
Truck Driver Killed When Front-End Loader Secured by Chains on a Lowboy Trailer Broke Free and Rolled Onto Cab
Investigation: # 02MI040
SUMMARY

|
| Figure 1. Loader on truck cab |
On April 10, 2002, a 56-year old truck driver with 22 years of experience died when a front-end loader weighing between 60,000 and 65,000 pounds that was being transported on a 50-ton lowboy trailer broke free from its securing chains and rolled onto the cab crushing him. The loader transmission was in neutral and the parking brake was set. The victim used at least four 3/8-inch chains rated at 6,600 pounds (the exact number is unknown) to secure the loader. Five binders were found at the scene. One chain appeared to be improperly attached to the loader’s maintenance ladder, one chain appeared to be attached to an attachment point on the loader. The remaining chain attachments to the loader are unknown. If four chains were used, the load exceeded the aggregate working load limit of the chains. Also unknown is where each of the chain hooks and/or binder hooks were attached to the trailer. Based on the police report of the incident, at least one chain hook/binder was improperly attached to the trailer bed. One chain appeared to have an oversized hook. During transport, the driver stopped suddenly between two bridges. Skid marks from the truck were present on the roadway. It appears that a sudden stop caused sufficient force on the chains to break them. The loader rolled forward over the 5th wheel and onto the top of the truck cab. The cab was crushed, and the driver was declared dead at the scene.
RECOMMENDATIONS
- Companies should require and train employees to use manufacturer identified cargo attachment points and “D” rings on the trailer using the appropriate number of tiedown assemblies.
- Companies should ensure that consistency is maintained with the working load limits of all components of a tiedown assembly.
- Companies should ensure employees inspect all components of a tiedown assembly to ensure that they are in good working order and are an appropriate and consistent size.
- Additionally, MIFACE recommends that all employers develop standard operating procedures and provide employee training to educate workers about the January 2004 FMCSA new cargo securement rules.
INTRODUCTION
On April 10, 2002, a 56-year old male truck driver died when a 60,000-65,000 pound front-end loader on a 50-ton lowboy trailer broke free from its securing chains and rolled onto the cab. MIFACE investigators were notified of this work-related fatality by a newspaper clipping. The company agreed to participate in the MIFACE program and on May 21, 2002 a MIFACE researcher interviewed the owner of the company and several company employees at the company headquarters about work practices. After the interview, the owner and MIFACE researcher viewed the chains thought to be used to secure the front-end loader and was shown how a piece of equipment is secured on a lowboy trailer. The pictures in Figures 1-12, Figure 15 and Figure 17 were taken by the responding enforcement agency at the time of the incident. Pictures in Figures 13,14, and Figure 16 are MIFACE pictures taken at the company’s headquarters. The death certificate, autopsy results, and police report were obtained during the course of the investigation. To preserve anonymity, MIFACE removed the company’s name from the truck in Figure 7.
MIOSHA was notified by the police and sent a compliance officer to the incident location. MIOSHA did not conduct an investigation because the incident did not occur in a construction zone.
Michigan has adopted the U.S. Department of Transportation Federal Motor Carrier Safety Administration (FMCSA) Rules and Regulations. The Federal Motor Carrier Safety Administration was established as a separate administration within the U.S. Department of Transportation on January 1, 2000. FMCSA’s mission is to reduce crashes, injuries, and fatalities involving large trucks and buses. FMCSA develops, maintains, and enforces federal regulations that promote carrier safety, industry productivity, and new technologies. FMCSA Part 393, Parts and Accessories Necessary for Safe Operation, Subpart I, Protection Against Shifting or Falling Cargo encompasses several regulations that identify work practices to be followed when securing a load on a trailer. §393.100 are the general rules for protection against shifting or falling cargo, §393.102 describes securement systems, and §393.104 describes blocking and bracing. In December 2002, regulations for securement by commodity type went into effect; §393.130 regulates securement of heavy vehicles, equipment and machinery, such as front-end loaders. This fatality occurred prior to the promulgation of the new cargo securement rules.
