
Snowplow Operator Caught Between Two Trucks in Nebraska
July 23, 2001
Nebraska FACE Investigation 01NE008
SUMMARY:
A 57-year-old male equipment operator was killed when he was pinned between two trucks. The victim was power washing the windshield of a snowplow equipped truck, when another truck backed out of a nearby shed and pinned him against the vehicle’s front fender. He was immediately provided first aid until rescue personnel arrived, then transported to a local hospital where he was pronounced dead.
The Nebraska Workforce Development Department of Labor Investigator concluded that to prevent future similar occurrences:
- Employers should develop, implement and review their policies and training programs on the particular type of equipment the employees will be utilizing to include safe backing practices.
- Employers should ensure that “close proximity devices” and other such devices are evaluated to see if they would be beneficial for this type of operation.
- Employers should develop, implement and enforce a policy that requires each bay entrance to be clear of all obstacles to allow for a clear path of travel and adequate clearance for the trucks and plows.
- Employees should ensure that their path of travel is clear prior to putting the vehicle in motion.
- Employees should read, understand and obey all written safety requirements for the type of equipment they are operating.
PROGRAM OBJECTIVE:
The goal of the Fatality Assessment and Control Evaluation (FACE) workplace investigation is to prevent work-related deaths or injuries in the future by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact.
This report is generated and distributed solely for the purpose of providing current, relevant education to employers, their employees and the community on methods to prevent occupational fatalities and injuries.
INTRODUCTION:
On February 14, 2001 at approximately 5:35 a.m., a 57-year-old equipment operator was killed when he was pinned between two snow plow equipped dump trucks. The Nebraska Department of Labor was made aware of the fatality the same day by OSHA, the local news media and the victim’s employer. The Investigator talked with company officials on February 14, 2001 and met them on March 1, 2001. A site visit was conducted on April 13, 2001. Local law enforcement reports concerning this incident were also reviewed.
The employer is a large municipality. They employ 350-400 personnel in this division. They have operated from this site for approximately 10 years. They do have a written safety program and full time safety personnel. They have no previous history of fatalities in this division.
INVESTIGATION:
The victim was a 57-year-old male equipment operator. He had been employed by the municipality for 35 years. He had performed this task many times over the years. Safety training had been conducted routinely every year prior to snow removal operations, and whenever new equipment was being used. All three persons involved had received relative safety training one week prior to the accident. It covered backing procedures and the use of spotters when available, or checking the area themselves.
On the mishap day the victim and co-workers started their shift at 03:30 a.m. All three were assigned the task of removing snow and spreading sand/salt on roadways. After performing “pre-trip” inspections of their trucks, they filled them with salt/sand and left on their assigned routes. By 05:20 a.m. they had emptied their trucks and had returned to the maintenance yard to refill and perform any minor maintenance necessary.
There were a total of three personnel directly involved in this accident:
a. Operator #1, a 46-year-old male, with truck #1, a 1993 International 4900 Series single axle dump truck, orange in color with a snowplow attached to the front. He has worked for this employer since May of 2000.
b. Operator #2, a 26-year-old male, with truck #2, a 1996 International 4700 series single axle dump truck, orange in color with a snowplow attached to the front. He has worked for this employer full time since March of 1999.
c. The victim with truck #3, a 2000 International 4000 Series dump truck, orange in color with a snowplow attached to the front. He had worked for the employer for over 35 years.
The accident site is a vehicle maintenance facility used to house maintenance vehicles when minor repairs are being completed. The building runs east to west. The inside bay area was well lit with sodium type lights and the floor was wet with a heavy dusting of salt and sand. All interior lights were working. The building has 16′ wide garage doors to the bays that face south and open up into a maintenance yard parking lot area. There is exterior street lighting located at various locations throughout the yard. There are also flood lights located overhead on the exterior between the bays. One floodlight between bays #4 and #5 was inoperative. All other exterior lights were working. The yard area was covered with a layer of ice/snow/sleet approximately ¼” to ½” in depth. The temperature was 10 degrees with a northwest wind blowing at 13 mph, gusting to 30 mph. It had been raining since 04:06 a.m. that morning. There had been considerable snow, sleet, drizzle and fog in the area.
(See figure #1) The victim had parked his truck facing the bays (north), lined up slightly to the left of center to bay #6, the wash bay entrance. Before assuming his route duties, the victim was using a steam power washer to remove ice, dirt and debris from his truck’s windshield and lights. He was standing beside his vehicle’s front driver’s side tire facing the truck. Operator #1 could not get the belt on his spreader to work properly, and was going to pull into bay #5, located next to the wash bay on the west (left) side. He was going to perform either minor maintenance or acquire a replacement vehicle if necessary. He exited his vehicle to go inside to raise the door, and told the victim his intentions. The victim acknowledged the warning and continued cleaning. Operator #1 opened the bay door, pulled in apx. three quarters of the vehicle length, but realized he was at too great an angle to the stall to proceed safely. The stall width was restricted approximately 3-4 feet due to several buckets and a barrel stored along the east (right) side wall. To continue would have caused the driver’s side rear dual wheels to hit the door jam. He stopped his forward motion, placed the truck in reverse and immediately started backing out at an angle to square up to the stall. As he backed out, the plow blade did catch one of the buckets and drag it a short distance. He did not honk his horn to indicate he was backing up.
