
Massachusetts Stock Clerk Dies from Fall Out of a Tipped Vertical Lift
Investigation: # 00-MA-003-01
Release Date: January 5, 2001
SUMMARY
On January 11, 2000, a 34-year-old male stock clerk (the victim) was fatally injured when he fell approximately 15 feet from the platform of a manual electric vertical hydraulic lift while placing a generator onto a shelf. The force from pushing the generator from the lift platform to the shelf was great enough to tip the lift, which landed partially upright against an adjacent row of shelving. The victim was not wearing the available company-required fall protection equipment, which consisted of a body harness and lanyard. The co-worker who found the victim went to get help and placed a call for emergency assistance. The local police and fire departments arrived and transported the victim to a local hospital. He was then moved to a larger hospital in a nearby city where he was pronounced dead. The MA FACE Program concluded that to prevent similar occurrences in the future, employers should:
- Match new equipment to the tasks before implementing it into daily activities.
- Develop a standard operating procedure (SOP) for new equipment before introducing the equipment into daily activities.
- Train all employees in the proper and safe use of equipment and how to complete tasks.
In addition, manufacturers of vertical lifts should:
- Inform purchasers and operators of the potential tipping hazard of narrow lifts.
INTRODUCTION
On January 12, 2000, the MA FACE Program was notified by the Occupational Safety and Health Administration (OSHA) that on January 11, 2000, a 34-year-old male stock clerk had been fatally injured when he fell approximately 15 feet from the platform of a manual electric vertical hydraulic lift while placing a generator on a shelf. An investigation was immediately initiated. The MA FACE Program Director traveled to the location of the home improvement warehouse store on February 8, 2000 where the store manager, health and safety representative, and a co-employee of the victim were interviewed. The police report, death certificate, corporate information, OSHA fatality/catastrophe report, interviews, and pictures were obtained during the course of the investigation.
The employer, a home improvement warehouse store, was in business approximately 22 years and had operated the site involved in the incident for approximately 6 years. The company had stores in 4 countries including 45 stores in the United States. At the site of the incident, the company employed approximately 250 people and approximately 10 of these employees worked the overnight shift. One other overnight shift employee worked in the hardware section along with the victim. The company had a designated safety representative at the store location and written safety procedures along with scheduled safety meetings twice a month. The safety topics brought up at these meetings would then be discussed at staff meetings.
The victim had been employed by the company for approximately three years. He started out in sales in the hardware and garden departments and switched to the overnight shift as a stock clerk approximately one and a half years ago. Training consisted of classroom training, including videos and written material that was updated yearly, along with on-the-job training. Employee proficiency with equipment was demonstrated through written exams and observations during the use of equipment. The company certified employees to use most equipment such as forklifts and order pickers, but did not certify for the use of the manual electric vertical hydraulic lift, which was involved in the incident. There is no union representation at this company.
INVESTIGATION
On the night of the incident, the overnight shift crew of the home improvement warehouse store were performing their typical tasks, including restocking shelves. The store contained approximately 120,000 square feet of retail space not including the garden center. The building’s ceiling was approximately 25 feet high in the middle and at the edges it sloped down to approximately 20 feet in height. The main section of the store contained rows of approximately 16-foot high shelving. The shelves were not consistently vertically spaced but spaced at distances best suited to the objects being stored. Heavy and/or large objects would be placed on pallets for the use of forklifts or order pickers to stock the shelves.
The lift, involved in the incident, a manual electric vertical hydraulic lift, was not motorized and was pushed by the operator to the desired location. It had four-wheels, was battery operated with a maximum lifting height of 14 feet 10 inches, and was rated to lift a maximum of 500 pounds total, including the operator and any objects onboard. Two footpads were located next to the rear wheels, when lowered, they took the weight off the rear wheels, preventing the lift from rolling during use. The footpads must be in the down position and locked for the lift to operate. The lift was equipped with a level sensor that prevented the lift from rising if it were on a slope greater than 1 degree.
The base dimensions of the lift were 2 feet 6½ inches wide by 5 feet 11 inches long by 6 feet 5 inches high. The dimensions of the operator’s area were 2 feet 5 inches wide by 4 feet 2 inches long. The operator’s area was used to temporarily store objects that were being raised. The operator’s area was equipped with a safety cage, which consisted of two movable sections that were 3 feet 6 inches high. The control panel located at the front of the operator’s area acted as the third side of the safety cage. This design left one side of the operator’s safety cage open at all times. The lift had an anchor point located below the control panel for the use of a lanyard.
At the time of the incident, this style of lift involved had been integrated into the company’s daily activities for approximately seven months. The investigation revealed that these lifts were being used in place of 12-foot stepladders. A store employee performed daily, weekly, and monthly equipment maintenance checks on equipment, while an outside company conducted any required maintenance work to the equipment.
The company developed a training program for the lift and distributed it to the individual stores. Each store provided the training to employees without any input or modification to the program. The training provided employees with information on how to operate the lift including use of the footpads, lanyard, controls, and information about the specified weight limit. However, the training did not include procedures to prevent tipping.
At the time of the incident, the victim was working the overnight shift as a stock clerk in the hardware section located at the front of the store. His main task consisted of restocking the hardware items that accumulated on the floor and other locations during the day. A co-employee was also working in the hardware section but he did not witness the incident. The remaining onsite employees were on break in the break room located at the rear of the store.