INVESTIGATION
The company that employed the victim is a family-owned excavating company that does site preparation for roads, parking lots, etc. The company has been in business for 30 years. The company employs, on an average, approximately 80 people. During road construction season, it may employ as many as 100 people. Approximately 15 other employees have the same job classification, truck driver, as the victim. The victim also trained new drivers on truck safety issues.
The victim was a full-time employee with over 22 years experience in the trucking business. The company has a written health and safety program, but did not have written safety rules and procedures in place for the victim’s specific task (load securement). Company employees indicated that chains were routinely checked for damage by visual inspection and also by laying the chain on the ground and measuring it to determine if the chain had “stretched”.
The company uses an outside paid consultant as well as governmental agencies to assist it with its health and safety program. A person is assigned within the company that has primary responsibility for safety. This person reports directly to the company owner. This individual has attended health and safety seminars and has on-the-job experience working on excavation sites and spends at least 75% of the workday devoted to safety issues.
On-site safety responsibilities are delegated to site supervisors. The supervisors receive at least 8 hours of safety training and attend company-sponsored safety meetings at least one time per month. On site, the supervisors hold weekly tailgate talks. On an annual basis, company employees receive nearly 40 hours of safety training. The company has an informal group designated as the health and safety committee, which meets on a monthly basis. The company has a written disciplinary procedure in place for violations of the health and safety policy.
The company purchased the lowboy trailer new in 1994. The trailer had a 50-ton carrying capacity. The trailer bed was 2 feet high, 10 feet wide and over 54 feet long. The front-end loader was a Michigan L190 with an estimated weight of 60,000-65,000 pounds. The loader bucket was empty and lowered. The victim secured the loader with Grade 7, 3/8-inch transport chains rated by the manufacturer at 6,600 pounds with 5/16 grab hooks rated for 3/8-inch chains. Ratchet binders were used to eliminate chain slack. One hook (See Figure 17) appeared to be larger than the 5/16-grab hook. The tractor cab had an oversize load sign on the front bumper, and two 12-inch by 12-inch red flags attached to the bumper. The trailer had two 12-inch by 12-inch red flags at the rear of the trailer.
The loader was transported on a 2-lane paved, flat roadway that was in good condition. The speed limit was 55 mph. On the day of the incident the investigating police could not detect an obstacle that could have impaired the driver’s vision. The overpass was measured at 17 feet 2 inches above the ground; the height of the truck with its load was 14 feet 1 inch.
The victim’s employer was contracted by the owner of the loader to move it to another location. The loader driver drove the loader onto the trailer bed and, with the assistance of the victim, centered the loader on the trailer. According to the police report, the loader driver shut down the engine, placed the transmission in neutral and set the parking brake. The loader driver stayed with the victim as he attached chains to one side of the truck. MIFACE did not interview the front-end loader driver, so it is unknown if the loader bucket was wedged against the trailer or where the securing chains were attached.

|
|
Figure 2. Road where incident took place
|
The victim placed at least four 3/8-inch chains onto the loader. The police pictures taken at the scene identified two known points of attachment on the loader. One point of attachment was on the mechanic’s ladder and the other attachment was on a designated loader attachment point. The other exact chain locations are unknown as all chains broke when the load shifted. The attachment points appeared to be to the trailer deck, not the trailer’s “D” rings. Five ratchet binders were used to tighten the chain slack or used as attachment points to the trailer.
The incident occurred approximately 1½ miles from the loading site. The victim was traveling west on the road. Police state that it appears from skid marks on the roadway that the victim was applying the brakes. A witness traveling eastbound noticed that the truck appeared to be slowing down. The incident occurred between the two bridges in Figure 2. As the witness neared the truck, a piece of chain and binder broke away from the load. The witness stopped his vehicle and called 911. When the load shifted and the chains broke, the loader rolled over the 5th wheel and onto the tractor cab. The trailer’s passenger side wheels came to rest on the gravel portion on the side of the roadway. The victim was trapped in the cab. Emergency response arrived and the victim was declared dead at the scene.
