
Equipment Operator Drowns in Canal
September 25, 2001
Nebraska FACE Investigation 00NE016
SUMMARY:
A 56-year-old equipment operator drowned when the water tanker he was operating went into a canal. He was in the process of filling the tanker with water. The tanker was parked on a road parallel to the canal. The victim apparently was in the cab of the tanker when it rolled into the canal. He was found in the canal approximately 50 feet east of the tanker and emergency personnel were called. He was taken to a hospital where he was pronounced dead two days later on July 19, 2000.
The Nebraska Department of Labor Investigator concluded that to prevent future similar occurrences:
- employers and employees should ensure the transmission on the water tanker is placed in neutral and the emergency brake set during water filling.
- employers and employees should ensure the wheels on the tanker are chocked.
- employers and employees should ensure the wheels on the tanker are turned away from the canal, or other water source.
- employers should perform a Job Hazard Analysis (JHA) on the water filling operation.
PROGRAM OBJECTIVE:
The goal of the Fatality Assessment and Control Evaluation (FACE) workplace investigation is to prevent work-related deaths or injuries in the future by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact.
This report is generated and distributed solely for the purpose of providing current, relevant education to employers, their employees and the community on methods to prevent occupational fatalities and injuries.
INTRODUCTION:
On July 17, 2000, at approximately 10:00 a.m., a 56-year-old equipment operator drowned when the water tanker he was operating went into a canal. The Nebraska Department of Labor was notified of the fatality on July 19, 2000, by OSHA. The Nebraska FACE Investigator and an OSHA Compliance Officer conducted a site visit on July 20, 2000. Interviews were conducted with management and workers at the work site.
The employer is a dirt contractor and has been in business for approximately 30 years. The company had been at the incident location for approximately two months. The company employs a total of approximately 40 people and 10 were employed at the incident location. The company has had no previous fatalities in its history. A part-time safety consultant is employed by the company. The company has a written safety program.
The victim had been employed by the company for approximately nine years. He had received general safety training from the company but their was no specific documented training on the water tanker. Another water tanker operator stated the victim was provided on-the-job training on the equipment.
INVESTIGATION:
On the day of the incident the victim started his shift at 7:00 a.m. The incident happened at approximately 10:00 a.m. The victim was an equipment operator. The project the company was working on was building a new road. The water tanker the victim was operating was used to spray the road surface with water to keep the dust down. The tanker was refilled numerous times during the workday. The victim was experienced with the refilling procedure and he had refilled the tanker 67 times since he began working on the project on July 6, 2000.
Standard procedure for filling the tanker, at the incident location, is to pull the tanker up parallel to the canal and connect one end of the fill hose to the tanker. The other end of the hose is in the canal. The hose is tied to a “Stop Ahead” sign to keep it from moving around (see figure 1).
The operator then has to return to the cab of the tanker to flip some toggle switches to pump the water into the tanker. The engine is revved, with the transmission in neutral, to get the water pumping. After the tanker is filled the hose is disconnected from the tanker.
On the day of the incident, an employee of another company noticed that the tanker was in the canal (see figure 2). This individual notified a representative of the incident company who responded to the scene. The victim was discovered about 50 feet east of the cab of the tanker, which was underwater. The canal was flowing from west to east. Either the victim was swept out of the cab by the flowing water or he got out of the cab and was possibly attempting to return to shore. Rescue personnel were called and the victim was transported to a hospital where he died two days later.
When the truck was pulled out of the canal, it was in 8th gear and the emergency brake was set. Standard procedure was to have the transmission in neutral with the brakes set. Although the brake was set we cannot be sure it was set prior to the tanker rolling into the canal. It could have set itself due to lack of air pressure.
Two plausible scenarios are: 1. The victim had prepared the tanker for refilling and returned to the cab. While in the cab he revved up the engine to get the water pumping. With the transmission in 8th gear, the tanker could have lunged forward into the canal. 2. The victim could have suffered a heart attack or seizure and stepped on the gas pedal, running the tanker into the canal. An autopsy was not performed, however the victim was a diabetic and was on several types of medications.
CAUSE OF DEATH:
The cause of death, as stated on the death certificate, was anoxic brain damage as a consequence of drowning.
RECOMMENDATIONS/DISCUSSION:
Recommendation #1: Employers and employees should ensure the transmission on the water tanker is placed in neutral and the emergency brake set during water filling.
Discussion: Had the transmission been in neutral, which is standard operating procedure, the tanker would not have gone into the canal. Setting the emergency brake, which may or may not have been set in this case, just adds another measure of safety to the operation.
Recommendation #2: Employers and employees should ensure the wheels on the tanker are chocked.
Discussion: It is a good safety practice to chock the wheels of equipment while working around it, particularly while it is running, as was the case in this incident. Had the wheels been chocked, this might have prevented the tanker from rolling into the canal, even with the engine revved and the tanker in 8th gear.
Recommendation #3: Employers and employees should ensure the wheels on the tanker are turned away from the canal, or other water source.
Discussion: Another safe practice is to turn the wheels of a vehicle away from a hazard, in this case the canal. Had the front wheels of the tanker been turned to the right, away from the canal, the tanker would have merely traveled into an empty field when the engine was revved.
Recommendation #4: Employers should perform a Job Hazard Analysis (JHA) on the water filling operation.
Discussion: A Job Hazard Analysis (JHA) is a process of studying and recording each step of a job to identify existing or potential job hazards and determining the best way to do the job to reduce or eliminate these hazards. A JHA performed on the tanker refilling task should have identified recommendations one through three above. Had these recommendations been implemented, as part of the JHA, this incident might have been prevented.
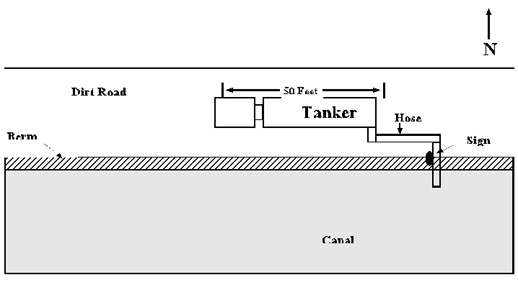
Figure 1. Location of Tanker Prior to Incident
Figure 2. Location of Tanker After Incident
To contact Nebraska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.