Photo/New York City Department of Health and Mental Hygiene
Alternate Text: The figure above shows an amulet with leaded beads made in Cambodia, similar to one worn by a lead-poisoned child in New York City in 2009
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Lead poisoning in children is a preventable public health problem that can adversely affect the developing nervous system and result in learning and behavior problems. The most common source of exposure for lead-poisoned children aged <6 years in the United States is lead-based paint. However, nonpaint sources have been identified increasingly as the cause of lead poisoning, particularly in immigrant communities. This report describes a case of lead poisoning in a child aged 1 year that was investigated by the New York City Department of Health and Mental Hygiene's (NYC DOHMH) Lead Poisoning Prevention Program in 2009. The likely source of exposure was an amulet made in Cambodia with leaded beads that was worn by the child. Health-care providers and public health workers should consider traditional customs when seeking sources of lead exposure in Southeast Asian populations. Health-care providers should ask parents about their use of amulets, especially those in Southeast Asian families and those with children found to have elevated blood lead levels (BLLs). Educational efforts are needed to inform Southeast Asian immigrants that amulets can be a source of lead poisoning.
Restrictions in the use of lead in paint and gasoline have reduced the amount of environmental lead, resulting in a 98% decline in the number of children with BLLs ≥10 µg/dL from 1976 to 2004. The geometric mean BLL of children aged 1--5 years declined from 14.9 µg/dL in the late 1970s to 1.9 µg/dL in 2004 (1,2). Despite this improvement, some children remain at greater risk for lead poisoning: black children, children aged 1--5 years (especially children aged 1--2 years because of hand-to-mouth activity typical for this age group), children living in older deteriorated housing, and children living in poverty (2). In New York City, Asian children also have been noted to be at risk for lead poisoning (3).
The most common source of lead poisoning for young children is lead-based paint; however, nonpaint sources of lead are being identified increasingly in lead poisoning cases (4). Children with immigrant backgrounds might be at increased risk through exposure to lead-containing products from their family's country of origin. In New York City in 2007, among children with BLLs ≥15 µg/dL, 38% of foreign-born children did not have a lead paint hazard in the home compared with 21% of U.S.-born children (p<0.05) (3). Nonpaint lead risk factors include recent travel to a foreign country and use of imported products such as spices, food, candy, cosmetics, health remedies, ceramics or pottery, and jewelry.
Case Report
In March 2009, routine lead testing of a healthy, nonanemic boy aged 1 year who was born in the United States to Cambodian-born parents showed an elevated BLL of 10 µg/dL. Because the toddler shared a household with a cousin who had lead poisoning, he also had been tested at age 6 months, and was found to have a BLL of 1 µg/dL at that time. During the first home interview and inspection after the elevated BLL, the child's home and routine activities were evaluated by a risk assessor certified by the Environmental Protection Agency. The boy's father denied use of imported products, and no paint or nonpaint lead sources were identified. Out of 29 X-ray fluorescence (XRF) readings of painted areas obtained during the inspection, none were above U.S. Housing and Urban Development guidelines of 1 mg/cm2 of lead (5).
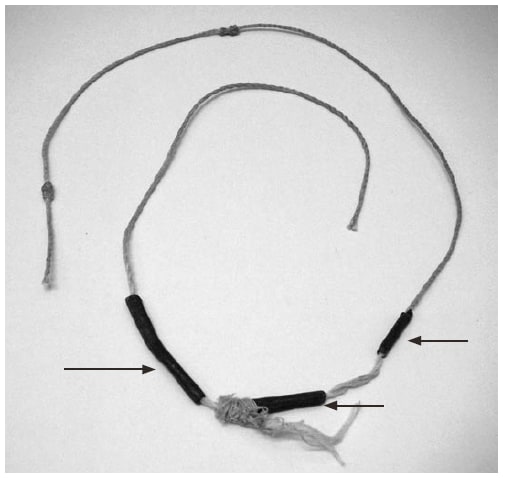
Three months later, the child's BLL increased to 20 µg/dL. In a telephone interview before a second home inspection, the boy's father again denied that the child wore jewelry or charms, but when questioned more closely, he said that the toddler wore an amulet or "something to protect him." The amulet, acquired by the boy's mother in a rural Cambodian market, was a knotted string onto which gray metallic beads had been molded (Figure). The father reported that the boy had worn the amulet around his neck since age 3 months and had been observed mouthing it.
The second home inspection revealed one positive XRF reading of 2.2 mg/cm2 on an interior window sill and several potential nonpaint lead sources: two imported spices, imported rice, and the amulet. All four nonpaint samples were sent to a laboratory for acid-digestion testing. The lead contents of the food items were below the limits of detection used, which were 0.94 mg/kg and 0.95 mg/kg for the spices and 0.49 mg/kg for the rice. The amulet's metal beads had a total lead content of 450,000 mg/kg (45%).
