Trichinellosis Surveillance — United States, 2008–2012
Corresponding author: Susan P. Montgomery, Division of Parasitic Diseases and Malaria, Center for Global Health. Telephone: 404-718-4731; E-mail: zqu6@cdc.gov.
Abstract
Problem/Condition: Trichinellosis is a parasitic disease caused by nematodes in the genus Trichinella, which are among the most widespread zoonotic pathogens globally. Infection occurs following consumption of raw or undercooked meat infected with Trichinella larvae. Clinical manifestations of the disease range from asymptomatic infection to fatal disease; the common signs and symptoms include eosinophilia, fever, periorbital edema, and myalgia. Trichinellosis surveillance has documented a steady decline in the reported incidence of the disease in the United States. In recent years, proportionally fewer cases have been associated with consumption of commercial pork products, and more are associated with meat from wild game such as bear.
Period Covered: 2008–2012.
Description of System: Trichinellosis has been a nationally notifiable disease in the United States since 1966 and is reportable in 48 states, New York City, and the District of Columbia. The purpose of national surveillance is to estimate incidence of infection, detect outbreaks, and guide prevention efforts. Cases are defined by clinical characteristics and the results of laboratory testing for evidence of Trichinella infection. Food exposure histories are obtained at the local level either at the point of care or through health department interview. States notify CDC of cases electronically through the National Notifiable Disease Surveillance System (available at http://wwwn.cdc.gov/nndss). In addition, states are asked to submit a standardized supplementary case report form that captures the clinical and epidemiologic information needed to meet the surveillance case definition. Reported cases are summarized weekly and annually in MMWR.
Results: During 2008–2012, a total of 90 cases of trichinellosis were reported to CDC from 24 states and the District of Columbia. Six (7%) cases were excluded from analysis because a supplementary case report form was not submitted or the case did not meet the case definition. A total of 84 confirmed trichinellosis cases, including five outbreaks that comprised 40 cases, were analyzed and included in this report. During 2008–2012, the mean annual incidence of trichinellosis in the United States was 0.1 cases per 1 million population, with a median of 15 cases per year. Pork products were associated with 22 (26%) cases, including 10 (45%) that were linked with commercial pork products, six (27%) that were linked with wild boar, and one (5%) that was linked with home-raised swine; five (23%) were unspecified. Meats other than pork were associated with 45 (54%) cases, including 41 (91%) that were linked with bear meat, two (4%) that were linked with deer meat, and two (4%) that were linked with ground beef. The source for 17 (20%) cases was unknown. Of the 51 patients for whom information was reported on the manner in which the meat product was cooked, 24 (47%) reported eating raw or undercooked meat.
Interpretation: The risk for Trichinella infection associated with commercial pork has decreased substantially in the United States since the 1940s, when data collection on trichinellosis cases first began. However, the continued identification of cases related to both pork and nonpork sources indicates that public education about trichinellosis and the dangers of consuming raw or undercooked meat still is needed.
Public Health Actions: Changes in domestic pork production and public health education regarding the safe preparation of pork have contributed to the reduction in the incidence of trichinellosis in the United States; however, consumption of wild game meat such as bear continues to be an important source of infection. Hunters and consumers of wild game meat should be educated about the risk associated with consumption of raw or undercooked meat.
Introduction
Trichinellosis is a foodborne parasitic zoonotic disease caused by roundworms of the genus Trichinella. Trichinellosis is a public health hazard and represents a food safety problem (1). Humans acquire the disease by consuming raw or undercooked meat that contains viable Trichinella larvae. Trichinella infection has been detected in domestic and wild animals from all continents except Antarctica (2).