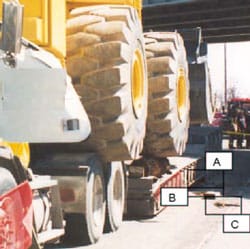
Police noted several chains and binders on the ground on each side of the trailer. The police located three ratchet binders and one chain on the passenger side of the truck’s trailer. Figure 3 shows the chain and binder locations on the passenger side. One binder with a broken hook was found at the rear of the trailer (Box A). One binder/chain with a broken chain link were found at the middle of the trailer (Box B). One binder was located at the front of the trailer (Box C). Figures 4–5 show a close-up view of the binder with the broken hook noted in Figure 3 , Box A.
During their investigation, police found fresh scratches on the middle of the trailer decking. There were no fresh marks or scratches on the “D” rings. The box in Figure 6 outlines the chain or binder marks.
On the driver’s side of the vehicle, Figure 7 shows the chains and binders found on the ground. One long chain was found at the rear of the trailer. (Box A and Figure 8) Another chain and binder were located at the middle of the trailer (Box B, and Figure 9). A binder was found toward the front of the trailer (Box C).
Broken chains were also attached to the loader. One chain appeared to be attached to the mechanic’s ladder (See Figure 10) on the passenger side of the truck. Two chains were attached to the loader bucket (Figure 11). It is unknown if the chains on the bucket were used for securing the loader or if they were used earlier and prior and were not taken off the loader prior to transport. One chain is attached to an attachment point on the loader (See Figure 12).
It is unknown if the timber seen in Figures 3,7,8 and 11 was used for blocking or was being transported on the trailer from one site to another.









After the incident, the company had an outside consultant provide employee training in the proper securement of loads.
During the MIFACE visit, the company representative arranged for a lowboy trailer that was loaded with a piece of heavy machinery to be driven to the company headquarters so the MIFACE representative could see how a load should be secured. The loader blade was retracted and wedged against the trailer end. The individual who secured the load on the trailer stated he was trained by the victim and also by a trade association representative on proper load securement procedures. Figures 13 and 14 show that the loader was not properly secured on the trailer bed. Figures 13 and 14 were taken looking down the driver’s side of the trailer. Figure 13 shows that one of the chains used to secure the load is improperly attached to the trailer bed. Figure 14 shows proper attachment to the “D” ring, but improper loader attachment.

|
 |
|
Figure 13. Improper attachment of loader to trailer bed
|
Figure 14. Proper attachment to “D” ring
|
CAUSE OF DEATH
The cause of death as stated on the death certificate was blunt force head and neck trauma. No alcohol or drugs of abuse were found in the victim’s blood or urine.
RECOMMENDATIONS/DISCUSSION
- Companies should require and train employees to use manufacturer identified cargo attachment points and “D” rings on the trailer using the appropriate number of tiedown assemblies.
This fatality occurred prior to the promulgation of the new cargo securement rules. The Federal Motor Carrier Safety Administration (FMCSA), Rule 393.130, went into effect December 26, 2002. The rule required mandatory compliance as of January 1, 2004. This rule requires the following actions when securing heavy vehicles for transport: (1) Accessory equipment, such as hydraulic shovels, must be completely lowered and secured to the vehicle, (2) Articulated vehicles restrained in a manner that prevents articulation while in transit, (3) heavy equipment with crawler tracks or wheels must be restrained against movement in the lateral, forward, rearward and vertical direction using a minimum of four tiedowns, and (4) Each of the tiedowns must be affixed as close as practicable to the front and rear of the vehicle, or mounting points on the vehicle that have been specifically designed for that purpose.
The victim did ensure that the loader’s hydraulic bucket (accessory equipment) was completely lowered to the trailer bed. It is unknown if the chains on the bucket were intended to secure the bucket to the trailer and to prevent articulation in transit.
The load was not adequately secured against longitudinal (forward/rearward) and lateral movement. See Figure 15. Protecting against longitudinal movement insures the cargo remains on the vehicle and does not penetrates the vehicle’s front-end structure. Protection against lateral movement insures the load does not shift sideways in transit.
The working load limit (WWL) of a tie down, associated connector or attachment mechanism is the lowest working load limit of any of its components (including tensioner) or the working load limit of the anchor points to which it is attached, whichever is less. The WWL is determined by using either the tiedown manufacturer’s markings or by using the tables in the Federal Motor Carrier Safety Administration tables found in 393.108. The tables should be used when the manufacturer does not mark the working load limit of the tiedown material.

