National Overview of Acute Flaccid Myelitis—United States, 2014–2018
CDC epidemiologic overview
Also available as Printable PDF pdf icon[PDF – 397 KB]
Slide 1

National Overview of Acute Flaccid Myelitis — United States, 2014–2018
National Center for Immunization & Respiratory Diseases
Manisha Patel, MD MS
Measles, Mumps, Rubella, Herpesvirus and Domestic Polio Epidemiology Team Lead
Board of Scientific Counselors
December 6, 2018
Slide 2
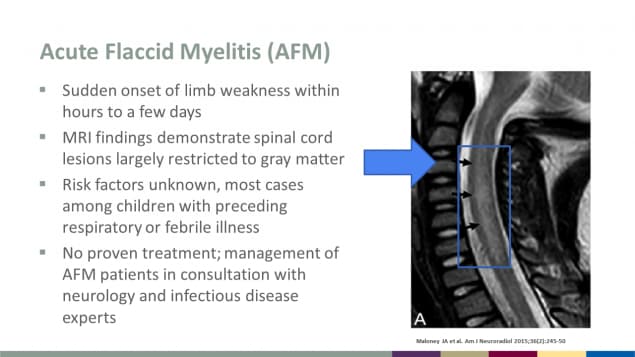
Acute Flaccid Myelitis (AFM)
- Sudden onset of limb weakness within hours to a few days
- MRI findings demonstrate spinal cord lesions largely restricted to gray matter
- Risk factors unknown, most cases among children with preceding respiratory or febrile illness
- No proven treatment; management of AFM patients in consultation with neurology and infectious disease experts
Reference for photo: Maloney JA et al. Am J Neuroradiol 2015;36(2):245-50
Slide 3
Initial investigations of AFM in the United States
- 2012, CA: Three patients with limb weakness and anterior myelitis on MRI within 1 month
- Total of 23 patients identified from 2012–2014
- 2014, CO: Nine patients with limb weakness and spinal cord gray matter lesions with onset dates August–September
- 2014: A national call for additional cases confirmed 120 cases in 34 states from Aug–Dec
More than 5 cases reported from CA, CO, MA, PA and UT
Ayescue, MMWR, 2014; Pastula, MMWR, 2014; Van Haren, JAMA, 2015; Sejvar, CID, 2016
Slide 4

Evolution of the case definition for AFM
- 2014: Confirmed case of AFM – Acute onset of limb weakness and magnetic resonance image (MRI) showing a spinal cord lesion largely restricted to gray matter in a patient ≤21 years of age.
- Sept 26, 2014: HAN to call for national reporting
- 2015: Added a probable case definition
- June 2015: CSTE adopted standardized case definition
- 2017: Confirmed case of AFM – Acute onset of flaccid limb weakness, AND an MRI showing a spinal cord lesion largely restricted to gray matter and spanning one or more spinal segments. Probable case of AFM – Acute onset of focal limb weakness, AND cerebrospinal fluid (CSF) with pleocytosis (white blood cell count >5 cells/mm3).
- June 2017: CSTE adopted revisions to case definition
Slide 5
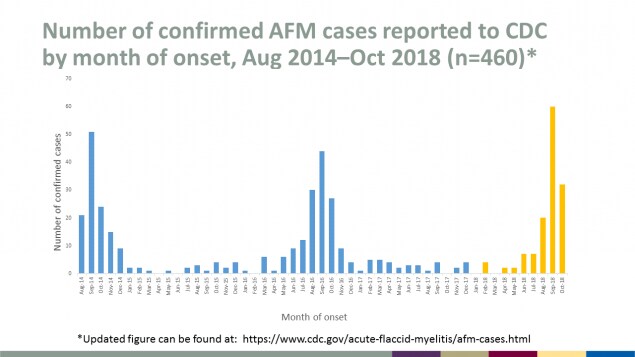
Number of confirmed AFM cases reported to CDC by month of onset, Aug 2014–Oct 2018 (n=460)
Updated figure with data for case counts can be found at AFM Confirmed U.S. Cases.