Trichinella infection in human hosts can be divided into an intestinal (enteral) phase and a muscular (parenteral) phase, with clinical manifestations ranging from asymptomatic infection to fatal disease, depending on the number of larvae ingested (3). After ingestion, larvae are released into the intestinal mucosa and subsequently migrate to the blood vessels, from which they spread throughout the body before reaching the skeletal muscles (1). During the enteral phase, infection with low intensity (<70 larvae) can remain asymptomatic, but infection with approximately 70–150 or more larvae can cause gastroenteritis with diarrhea and abdominal pain approximately 2 days after infection (1,4). The parenteral phase is characterized by fever, myalgia, periorbital edema, eosinophilia, and increased levels of muscle enzymes (5,6). Death generally is ascribed to myocarditis, meningoencephalitis, or pneumonitis (7). Fatal complications such as respiratory failure caused by parasitism of the respiratory muscles have been reported (8–10).Treatment during the early stages of infection might be effective in preventing the development of more severe symptoms, although early clinical diagnosis of trichinellosis is difficult because symptoms often are lacking or nonspecific (11). Diagnosis of trichinellosis is made on the basis of a positive result from serologic testing for Trichinella-specific antibody or a Trichinella-positive muscle biopsy specimen in a patient exhibiting one or more clinical signs or symptoms compatible with trichinellosis (e.g., eosinophilia, fever, myalgia, or periorbital edema) (12). However, both serologic testing and biopsy examination can have limited sensitivity in early infections (6,11). Antibody to Trichinella can persist for years; positive serologic testing results can result in misdiagnoses in patients who have symptoms that are compatible with trichinellosis but whose current illness is attributable to other causes. For certain reported trichinellosis cases, disease might be attributed to recently consumed meat products rather than to the true source of past infection (13). Albendazole is the recommended drug for the treatment of the enteral phase of infection; albendazole often is used in conjunction with steroids to treat severe symptoms during the parenteral phase (1).
During 1947–1951, when systematic tracking of trichinellosis cases began in the United States, approximately 400 cases with 10–15 trichinellosis-related deaths were reported each year (14). This number declined to a median annual incidence of eight cases (range: 5–15) during 2002–2007, with no reported deaths (13). Historically, 60%–88% of infections in the United States were the result of ingesting raw or undercooked Trichinella-infected pork (15–18). However, measures taken by the U.S. pork industry many decades ago to improve the health of farm-raised hogs have made Trichinella infections in U.S. swine rare (19). The consumption of meat from Trichinella-infected wildlife, including wild boar, are now implicated in a greater proportion of cases (12,13).
This report presents data on trichinellosis cases in the United States reported to CDC from state and local health departments through the National Notifiable Disease Surveillance System (NNDSS, available at http://wwwn.cdc.gov/nndss) during 2008–2012. This report on the number of confirmed trichinellosis cases and the epidemiology of the disease is intended for public health officials, health-care providers, the pork industry, and the general public to promote awareness and prevention efforts in United States.
Methods
To quantify the number of confirmed trichinellosis cases and identify changes in the epidemiology of the disease to guide prevention efforts in United States, CDC analyzed 2008–2012 data from NNDSS. Annual incidence and mean annual incidence of confirmed trichinellosis cases were calculated for each reporting state. Variables analyzed included age, sex, race/ethnicity, month of illness onset, and source of infection (i.e., pork and nonpork products or unknown). Outbreaks of trichinellosis were characterized by year, state, number of cases, month of illness onset, and implicated food.
State health departments notify CDC of trichinellosis cases through NNDSS. Additional clinical and epidemiologic information is provided to CDC on a case report form (CDC form no. 54.7, available at http://www.cdc.gov/parasites/trichinellosis/resources/pdf/trichinellosis_case_report_form.pdf). State and local health department epidemiologists interview patients to obtain food exposure histories and clinical information. Additional cases might be identified separately from NNDSS through CDC laboratory testing for Trichinella. CDC notifies the state health department of laboratory-confirmed Trichinella infections, which are investigated subsequently to determine whether they meet the confirmed case definition.
