccine schedules in 6- to 23-month-old children. Pediatrics. 2005;115:1039--47
- Plennevaux E, Sheldon E, Blatter M, Reeves-Hoché MK, Denis M. Immune response after a single vaccination against 2009 influenza A H1N1 in USA: a preliminary report of two randomised controlled phase 2 trials. Lancet 2009;375:41--8.
- Nolan T, McVernon J, Skeljo M, et al. Immunogenicity of a monovalent 2009 influenza A(H1N1) vaccine in infants and children: a randomized trial. JAMA 2010;303:37--46.
- Arguedas A, Soley C, Lindert K. Responses to 2009 H1N1 vaccine in children 3 to 17 years of age. N Engl J Med 2010;362:370--2.
- CDC. General recommendations on immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2011;60(No. RR-2).
- Sanofi Pasteur, Inc. Fluzone [package insert]. Swiftwater, Pennsylvania: Sanofi Pasteur, Inc.; 2011. Available at http://www.fda.gov/downloads/biologicsbloodvaccines/.../ucm195479.pdf. Accessed August 15, 2011.
- Vellozzi C, Burwen DR, Dobardzic A, Ball R, Walton K, Haber P. Safety of trivalent inactivated influenza vaccine in adults: background for pandemic influenza vaccine safety monitoring. Vaccine 2009;27:2114--20.
- Bierman CW, Shapiro GG, Pierson WE, Taylor JW, Foy HM, Fox JP. Safety of influenza vaccination in allergic children. J Infect Dis 1977;136(Suppl):S652--5.
- James JM, Zeiger RS, Lester MR, et al. Safe administration of influenza vaccine to patients with egg allergy. J Pediatr 1998;133:624--8.
- Esposito S, Gasparini C, Martelli A, et al. Safe administration of an inactivated virosomal adjuvanted influenza vaccine in asthmatic children with egg allergy. Vaccine 2008;26:4664--8.
- Chung EY, Huang L, Schneider L. Safety of influenza vaccine administration in egg-allergic patients. Pediatrics 2010;125:e1024--30.
- Gagnon R, Primeau MN, Des Roches A, et al. Safe vaccination of patients with egg allergy with an adjuvanted pandemic H1N1 vaccine. J Allergy Clin Immunol 2010;126:317--23.
- Greenhawt MJ, Chernin AS, Howe L, Li JT, Sanders G. The safety of the H1N1 influenza A vaccine in egg allergic individuals. Ann Allergy Asthma Immunol 2010;105:387--93.
- Owens G, MacGinnitie A. Higher-ovalbumin-content influenza vaccines are well tolerated in children with egg allergy. J Allergy Clin Immunol 2011;127:264--5.
- Webb L, Petersen M, Boden S, et al. Single-dose influenza vaccination of patients with egg allergy in a multicenter study. J Allergy Clin Immunol 2011;128:218--9.
- Howe LE, Conlon ASC, Greenhawt MJ, Sanders GM. Safe administration of seasonal influenza vaccine to children with egg allergy of all severities. Ann Allergy Asthma Immunol 2011;106:446--7.
- National Institutes of Health. Guidelines for the diagnosis and management of food allergies in the United States: summary of the NIAID-sponsored expert panel report. December 2010. Available at http://www.niaid.nih.gov/topics/foodallergy/clinical/pages/default.aspx. Accessed August 15, 2011.
- Greenhawt MJ, Li JT. Administering influenza vaccine to egg allergic recipients: a focused practice parameter update. Ann Allergy Asthma Immunol 201;106:11--6.
- Bernstein HH. Guidance offered on giving influenza vaccine to egg allergic patients. AAP News 2010;31:12.
- Li JT, Rank MA, Squillace DL, Kita H. Ovalbumin content of influenza vaccines. J Allergy Clin Immunol 2010;125:1412--3.
- Waibel KH, Gomez R. Ovalbumin content in 2009 to 2010 seasonal and H1N1 monovalent influenza vaccines. J Allergy Clin Immunol 2010;125:749--51.
- Erlewyn-Lajeunesse M, Brathwaite N, Lucas JS, Warner JO. Recommendations for the administration of influenza vaccine in children allergic to egg. BMJ 2009;339:912--5.