Within 8 days of the amulet being removed from the home, the child's BLL had decreased from 20 µg/dL to 14 µg/dL. Six weeks after the amulet was removed, and 2 days after the lead paint violation was reported as abated, the child's BLL was 10 µg/dL. Five months after the amulet was removed, the boy's BLL was down to 5 µg/dL. Although other factors might have contributed to the child's overall lead burden, the most likely source identified was the amulet, based on its high lead content, statements that the child had been observed mouthing it, and the rapid decrease in the child's BLL after its removal.
The toddler's cousin, aged 6 years, who was living in the same home, had lead poisoning diagnosed in September 2008. His BLL had been 17 µg/dL. Fifty-eight violations for lead had been repaired in the home, and during the next 8 months the boy had BLLs of 11--15 µg/dL. He also had worn a Cambodian amulet, and 3 months after he stopped wearing his amulet, his BLL was 7 µg/dL. The toddler's sister, aged 10 years, was tested and had a BLL of 4 µg/dL. Although she also wore an amulet, she presumably was old enough not to mouth it.
M Mann, MD, MN Rublowska, JE Ehrlich, MD, Lead Poisoning Prevention Program, New York City Dept of Health and Mental Hygiene, New York. MS Sucosky, MPH, CM Kennedy, DrPH, Healthy Homes and Lead Poisoning Prevention Br, Div of Environmental Hazards and Health Effects, National Center for Environmental Health, CDC.
Wearing amulets is common among Cambodians and other ethnic groups in Southeast Asia, including Vietnamese, Hmong, and Lao populations. Typically, infants and toddlers wear these "protection strings" around their necks, wrists, or waists (6). The amulets usually are made of black or white string with several knots, metal beads, or both. The knots and beads are believed by some to be infused with protective powers. In this case, the mother of the toddler reported that on her most recent trip to Cambodia, she had three amulets custom-made ("cooked in a pot") for the children in her family. Anecdotal information suggests that lead bullets sometimes are melted to make the beads for such amulets.
This case identified a lead risk factor not previously recognized for the Southeast Asian community. In addition, this case highlights the importance of blood lead testing in children of immigrants because of the increased risk for exposure to lead-containing foreign products. CDC recommends blood lead testing for internationally adopted and refugee children.* NYC DOHMH recommends testing all children with recent travel to foreign countries.
This case also adds to the medical literature of nonpaint lead sources as causes of lead poisoning. Some incidents of lead poisoning in children from atypical sources have been documented previously (4,7), and two cases of jewelry-associated lead poisonings in children have been reported recently. In 2004, a boy aged 4 years from Oregon had a BLL of 123 µg/dL after ingesting a necklace with a 38.8% lead content that had come from a vending machine (8). In 2006, another boy aged 4 years from Minnesota died from acute lead poisoning after ingesting a heart-shaped metallic charm containing 99.1% lead (9). These two cases led to the recall of 150 million pieces of imported metallic toy jewelry sold in vending machines and a voluntary recall of 300,000 heart-shaped charm bracelets, respectively. These cases also call attention to ingestion of jewelry as a mechanism for lead poisoning.
Educational efforts are needed to inform Southeast Asian immigrants that amulets can be sources of lead poisoning for children. Health-care providers and public health workers should ask about this custom when seeking a source of exposure in Southeast Asians with elevated BLLs. Targeted educational efforts in Southeast Asian communities also should be considered. This case also underscores the importance of being aware of different cultural practices, such as wearing amulets, and highlights the need to assess and reassess the same risk factors and rephrasing questions using different words when communicating with immigrant families.
* Guidelines available at http://www.cdc.gov/nceh/lead/tips/populations.htm.
What is already known on this topic?
Although the most common source of lead poisoning for young children is lead-based paint, nonpaint sources of lead are being identified increasingly in lead poisoning cases, particularly in immigrant communities.
What is added by this report?
This report describes a case of pediatric lead poisoning that likely resulted from wearing an amulet made in Cambodia with leaded beads, a newly identified lead risk factor for the Southeast Asian community.
What are the implications for public health practice?
Educational efforts are needed to inform Southeast Asian immigrants that amulets can be a potential source of lead poisoning. Health-care providers should ask parents about use of amulets, especially Southeast Asian families and those with children found to have elevated blood lead levels.
FIGURE. Amulet with leaded beads (indicated by arrows) made in Cambodia similar to the one worn by a lead-poisoned child --- New York City, 2009.
Photo/New York City Department of Health and Mental Hygiene
Alternate Text: The figure above shows an amulet with leaded beads made in Cambodia, similar to one worn by a lead-poisoned child in New York City in 2009
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