A confirmed case of trichinellosis was classified using the 1996 CSTE case definition (20). A confirmed case was defined as an illness with clinically compatible symptoms of trichinellosis and laboratory-confirmed Trichinella infection. Signs and symptoms of trichinellosis include eosinophilia, fever, periorbital edema, and myalgia. Laboratory confirmation was made either by a positive result from serologic testing for Trichinella-specific antibody or by identification of Trichinella larvae in tissue obtained by muscle biopsy.
An outbreak of trichinellosis was defined as two or more cases, at least one of which was laboratory confirmed (20). In an outbreak setting, cases were reported as confirmed if they occurred in persons who shared an epidemiologically implicated meal (a meal that was consumed by a person who developed a clinically compatible illness that was laboratory confirmed) or ate an epidemiologically implicated meat product (a meat product that was consumed by a person who developed a clinically compatible illness that was laboratory confirmed) and had either a positive result on serologic testing for Trichinella-specific antibody or clinically compatible illness.
Cases that did not meet the definition of a confirmed case or those for which a case report form was not submitted were excluded from this report. Commercial pork products were defined as pork purchased at supermarkets, butcher shops, or restaurants. Noncommercial pork products were defined as pork obtained directly from a farm, home-raised swine, or wild boar.
The annual incidence of trichinellosis in each state was determined by dividing the number of reported cases by the U. S. Census Bureau estimate of the state population on July 1 of the year in which the cases were reported. The mean annual incidence of trichinellosis for each state was determined by calculating the average annual incidence in each state during 2008–2012.
Results
During 2008–2012, a total of 90 cases of trichinellosis, including five outbreaks, were reported to CDC from 24 states and the District of Columbia. Of these 90 cases, six (7%) were excluded from analysis, including one that did not meet the case definition and five for which case report forms were not available. This report provides data on the 84 cases from 23 states and the District of Columbia that met the case definition and for which case report forms were available.
The largest number of confirmed cases, 41 (49%) cases, occurred in the Pacific region* of the United States, including 35 cases in California and six cases in Alaska (Table 1). California accounted for 42% of the 84 cases (Table 1). The mean annual incidence of trichinellosis in Alaska (4.1 cases per 1 million population) was approximately 40 times higher than the mean annual incidence in the U.S. population (0.1 cases per 1 million population) (Table 1).
Of the 84 cases, 57 (68%) occurred among males and 27 (32%) among females. The median age of patients was 40 years (range: 1–72 years). The age distribution was similar among male and female patients, with 81% of the cases occurring in persons aged 20–69 years (Figure 1). Thirty-seven (44%) cases occurred in persons of Asian descent, 31 (37%) in whites, and two (2%) in blacks; information on race was unavailable for 14 (17%) cases (Table 2). Information on ethnicity was not available for most patients, but among the 37 persons for whom such information was available, 32 (86%) were non-Hispanic (Table 2).
A total of 77 (92%) patients had at least one classic sign or symptom of trichinellosis: 65 (77%) had myalgia, 45 (54%) had eosinophilia, 45 (54%) had fever, and 35 (42%) had periorbital edema. Sixty-nine (82%) patients recovered from the disease, and 15 (18%) had no information on outcome. No deaths from trichinellosis were reported. Of the 84 patients, 77 (92%) were tested, and 65 (84%) were seropositive for Trichinella antibodies. Muscle biopsies were performed for four (5%) patients, and three were positive for Trichinella larvae. Seven (8%) of the 84 patients who shared an epidemiologically implicated meal or ate an epidemiologically implicated meat product were not tested for Trichinella.