FIGURE 1. Influenza vaccine dosing algorithm for children aged 6 months through 8 years --- Advisory Committee on Immunization Practices (ACIP), 2011--12 influenza season
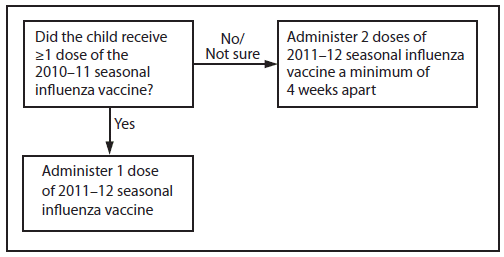
Alternate Text: The figure above shows influenza vaccine dosing algorithm for children aged 6 months through 8 years for the 2011-12 influenza season, according to the Advisory Committee on Immunization Practices (ACIP). Children aged 6 months through 8 years who did not receive at least 1 dose of the 2010-11 seasonal influenza vaccine, or for whom it is not certain whether the 2010-11 seasonal vaccine was received, should receive 2 doses of the 2011-12 seasonal influenza vaccine.
|
Vaccine
|
Trade name
|
Manufacturer
|
Presentation
|
Mercury content (µg Hg/0.5 mL dose)
|
Ovalbumin content (µg /0.5mL dose)
|
Age group
|
No. of doses
|
Route
|
|
TIV
|
Fluzone
|
Sanofi Pasteur
|
0.25 mL prefilled syringe
|
0.0
|
---†
|
6--35 mos
|
1 or 2§
|
IM¶
|
|
0.5 mL prefilled syringe
|
0.0
|
---†
|
≥36 mos
|
1 or 2§
|
IM¶
|
|
0.5 mL vial
|
0.0
|
---†
|
≥36 mos
|
1 or 2§
|
IM¶
|
|
5.0 mL multidose vial
|
25.0
|
---†
|
≥6 mos
|
1 or 2§
|
IM¶
|
|
TIV
|
Fluvirin
|
Novartis Vaccines
|
0.5 mL prefilled syringe
|
≤1
|
≤1
|
≥4 yrs
|
1 or 2§
|
IM¶
|
|
5.0 mL multidose vial
|
25.0
|
≤1
|
|
TIV
|
Fluarix
|
GlaxoSmithKline
|
0.5 mL prefilled syringe
|
0
|
≤0.05
|
≥3 yrs
|
1 or 2§
|
IM¶
|
|
TIV
|
FluLaval
|
ID Biomedical Corporation of Quebec (distributed by GlaxoSmithKline)
|
5.0 mL multidose vial
|
25.0
|
≤1
|
≥18 yrs
|
1
|
IM¶
|
|
TIV
|
Afluria
|
CSL Biotherapies (distributed by Merck)
|
0.5 mL prefilled syringe
|
0.0
|
≤1
|
≥9 yrs**
|
1
|
IM¶
|
|
5.0 mL multidose vial
|
24.5
|
≤1
|
|
TIV High-Dose††
|
Fluzone High-Dose
|
Sanofi Pasteur
|
0.5 mL prefilled syringe
|
0.0
|
---†
|
≥65 yrs
|
1
|
IM¶
|
|
TIV Intradermal
|
Fluzone Intradermal
|
Sanofi Pasteur
|
0.1 mL prefilled microinjection system
|
0.0
|
---†
|
18--64 yrs
|
1
|
ID
|
|
LAIV
|
FluMist§§
|
MedImmune
|
0.2 mL prefilled intranasal sprayer
|
0.0
|
---¶¶
|
2--49 yrs***
|
1 or 2§
|
IN
|
FIGURE 2. Recommendations regarding influenza vaccination for persons who report allergy to eggs --- Advisory Committee on Immunization Practices (ACIP), 2011--12 influenza season
Alternate Text: The figure above shows recommendations regarding influenza vaccination for persons who report allergy to eggs for the 2011-12 influenza season, according to the Advisory Committee on Immunization Practices (ACIP). Persons who have experienced only hives following exposure to egg should receive influenza vaccine with the following additional measures.