(See photo #1) At this same time, Operator #2 saw the victim using the steam power washer. He pulled up directly behind the space just vacated by Operator #1. His truck was pointed in a northeast direction adjacent to the front of bay door #5 at an angle facing the driver’s side of the victim’s truck. He rolled down his driver’s side window and asked the victim if he would wash his ice covered windshield off also. The victim said “yeah” and walked over to the driver’s side of truck #2 beside the front tire and started spraying the windshield, which left him facing away from vehicle #1 in the bay. Operator #2 rolled up his driver’s side window, closed the wing window, then leaned over to ensure his passenger side window was rolled up completely and sat back upright. His headlights and plow lights were still on.
(See photo #2) At this same time, Operator #1 was backing up. He was looking at his driver’s side mirror to ensure he cleared the door frame. When he looked out of his passenger side mirror, he was unable to see the victim or vehicle #2, but able to see the victim’s truck cab lights. The victim just finished making a pass over Operator #2’s windshield as Operator #2 sat back upright, seeing vehicle #1’s backup lights through the receding water on his windshield. Operator #2 grabbed his radio mike and attempted to shout a warning to Operator #1 but wasn’t able to do so before the accident occurred. He did ask for “anyone” to call for an ambulance immediately.
As Operator #1 was about to stop his reverse motion, he stated he felt “a slight thump”, but he did not know its exact source. The victim was either struck and pushed forward into, or pinned directly between the right rear dump box of vehicle #1 and the front driver’s side fender of vehicle #2. Operator #1 placed his vehicle into forward, pulled into the stall and exited his vehicle, not realizing he had hit the victim.
As vehicle #1 pulled forward, Operator #2 saw the victim fall to the ground. He exited his truck to check on the victim, then returned to the cab to grab his coat to cover the victim. Operator #2 estimated there was only 6 or 7 seconds between the time he saw the vehicle #1’s lights until he exited his vehicle. Operator #1 was walking towards the scene, and Operator #2 instructed him to grab his coat also to lay over the victim. Other employees were arriving at the scene also, allowing Operator #2 to run inside the office area. He grabbed several more coats while informing the office personnel to call 911. Other personnel started CPR until emergency personnel arrived within a few minutes. The victim was transported to a local hospital where he was pronounced dead.
Post accident investigation was conducted by the employer’s safety personnel and local law enforcement. Vehicle #1’s backup alarm was tested and in proper order. This alarm activates when the transmission is placed into reverse, and continues to sound until the transmission is shifted to another gear. The truck does not have to be in motion for it to sound. The mirrors were also properly adjusted, although dirty. All tail, backup and break lights were functioning properly. The only new damage to either vehicle #1 or vehicle #2 consisted of a new crack and smudge mark in the fiberglass fender of vehicle #2, directly over the left front wheel area (See photo #3). The crack still had fresh, minute fiberglass particles sticking from it. It is believed that this is the area where the victim was pinned between the trucks.
Several factors may have contributed to this accident. At the angle Operator #1 was backing, he would not have been able to see vehicle #2 nor the victim in the driver side mirror. The passenger side mirror was in a brightly lit (sodium lights) bay, while outside was partially dark. The maintenance yard area was lit by lighting located throughout the yard area. There are also lights located overhead between the bays. The light between bays 4 and 5 was burnt out at the time of the accident, but should not have had a major impact on the overall lighting. There may have also been quite a bit of steam generated by the power washer’s spray contacting the extremely frigid air. During the mishap time period, the temperature was 10 degrees with snow and sleet falling. The driving surface was covered with ¼ to ½ inch of ice, snow and sleet. It was also snowing/sleeting during most of the early morning. Although early in the morning, there were other vehicles entering and exiting during this time period. The combined noise of the three diesel trucks, other vehicles, and the power washer may not have allowed the victim to hear the backup alarm. Local law enforcement investigators stated that with just the power washer running it was extremely difficult to hear. If he did hear the alarm, he may not have had time to recognize which vehicle it was coming from nor time to react. Neither Operator #1 or #2 remember hearing the alarm. There is also the possibility that fatigue and stress may have played some part in this accident. All three personnel had been working long hours for many days during this year’s severe winter. There was a sense of urgency amongst the snowplow operators to get back to their routes before the morning rush hour started. There was no blood/alcohol presence noted in Operator #1’s or the victim’s post accident testing.