The confirmed or suspected source of infection was available for 67 (80%) cases. Of those patients for whom the source of infection was suspected or known, 22 (33%) patients attributed their illnesses to pork products, and 45 (67%) patients attributed their illnesses to nonpork products (Table 3). Among the 22 patients reporting consumption of pork products, 10 (45%) obtained meat from a commercial source (six from supermarkets, two from butcher shops, and two from restaurants), six (27%) consumed wild boar (from hunting), one (5%) consumed home-raised swine, and five (23%) consumed an unspecified pork product from an unknown source. Information on the manner in which the pork meat was cooked was available for 39 cases; 21 (54%) of the 39 patients reported eating raw or undercooked meat. Among the 45 patients reporting consumption of nonpork products, 41 (91%) consumed bear meat, two (4%) consumed deer meat, and two (4%) consumed ground beef (Table 3). Information on the manner in which the nonpork product was cooked was available for 12 cases. Three (25%) of the 12 patients reported eating raw or undercooked meat.
During 2008–2012, five outbreaks were reported from four states (Alaska, California, Illinois, and Minnesota), involving 40 persons (Table 4). Bear meat was implicated in three of the five outbreaks. One large outbreak, which accounted for 28 cases reported during the surveillance period, occurred in northern California in October 2008 following a community gathering at which raw or undercooked black bear meat was served (Table 4). The bear had been hunted legally a few days before the gathering and was reportedly lying down and appeared sick when it was shot (21). The bear was butchered on a table that was used later to serve food, and subsequent cross-contamination might explain why one person who reportedly did not consume any bear meat later became ill with symptoms consistent with trichinellosis (21). A second outbreak that occurred in northern California during October–November 2008 involved five persons who consumed raw or undercooked bear meat. An outbreak in Minnesota during March–April 2011 involving a man aged 50 years and his son aged 10 years was associated with the consumption of wild boar obtained from a wild game farm in Iowa in March 2011. An outbreak in October 2012 involving two persons, a Minnesota resident and an Illinois resident, was associated with consumption of pan-seared black bear meat during a hunting trip in Alaska that occurred in September 2012. An outbreak in Alaska in August 2012 involving a family of three persons could not be linked to a single meat source because the family reported consuming multiple types of undercooked meat during the exposure period.
Historically, seasonal patterns of cases in the United States have been observed in winter months (December–March) (15,22). During 2008–2012, no winter pattern was observed for 70 patients with known dates of illness onset (Figure 2). Twelve cases occurred in the winter, eight in the spring, and 41 in the fall. Most cases (87%) in October and November were associated with the outbreaks associated with bear meat consumption in California (Figure 2). For 45 patients who consumed nonpork products, most had illness onset during October–November, and illness was associated with bear meat (Figure 3).
Discussion
During 2008–2012, a median of 15 cases were reported annually to CDC, an increase from eight cases reported annually during 2002–2007 (13). The increase in cases during 2008–2012 was attributable in part to the October 2008 outbreak in California, which accounted for 28 (33%) of the reported cases. Of the 84 cases for which sufficient data were reported during the surveillance period, 22 (26%) were associated with pork products, an increase from 10 (19%) cases associated with pork products during 2002–2007 (13). Of the 22 cases associated with pork products, 10 (45%) were associated with commercial pork products, a decrease from five (50%) cases associated with commercial pork products during 2002–2007 (13). In addition, 45 (54%) of the 84 cases that occurred during 2008–2012 were associated with nonpork products; (41/84 [49%] bear meat), an increase from 27 (50%) of 54 cases during 2002–2007 (21/54 [39%] bear meat) (13). Most of the cases associated with nonpork products during 2008–2012 were the result of an outbreak that occurred in California in October 2008 involving consumption of raw or undercooked black bear meat. Among the 51 patients for whom information was available regarding the manner in which the meat product was cooked, 24 (47%) reported eating raw or undercooked meat, an increase from five (17%) of 30 cases reported during 2002–2007 (13).
