Learn more about the Prevention Research Centers (PRCs).
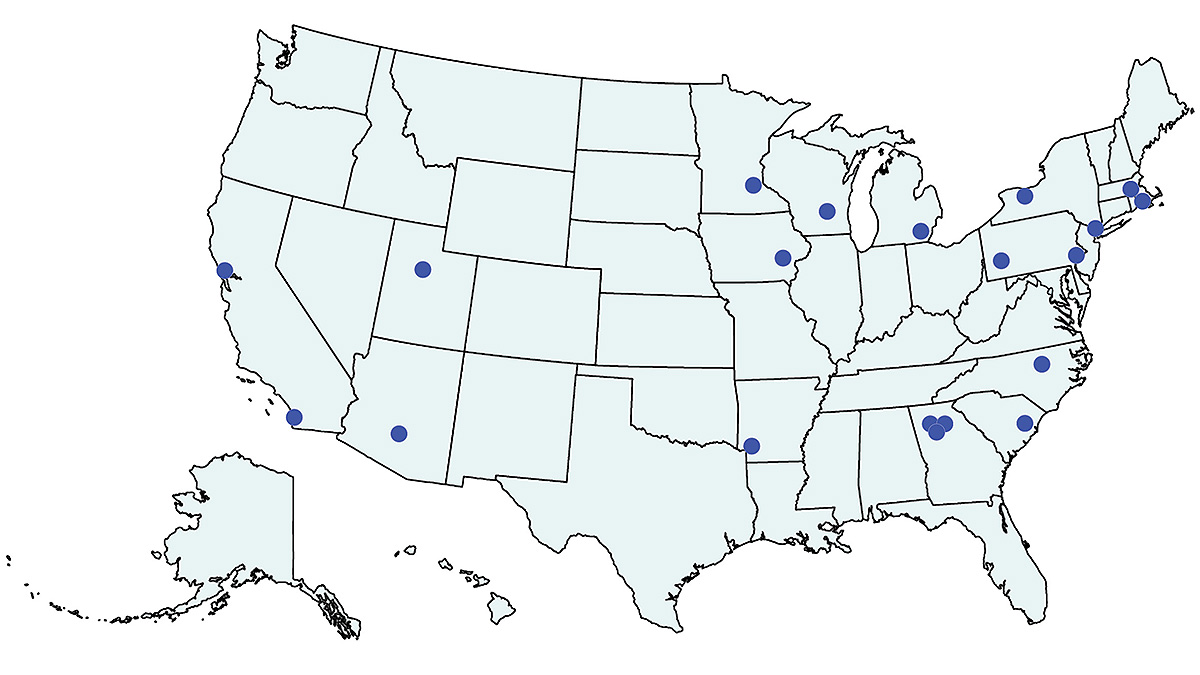
CDC currently funds 20 PRCs during the 2024–2029 funding cycle.
- Prevention Research Centers funded during the 2019-2024 cycle.
- Explore PRC core research projects and dissemination and implementation science.
- Read about the currently funded Thematic Research Networks.
- Impact of the PRC Program
- Communication resources for the CDC Prevention Research Centers
- The P2P Resource center is a one-stop, easy-to-navigate website that features tools and resources pr...