An uncrated generator that weighed 247 pounds was one of the objects placed on the floor of the hardware section during the previous day. Alone, the victim loaded the generator onto the lift to restock the generator back to the top shelf. Once the generator was loaded onto the lift, only a small area approximately 1 foot long and 2 feet 5 inches wide remained for the victim to operate the lift and maneuver the generator onto the shelf. The victim raised the lift to the maximum lifting height of 14 feet 10 inches with the open side of the operator’s cage toward the shelf he was accessing. Although unwitnessed, the evidence indicates that the force being applied against the raised lift while maneuvering the generator up onto the shelf, which was 16 feet high, caused the lift to tip away from the shelf. The victim was not wearing the company required fall protection equipment (body harness and lanyard) fell over the top of the operator’s area safety rail and fell approximately 15 feet to the floor below as the lift tipped. The lift landed partially upright against an adjacent shelf.
The co-employee working in the hardware section heard a noise from the aisle where the victim was working and went to find out what had caused it. He found the victim lying on the floor next to the generator. The co-employee went to the break room to get the nightshift manager and called for emergency assistance. The local police and fire departments arrived and transported the victim to a local hospital. Then the victim was transported to a larger hospital in a nearby city where he was pronounced dead.
The store manager stated that to place a large and heavy object, such as the generator involved in the incident, onto a shelf, an order picker forklift should have been used. It was also revealed that, the victim, by his own choice was not certified by the company to use self-propelled style equipment such as an order picker forklift due to a medical condition. In addition, it was revealed that the victim had previously failed to wear fall protection equipment and that a few days before the incident, the store manager had spoken to him about the need to use fall protection when operating the lift.
CAUSE OF DEATH
The medical examiner listed the cause of death as blunt head trauma.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should develop a standard operating procedure (SOP) for new equipment before introducing the equipment into daily activities.
Discussion: Employees of the store were trained on how to operate the lift, but the training program did not include a standard operating procedure (SOP). A SOP stating exactly how to use this type of lift is important and should be developed and implemented. It could help prevent tipping incidents by including guidelines to assist the employees in operating the equipment correctly and knowing the size, weight, and quantity limits of objects that can be handled while using the lift.
To protect against tipping a SOP should include but not be limited to:
- Weight limits for an object or objects being raised by the lift. The weight limits should take into consideration how much weight an employee can physically lift up and place down in a desired location.
- Height limits for the maximum shelf height an operator should access while using the lift.
- Maximum size of an object that can be raised by the lift. This size limit should consider the employee’s ability to safely handle the size of the object, including a light but large object and awkward sized objects.
- The size of the operator’s area should be considered at all times. The object or objects must fit in the operator’s area with the safety cage in place and give the operator enough room to operate the lift and safely maneuver the object and place it in the desired location eliminating the need of the operator to lean over the safety cage.
In this case, the victim was using the lift to raise an object that was too heavy and large to safely maneuver onto the shelf. The size of the object took up most of the operator’s area inside the safety cage leaving him with little room to operate the lift and maneuver the generator to the shelf. Although, the weight of the generator and the victim combined was less than the maximum weight rating provided by the manufacturer, the combination of the lift being fully extended, generator’s weight, and maneuvering the generator exceeded the amount of applied vertical force the lift could handle.
Recommendation #2: Employers should train all employees in the proper and safe use of equipment and how to complete tasks.
Discussion: Employers should provide training for all employees in the proper and safe use of equipment and how to complete tasks. Employee training should include the SOP for each piece of equipment and written task specific safety procedures. The training should be updated with employees’ input annually, when safety concerns arise and when new equipment and new tasks are going to be introduced into the workplace. Also, employers should make clear to employees that when performing tasks if they come across an element of that task which requires the use of equipment they are not trained or certified to operate then they would not be expected to accomplish that task.
Involving employees when updating their training is important. The employer should ask the employees about and evaluate possible hazards associated with equipment and techniques involved in completing their tasks. Employees will know the most about the effectiveness, limitations, and inconveniences of the equipment and procedures to complete tasks.
In addition, the employee training should cover personal protective equipment. The company had a standard that required the use of fall protection equipment which in this case, would had helped minimized the injuries because when the lift tipped it landed partially upright against the adjacent shelf. However, this type of fall protection system is not designed to save a person if the lift tips, because the lanyard’s anchor point is located on the lift. In most cases with this type of lift and fall protection system, if the operator were wearing fall protection and the lift tipped the operator would fall with the lift to the floor level but with proper training the chances of the lift tipping would be minimized.
Recommendation #3: Manufacturers of vertical lifts should inform purchasers and operators of the potential tipping hazard of narrow lifts.
Discussion: The manufacturer did not make information on the potential tipping hazard of this lift available leaving owners and operators unaware of the hazard. The manufacturer of the lift should include a section on the potential tipping hazard of narrow lifts in the operation and maintenance manual. In addition, by affixing decals on the lift, the manufacturer attempted to inform the operator of other safety hazards. The manufacturer could also attempt to inform the lift owners and operators of the potential tipping hazard by placing an additional decal on the lift in clear view of the operator.
REFERENCES
Code of Federal Regulations, 29 CFR 1910.67 (c)(2)(ii), Vehicle-mounted elevating and rotating work platforms.
American National Standards Institute, Manually Propelled Elevating Work Platforms, ANSI A92.3, New York.
Equipment Manufacturers Institute, Aerial Platforms, Chicago, Illinois, Revised 1995.

Figure 1 – Manual Electric Vertical Hydraulic Lift (side view)
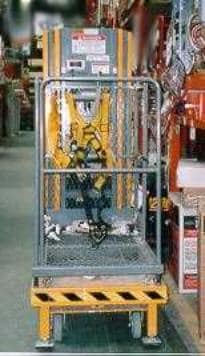
Figure 2 – Manual Electric Vertical Hydraulic Lift
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.