The number of reported trichinellosis cases has decreased since 1947 (Figure 4). The number of reported cases related to eating nonpork products surpassed cases associated with pork products starting in 1997 (Figure 5). During 2008–2012, the number of cases associated with eating nonpork products was more than twice (45 cases) as many as those associated with pork products (22 cases) (Table 3; Figure 5). The majority of nonpork-associated cases were linked with wildlife (specifically bear meat) consumption. Three of the five outbreaks that occurred during 2008–2012 were associated with consumption of bear meat. Because the consumption of Trichinella-infected meat by an animal host is required for transmission of infection, herbivores such as deer are atypical Trichinella hosts (13). However, experiments have demonstrated that deer can become infected with Trichinella (23,24), and during 2008–2012, two patients reported consumption of deer meat during their exposure period.
The number of swine reared in organic livestock operations certified by the U.S. Department of Agriculture (USDA) increased from 482 in 1997 to 12,373 in 2011 (25). Swine reared by these methods are likely exposed to sylvatic (i.e., occurring in or affecting wild animals) and synanthropic (i.e., ecologically associated with humans) hosts of Trichinella and are therefore more likely to be infected with Trichinella than commercial pork raised in confinement buildings under biosecure conditions (26). In addition, improper implementation of measures that limit contact between domestic animals and wildlife might cause introduction of Trichinella infection from the sylvatic environment into domestic animals (1). To help decrease the probability of transmission to other wildlife, hunters should be educated to avoid leaving animal carcasses in the field (1).
The decline in incidence of trichinellosis is a result of decreased prevalence of Trichinella in commercial pork products. This is a consequence of government legislation and changes in the U.S. pork industry that have reduced exposure of domestic pigs to Trichinella (19) including implementation of the 1980 Federal Swine Health Protection Act, which prohibited feeding of potentially Trichinella-contaminated garbage to swine.† Changes to commercial production practices ensuring that swine are raised in biosecure confinement housing with adequate feed as well as feed storage facilities and equipment that control rodents, have contributed to the decline in incidence of trichinellosis (12). In addition, processing methods such as cooking and freezing have contributed to the decline in trichinellosis associated with pork products (12). USDA has stipulated specific cooking temperature and times, freezing temperatures and times, and curing methods for processed pork products to inactivate Trichinella larvae in meat (27).
The decline in the number of cases also might be attributed to USDA successfully educating consumers to fully cook fresh pork to temperatures high enough to inactivate Trichinella. USDA recommends that consumers of fresh ground pork and wild game cook the meat product to an internal temperature of 160°F (71°C) (28). Whole cuts of meat (excluding poultry and wild game) should be cooked to at least 145°F (63°C) then allowed to rest for 3 minutes before consuming (28). Sufficient freezing of Trichinella-infected meat will kill the encysted larvae of several Trichinella species (13). Pork <6 inches thick can be made safe if frozen to -20°F (-29°C) for 6 days, -10°F (-23°C) for 10 days, or 5°F (-15°C) for 20 days to kill any encysted larvae.§ However, freezing at these temperatures does not reliably kill the freeze-resistance species T. nativa and Trichinella T6, which are found in animals in the arctic and subarctic regions. Infective Trichinella larvae have been found in bear meat frozen at -4°F–20°F (-20°C– -6.5°C) for 27 months (29). In addition, meat handlers should follow good hygienic practices such as washing their hands with warm water and soap after handling raw meat and cleaning meat grinders thoroughly after use. Heating in microwave ovens, curing, drying, and smoking are not effective in inactivating Trichinella larvae (1).
Limitations
The findings in this report are subject to at least two limitations. First, national surveillance for trichinellosis is based on NNDSS, which is a passive surveillance system. For this reason, case ascertainment might be incomplete, and the actual burden of trichinellosis in the United States might be greater than the surveillance data provided in this report indicate. Second, many of the food exposure histories that are reported cannot be corroborated by laboratory or epidemiologic evidence and might represent only a best guess of what might have made the case-patients ill. This is particularly relevant to the "atypical" reported exposures to meat from herbivorous animals (mostly deer and cows). Nevertheless, surveillance for trichinellosis is useful in providing estimates of the burden of illness and in identifying changes in the epidemiology of trichinellosis in United States.
