
A Forklift Operator Died When He Was Crushed in the Mast of a Forklift.
California Case Report: 04CA012
Summary
A 23-year-old Hispanic forklift operator died when he was crushed in the mast structure of a forklift while unloading cargo on pallets from a truck trailer. The victim was found leaning forward over the forklift’s steering wheel with his right leg against the forklift controls and his head in between the beams of the inner and outer masts. The CA/FACE investigator determined that in order to prevent future occurrences employers, as part of their Injury and Illness Prevention Program (IIPP), should:
- Ensure employees who operate forklifts do not extend any part of their body outside of the operator’s compartment while the forklift is running.
- Ensure employees who operate forklifts wear their seatbelts while the forklifts are running.
In addition, manufacturers of forklifts and/or employers should consider:
- Installing additional safeguards to protect forklift operators.
Introduction
On September 2, 2004, at approximately 4:20 a.m., a 23-year-old Hispanic machine forklift operator died when his head was crushed in a forklift mast. The victim was found bent over the forklift steering wheel with his right leg against the forklift controls. The CA/FACE investigator learned of this incident on September 2, 2004, by a faxed report from a district office of the Division of Occupational Safety and Health (Cal/OSHA). Contact with the victim’s employer was made on December 14, 2004, and the CA/FACE investigator was immediately referred to the employer’s legal counsel. On April 11, 2005, the CA/FACE investigator traveled to the facility where the incident occurred and interviewed the company’s management and the victim’s co-workers. The machine involved in the incident and the area where the incident took place were photographed and inspected.
The employer of the victim was a trucking company that hauls freight nationwide. The company had been in business for 75 years and had 1,400 employees nationwide. The facility where the incident took place employed 286 people. The victim had been employed approximately one and a half years with the company when the incident occurred. The victim was born in the United States and was of Hispanic descent. He spoke fluent English as well as Spanish. The victim was a high school graduate and had attended some college.
The company had a written safety program printed in English. The program had written safe work procedures for employees to follow. Safety meetings were held weekly and were documented. The company had a training program that provided specific training to its employees. The training program for forklift operators consisted of a combination of classroom, video, and on-the-job training. Training was measured by testing and observation.
Investigation
The site of the incident was a truck depot for the company where trucks exchange cargo for shipping. The machine involved in the incident was a forklift designed to enter the enclosed beds of trailers. The forklift was equipped with a seat belt. The forklift mast consisted of an outer mast which was stationary and an inner mast which was telescopic.
On the morning of the incident, the victim was using a forklift to unload a trailer of cargo stored on pallets. A co-worker was walking by the trailer and noticed the stopped forklift and the victim leaning forward out of the forklift seat. Approximately five minutes later, the same co-worker walked by the trailer again and noticed the victim in the identical position as before. The co-worker found the victim trapped in the mast of the forklift with the engine still running. The co-worker contacted the supervisor who immediately called 911. No one attempted to move the victim for fear of causing further injuries. The police were the first to arrive on the scene and asked company employees for assistance in removing the victim from the forklift in order to perform CPR. The paramedics arrived on scene and started treating the victim, then transported the victim to a local hospital where he was pronounced dead in spite of resuscitative efforts.
Although the incident was not witnessed, the position of the victim’s body suggests that as he leaned forward and stuck his head between the beams of the outer and inner forklift mast, his right leg pushed the control lever forward. This caused the inner mast to come down on the victim’s head before he could move out of the way.
Cause of Death
The cause of death, according to the death certificate, was blunt neck trauma with traumatic asphyxia.
Recommendations/Discussion
Recommendation #1: Ensure employees who operate forklifts do not extend any part of their body outside of the operator’s compartment while the forklift is running.
Discussion: The operation and maintenance manual for this forklift states that the operator shall “never place any part of the body into the mast structure, between mast and truck, or outside the truck.” It is not known why the victim leaned through the mast. Possible causes include lack of exposure to safe work principles, incomplete or lack of testing and evaluation to show understanding of those lessons, or inconsistent/incomplete programs to ensure implementation of those principles. Safe work practices can be enhanced through programs of task-specific training, supervision, safe work recognition, and progressive disciplinary measures.
Recommendation #2: Ensure employees who operate forklifts wear their seat belts while the forklifts are running.
Discussion: In this incident the victim was not wearing a seat belt while the forklift was running. This allowed him to lean forward into the mast structure. The operator of a forklift should always keep his/her seat belt fastened until the forklift is shut down. In this incident, if the forklift operator had kept his seat belt fastened, he would have been unable to lean into the mast structure.
Recommendation #3: Manufacturers and employers should consider installing additional safeguards to protect forklift operators.
Discussion: There are several devices which may have prevented this incident if they had been installed on the forklift. A screen (clear plastic or metal grate) in front of the forklift operator cabin would have prevented the operator from reaching forward between the masts. A safety interlock that requires the operator to engage two controls before moving the forks would have kept the mast from descending on the victim. A pressure interlock under the operator seat would have locked the controls in place when the pressure on the seat was released, or a sensor device could be attached to the seat belt of the forklift that when disconnected would shut off the power to the forklift. These are just some devices that, if installed on the forklift, might have prevented this incident from occurring.
Reference
California Code of Regulations, Vol. 9, Title 8, Sections 3664, 3668
Exhibits
 |

|
|
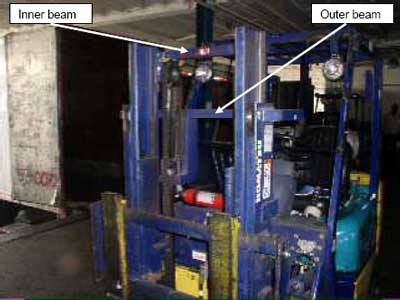
Exhibit #2: A picture of the forklift mast showing where the victim placed his head. |
California Fatality Assessment and Control Evaluation (FACE) Project
The California Department of Health Services, in cooperation with the Public Health Institute and the National Institute for Occupational Safety and Health (NIOSH), conducts investigations of work-related fatalities. The goal of this program, known as the California Fatality Assessment and Control Evaluation (CA/FACE), is to prevent fatal work injuries in the future. CA/FACE aims to achieve this goal by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact. NIOSH-funded, state-based FACE programs include: Alaska, California, Iowa, Kentucky, Massachusetts, Michigan, Minnesota, Nebraska, New Jersey, New York, Oklahoma, Oregon, Washington, West Virginia, and Wisconsin.
To contact California State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.