|
|
Figure 15. Lateral movement of loader
|
The aggregate working load limit of the tiedown assemblies used to secure an article against movement in any direction must be at least ½ times the weight of the article. The working load limit of the chains used by the victim were 6,600 pounds each, therefore, the chain theoretically could secure an item weighing 13,200 pounds. If the victim used four chains, each with a WWL of 6, 600 pounds, the aggregate working load limit would have been 26,400 pounds. If four chains were used, the load could not have weighed more than 52, 800 pounds. At least 5 chains were required if the loader weighed 60,000. When MIFACE spoke with the truck driver at the site visit, this individual indicated concern that attaching chain through the trailer’s “D” rings places strain on the chain links due to the chain bending around the trailer bed. Companies should stress that attaching binders to the trailer bed does not prevent the binder hook from sliding along the bed. Hook movement on the bed can result in load movement, placing greater strain on the tiedown assemblies. Trailers are designed with the “D” ring to provide an attachment point that minimizes chain slack and the resulting load movement on the trailer bed during transport.
To properly secure a load to the trailer, the tiedown assemblies must be properly attached to the load itself, as well as to the “D” rings on the trailer. If it is unknown where on the load the tiedown assemblies should be attached, or if the piece of equipment does not have readily identifiable attachment points for the tiedown assembly, companies should contact the manufacturer to obtain the manufacturer’s recommended attachment points.
Reinforcement of the best practices for load securement serves to remind both experienced and novice workers that they must never become complacent. The victim had many years of experience in securing heavy loads. Familiarity with a task often leads to a lax attitude regarding the steps to be followed to perform a job safely. Appropriate consideration given to the type and value of the training can also indicate to the workers that working safely is viewed as an important element of the job and safety, not simply being given lip service.
Even after safety training, there is no guarantee that safe practices will be followed. Job demands and previous use of shortcuts may be an encouragement for employees to go back to the “shortcut” way of performing the work. The employee may use his/her past experience is a guide – he/she may have done the work successfully and injury free using the shortcut. Companies that permit, encourage, allow, fail to identify and correct these inappropriate behaviors reinforce that behavior and give tacit approval to the unsafe action. The company’s safety culture, i.e., the safety attitudes, beliefs and behaviors that are generally shared within the organization, must have attention to safety in all activities. Management must demonstrate a commitment to safety and make it a high priority. Management must supervise the work of individuals and provide positive reinforcement for safe behaviors and negative consequences for unsafe behaviors. Employees must be aware of the importance of safety in their actions and be knowledgeable and competent to perform their jobs.
- Companies should ensure that consistency is maintained with the working load limits of all components of a tiedown assembly.
Company personnel indicated that the company has upgraded from 3/8-inch chains to ½-inch chains. See Figure 16. The entire tiedown assembly is only as strong as its weakest component. When upgrading, the company must take the next necessary step to ensure that the chain upgrade does not exceed the working load limit of any of the other components of the assembly, such as the hooks, tensioner, “D” rings, equipment attachment points, etc.

|
|
Figure 16. Storage area holding ½ inch chains
|
- Companies should ensure all components of a tiedown assembly are inspected for defects and correlate in size while securing each load.
On the day of the incident, it appears that the victim used a grab hook with a throat too big for the 3/8-inch chain link. See Figure 17. The chain links would not fit securely inside of the throat and could possibly slip during transport.
FMCSA Rule 393.104 states that all vehicle structures, systems, parts, and components including vehicle tiedown anchor points used to secure cargo must be in proper working order when used to perform that function with no damaged or weakened components that will adversely effect their performance for cargo securement purposes, including reducing the working load limit and must not have any cracks or cuts. Company personnel indicated that they routinely check the chains for stretched links by laying the chain out and measuring. According to a company worker, chains normally don’t stretch; they break. The workers do not routinely check for damaged chain links, damaged transport vehicle anchor points, or damage to the anchor points on the load. MIFACE recommends that the company require drivers who transport loads to check all components of the tiedown assembly during securement to ensure all components are in proper working order.