Slide 6
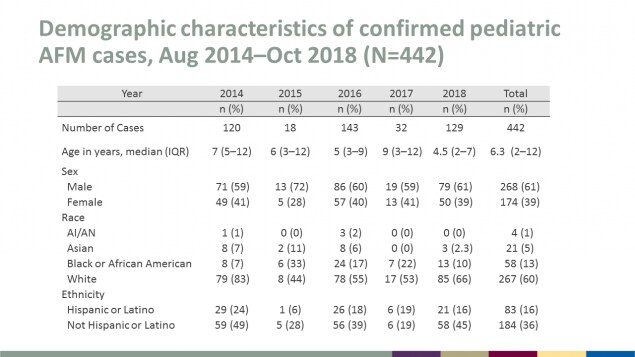
Demographic characteristics of confirmed pediatric AFM cases, Aug 2014–Oct 2018 (N=442)
| Demographic Characteristic | 2014 n (%) |
2015 n (%) |
2016 n (%) |
2017 n (%) |
2018 n (%) |
Total n (%) |
|---|---|---|---|---|---|---|
| Number of Cases | 120 | 18 | 143 | 32 | 129 | 442 |
| Age in years, median (IQR) | 7 (5–12) | 6 (3–12) | 5 (3–9) | 9 (3–12) | 4.5 (2–7) | 6.3 (2–12) |
| Sex | ||||||
| Male | 71 (59) | 13 (72) | 86 (60) | 19 (59) | 79 (61) | 268 (61) |
| Female | 49 (41) | 5 (28) | 57 (40) | 13 (41) | 50 (39) | 174 (39) |
| Race | ||||||
| AI/AN | 1 (1) | 0 (0) | 3 (2) | 0 (0) | 0 (0) | 4 (1) |
| Asian | 8 (7) | 2 (11) | 8 (6) | 0 (0) | 3 (2.3) | 21 (5) |
| Black or African American | 8 (7) | 6 (33) | 24 (17) | 7 (22) | 13 (10) | 58 (13) |
| White | 79 (83) | 8 (44) | 78 (55) | 17 (53) | 85 (66) | 267 (60) |
| Ethnicity | ||||||
| Hispanic or Latino | 29 (24) | 1 (6) | 26 (18) | 6 (19) | 21 (16) | 83 (16) |
| Not Hispanic or Latino | 59 (49) | 5 (28) | 56 (39) | 6 (19) | 58 (45) | 184 (36) |
Slide 7
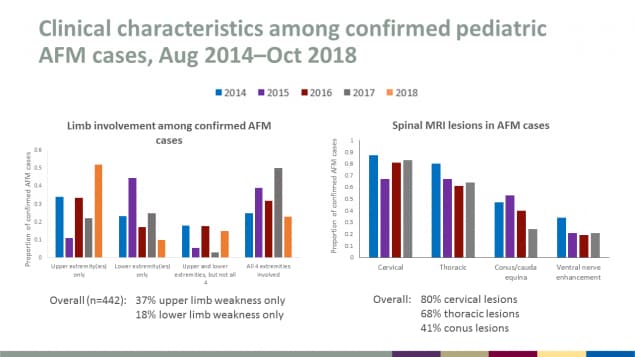
Clinical characteristics among confirmed pediatric AFM cases, Aug 2014–Oct 2018
Limb involvement among confirmed AFM cases
Overall (n=442): 37% upper limb weakness only; 18% lower limb weakness only
Spinal MRI lesions in AFM cases
Overall: 80% cervical lesions; 68% thoracic lesions; 41% conus lesions
Slide 8
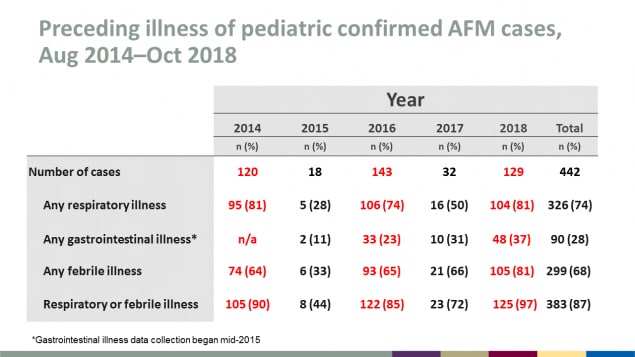
Preceding illness of pediatric confirmed AFM cases, Aug 2014–Oct 2018
| Preceding Illness | 2014 n (%) |
2015 n (%) |
2016 n (%) |
2017 n (%) |
2018 n (%) |
Total n (%) |
|---|---|---|---|---|---|---|
| Number of cases | 120 | 18 | 143 | 32 | 129 | 442 |
| Any respiratory illness | 95 (81) | 5 (28) | 106 (74) | 16 (50) | 104 (81) | 326 (74) |
| Any gastrointestinal illness* | n/a | 2 (11) | 33 (23) | 10 (31) | 48 (37) | 90(28) |
| Any febrile illness | 74 (64) | 6 (33) | 93 (65) | 21 (66) | 105 (81) | 299 (68) |