CAUSE OF DEATH:
Multiple internal injuries/Pinned between two snow plows.
RECOMMENDATIONS/DISCUSSION:
Recommendation #1: Employers should develop, implement and review their policies and training programs on the particular type of equipment the employees will be utilizing to include safe backing practices.
Discussion: This employer has full time safety personnel that have developed high quality safety training programs. These programs are administered to all employees prior to this “seasonal” task, and also before the use of any new or unfamiliar equipment. These programs are constantly updated. A new “BACKING SAFELY TO AVOID ACCIDENT” flyer was developed and distributed shortly after the accident as a reminder to follow established safety guidelines. All snow plow operators have received their commercial drivers license (CDL) as required by the U.S. Department of Transportation. [CFR 1926.20(b) & 1926.21(b)(2)]
Recommendation #2: Employers should ensure that “close proximity devices” and other such devices are evaluated to see if they would be beneficial for this type of operation.
Discussion: A proximity warning device functions as a supplemental safety system on a vehicle. It tells the operator how close the vehicle is to another vehicle, object or person behind the vehicle. It uses ultrasonic technology to “see” moving and stationary objects. The detector is normally mounted on the rear bumper of the vehicle and emits ultrasonic waves in a three-dimensional field. The device detects anything in or crossing its detection area (day or night), even if it is beyond or below the operator’s field of vision. An on-board display module warns the driver if an obstacle is present and how close it is by using audio and visual alerts. The employer has obtained a “close proximity device” and is currently evaluating its effectiveness for snow plow operations.
Recommendation #3: Employers should develop, implement and enforce a policy that requires each bay entrance to be clear of all obstacles to allow for a clear path of travel and adequate clearance for the trucks and plows.
Discussion: Bay #5’s access width was restricted by several buckets and a barrel that were stored along the right side wall. This restricted the forward access by Operator #1, forcing him to back out, then pull into the bay again. The employer may want to consider moving these items away from the wall.
Recommendation #4: Employees should ensure that their path of travel is clear prior to putting the vehicle in motion.
Discussion: Established written procedures state that a vehicle operator, prior to backing, should ask for a spotter to assist. When this is not possible, the operator should exit the vehicle his/herself to check the rear and side areas. In either case, the horn should also be utilized along with existing warning devices to increase the awareness of those close by. [CFR 1926.601(b)(4)(i)-(ii)]
Recommendation #5: Employees should read, understand and obey all written safety requirements for the type of equipment they are operating.
Discussion: Vehicle operators at this facility are all trained prior to actual street operation of the snow plows. All training is well documented and current. [CFR 1926.20(b)(4)]
REFERENCES:
OSHA Part 1926 Code of Federal Regulations for Construction Standards
ATTACHMENTS:
Figure #1: Diagram of accident site.
Photo #1: Picture of vehicle positioning taken 3 hours after accident.
Photo #2: Picture taken from rear of vehicle #1 showing proximity of vehicle #2.
Photo #3: Shows point of impact on vehicle #2’s fender with new crack in fiberglass.

Figure #1 — Accident Site Diagram.
This diagram represents the approximate positioning of all three vehicles at the time of impact.
The X marks the area where the victim was standing.

Photo #1. This picture shows vehicle #2 (foreground) and vehicle #3 (background) as they sat during the accident.
Vehicle #1 is inside the bay (see open bay door).
NOTE: Arrows on Photos #1 and #2 point to where victim was standing.

Photo #2. This picture, taken from the box of vehicle #1, shows the close proximity to vehicle #2.
This picture was taken when vehicle #1 was completely inside the maintenance bay.
NOTE: Arrows on Photos #1 and #2 point to where victim was standing.
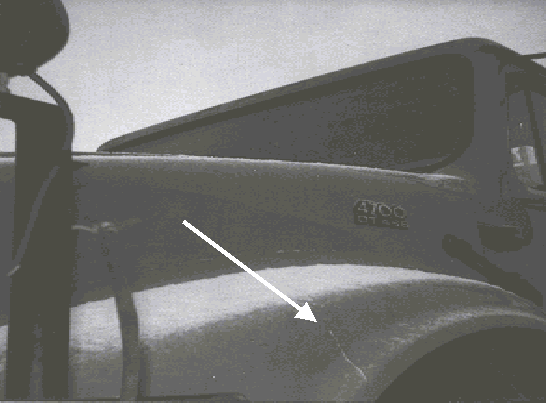
Photo #3. This is vehicle #2’s front driver’s side fender where the point of impact occurred.
Note the crack in the fiberglass fender.
Arrow points to crack in fiberglass fender.
To contact Nebraska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.