|
|
Figure 17. Oversized hook, driver’s side
|
- Additionally, MIFACE recommends that all employers develop standard operating procedures and provide employee training to educate workers about the January 2004 FMCSA new cargo securement rules.
Effective in January 2004, the securement of heavy vehicles, equipment and machinery which operate on wheels or tracks and which individually weigh 10,000 pounds or more must be restrained against movement in the lateral (sideways), forward, rearward and vertical direction using a minimum of four tiedowns. Each of the tiedowns must be affixed as close as practicable to the front and rear of the vehicle or mounting points on the vehicle that have been specifically designed for that purpose.
Standard operating procedures (SOPs) provide many benefits to a company. Among the benefits are: removing variation in work performance caused by different people doing the same job, facilitate employee job training as well as cross-training, provide a common understanding of the job and expectations for job performance, help to provide a safe work environment by assessing hazards and risk and providing ways to minimize the identified hazards/risks, and when written collaboratively between management and workers, provides for employee involvement and buy-in of the scope and intent of the standard operating procedure.
If practical, SOP development and implementation should be a joint effort of the people who are directly affected by it. The scope of the SOP should be defined and named using descriptive words. An overall task description should be developed and each task should be described in detail, keeping the number of steps to complete the task below ten. Implementing the SOP involves testing the SOP draft, communicating with employees about the SOP and training them in the SOP content. A system should be set up to monitor the implementation and use of the SOP to ensure its applicability and ease of use for the worker and operation.
The development of a “load securement” SOP and training associated with the SOP will assist individuals responsible to secure cargo being transported to properly assess the securement requirements of the load, including the number of tie down assemblies required and appropriate load attachment points. The SOP should prohibit the work practice of attaching chain hooks/binders directly to the truck trailer bed.
REFERENCES
- Federal Motor Carrier Safety Administration, 400 7th Street, S.W. Washington, D.C. 20590.
Internet Address: http://www.fmcsa.dot.gov/mission/about-us (Link Updated 4/9/2015)
MIFACE gratefully acknowledges the assistance and expertise of Mr. Michael Irwin, project director for the Michigan Center for Truck Safety in the preparation of this report.
He is accredited as a Certified Director of Safety through the University of Central Florida and the North American Transportation Management Institute. Mr. Irwin was formerly an officer with the Motor Carrier Division of the Michigan State Police and has been with the Michigan Center for Truck Safety since 1996. His past responsibilities at the Michigan Center for Truck Safety have included serving as the interim project director, safety specialist/training coordinator and hot line operator. He has more than 31 years experience in the commercial transportation field as enforcement, towing company manager, mechanic and driver. He currently sits on the Commercial Vehicle Safety Alliance and the Governor’s Traffic Safety Advisory Commission training committees.
MIFACE (Michigan Fatality and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 3/2/04
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
MIFACE
Investigation Report # 02 MI 040
Evaluation
| To improve the quality of the MIFACE program and our investigation reports, we would like to ask you a few questions regarding this report. | |||
| Please rate the following on a scale of: | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| What was your general impression of this MIFACE investigation report? | |||
| Excellent | Good | Fair | Poor |
| 1 | 2 | 3 | 4 |
| Was the report… | Excellent | Good | Fair | Poor |
| Objective? | 1 | 2 | 3 | 4 |
| Clearly written? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| Were the recommendations … | Excellent | Good | Fair | Poor |
| Clearly written? | 1 | 2 | 3 | 4 |
| Practical? | 1 | 2 | 3 | 4 |
| Useful? | 1 | 2 | 3 | 4 |
| How will you use this report? (Check all that apply) | |
| O | Distribute to employees |
| O | Post on bulletin board |
| O | Use in employee training |
| O | File for future reference |
| O | Will not use it |
| O |
Other (specify) __________________________________________ |
Thank You!
Please Return To:
MIFACE
Michigan State University
117 West Fee Hall
East Lansing, MI 48824
FAX: 517-432-3606
Comments:
| If you would like to receive e-mail notifications of future MIFACE work-related fatality investigation report summaries, please complete the information below. | |
| Name: __________________________________________ | |
| e-mail address: ___________________________________ | |
| I would like to receive summaries for reports involving: | |
| ___ Construction | ___ Agriculture |
| ___ Manufacturing | ___ All |