| Respiratory or febrile illness | 105 (90) | 8 (44) | 122 (85) | 23 (72) | 125 (97) | 383 (87) |
*Gastrointestinal illness data collection began mid-2015
Slide 9
AFM diagnostic testing, Aug 2014–Nov 2018
- Cerebrospinal fluid
- EV-D68, EV-A71, Coxsackievirus A16 in 4 confirmed cases
- Metagenomics testing in 2014 of 14/35 CSF: GB virus C, human rhinovirus, transfusion-transmitted virus
- Upper respiratory specimen positivity varied
- 20-30% EV-D68+ during peak years
- EV-D68 also detected in patients later classified as non-cases
- Approximately one-third specimens with other viruses detected, some co-infections
- Approximately one-third specimens with no pathogen detected
- All stool tested negative for poliovirus by standard WHO methods
Slide 10
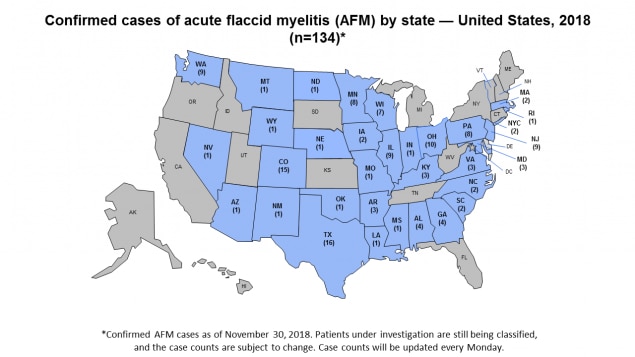
Confirmed cases of acute flaccid myelitis (AFM) by state — United States, 2018 (n=134)
Confirmed AFM cases as of November 30, 2018. Patients under investigation are still being classified, and the case counts are subject to change. Case counts will be updated every Monday at AFM Cases in the U.S.
Slide 11
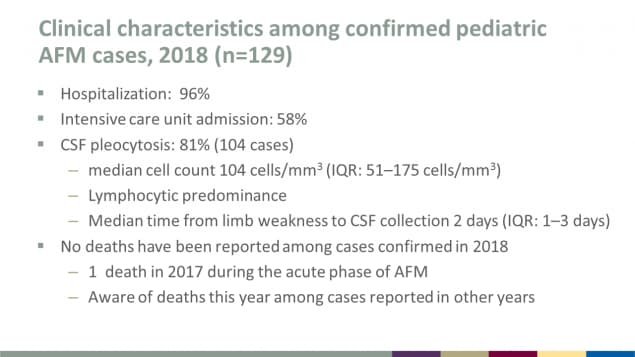
Clinical characteristics among confirmed pediatric AFM cases, 2018 (n=129)
- Hospitalization: 96%
- Intensive care unit admission: 58%
- CSF pleocytosis: 81% (104 cases)
- Median cell count 104 cells/mm3 (IQR: 51–175 cells/mm3)
- Lymphocytic predominance
- Median time from limb weakness to CSF collection 2 days (IQR: 1–3 days)
- No deaths have been reported among cases confirmed in 2018
- 1 death in 2017 during the acute phase of AFM
- Aware of deaths this year among cases reported in other years
Slide 12
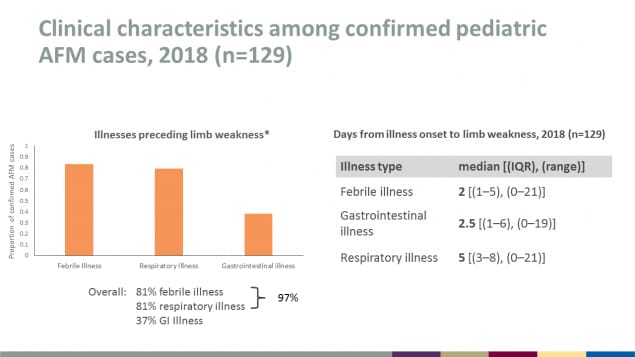
Clinical characteristics among confirmed pediatric AFM cases, 2018 (n=129)
Illnesses preceding limb weakness
Overall: 81% febrile illness; 81% respiratory illness; 37% GI Illness
(Febrile illness and respiratory illness combined is 97%)
Days from illness onset to limb weakness, 2018 (n=129)
By illness type, media [(IQR), (range)]:
- Febrile illness, 2 [(1–5), (0–21)]
- Gastrointestinal illness, 2.5 [(1–6), (0–19)]
- Respiratory illness, 5 [(3–8), (0–21)]
Slide 13
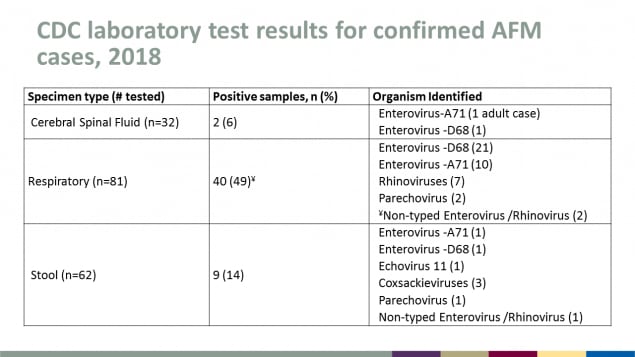
CDC laboratory test results for confirmed AFM cases, 2018
| Specimen type (# tested) |
Positive samples n (%) |
Organism Identified |
|---|---|---|
| Cerebral Spinal Fluid (n=32) | 2 (6) | Enterovirus-A71 (1 adult case) Enterovirus-D68 (1) |
| Respiratory (n=81) | 40 (49)* | Enterovirus-D68 (21) Enterovirus-A71 (10) Rhinoviruses (7) Parechovirus (2) *Non-typed Enterovirus / Rhinovirus (2) |
| Stool (n=62) | 9 (14) | Enterovirus-A71 (1) Enterovirus-D68 (1) Echovirus 11 (1) Coxsackieviruses (3) Parechovirus (1) Non-typed Enterovirus / Rhinovirus (1) |
Slide 14
Summary
- Despite the increase in cases this year, AFM is still a rare disease
- Predominately a pediatric illness
- Every-other-year rise continues to be observed
- Limited data suggests new epidemiology since 2014
- Cases reported in 44 states since 2014
- Greater than 85% with a preceding febrile or respiratory illness
- Virus detected in 50% of respiratory specimens
- Among 4 confirmed cases since 2014, 3 different viruses identified in CSF
- Unclear if direct viral invasion of spinal cord versus post-infectious process
- Limited biopsy or tissue specimens to look at pathology
Slide 15

Acknowledgments
Janell Routh, Adriana Lopez, Adria Lee, Tracy Ayers, Anita Kambhampati, Margaret Cortese, Jim Sejvar, Sarah Hopkins, Dan Pastula, Howard Lipton, Steve Oberste, Will Weldon, Jennifer Anstadt, Alan Nix, Shannon Rogers, Sue Tong, Laurence Briesach, Kimbell Hetzler, Heather Jost, Jessica Ciomperlik, Mark Pallansch, Glen Abedi, Susannah McKay, Brian Emery, Cate Otten, AFM Response Team, State and local health departments, Sue Gerber and the EV Team, External AFM collaborators
Slide 16
Thank You
For more information, contact CDC:
1-800-CDC-INFO (232-4636)
TTY: 1-888-232-6348
CDC.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.