Conclusion
Although the incidence of trichinellosis has decreased substantially since 1947, the continued identification of trichinellosis cases related to commercial pork consumption, infections from sylvatic sources such as bear meat, and the reported histories of consumption of raw or undercooked meat indicate the continuing need for public education about trichinellosis. Persons receiving permits to hunt bear, wild boar, or other potential Trichinella hosts should be informed about the risk for trichinellosis and receive instruction regarding proper food safety practices. Consumers of pork and game meat should follow the recommended cooking and freezing methods to inactivate Trichinella larvae and follow good hygienic practices with raw meat. In addition, the public should receive ongoing education about prevention methods, with additional communication efforts during an outbreak.
References
- Gottstein B, Pozio E, Nockler K. Epidemiology, diagnosis, treatment, and control of trichinellosis. Clin Microbiol Rev 2009;22:127–45.
- Pozio E, Darwin Murrell K. Systematics and epidemiology of Trichinella. Adv Parasitol 2006;63:367–439.
- Hueffer K, Parkinson AJ, Gerlach R, Berner J. Zoonotic infections in Alaska: disease prevalence, potential impact of climate change and recommended actions for earlier disease detection, research, prevention and control. Int J Circumpolar Health 2013;72.
- Murrell KD, Bruschi F. Clinical trichinellosis. In: Progress in clinical parasitology. Tsieh S (ed). Boca Raton, FL: CRC Press; 1994:117–50.
- Clausen MR, Meyer CN, Krantz T, et al. Trichinella infection and clinical disease. QJM 1996;89:631–6.
- Watt G, Silachamroon U. Areas of uncertainty in the management of human trichinellosis: a clinical perspective. Expert Rev Anti Infect Ther 2004;2:649–52.
- Pozio E, Gomez Morales MA, Dupouy-Camet J. Clinical aspects, diagnosis and treatment of trichinellosis. Expert Rev Anti Infect Ther 2003;1:471–82.
- Brashear RE, Martin RR, Glover JL. Trichinosis and respiratory failure. Am Rev Respir Dis 1971;104:245–8.
- Compton SJ, Celum CL, Lee C, et al. Trichinosis with ventilatory failure and persistent myocarditis. Clin Infect Dis 1993;16:500–4.
- Watt G, Saisorn S, Jongsakul K, Sakolvaree Y, Chaicumpa W. Blinded, placebo-controlled trial of antiparasitic drugs for trichinosis myositis. J Infect Dis 2000;182:371–4.
- Dupouy-Camet J, Kociecka W, Bruschi F, Bolas-Fernandez F, Pozio E. Opinion on the diagnosis and treatment of human trichinellosis. Expert Opin Pharmacother 2002;3:1117–30.
- Roy SL, Lopez AS, Schantz PM. Trichinellosis surveillance—United States, 1997–2001. MMWR Surveill Summ 2003;52(No. SS-6).
- Kennedy ED, Hall RL, Montgomery SP, Pyburn DG, Jones JL. Trichinellosis surveillance—United States, 2002–2007. MMWR Surveill Summ 2009;58(No. SS-9).
- Schantz PM. Trichinellosis in the United States—1947–1981. Food Technol 1983;37:83-6.
- Bailey TM, Schantz PM. Trichinosis surveillance, United States, 1986. MMWR Surveill Summ 1988;37(No. SS-5):1–8.
- Gamble HR, Bush E. Seroprevalence of Trichinella infection in domestic swine based on the National Animal Health Monitoring System's 1990 and 1995 swine surveys. Vet Parasitol 1999;80:303–10.
- McAuley JB, Michelson MK, Schantz PM. Trichinosis surveillance, United States, 1987–1990. MMWR Surveill Summ 1991;40(No. SS-3).
- Stehr-Green JK, Schantz PM, Chisolm EM. Trichinosis surveillance, 1984. MMWR Surveill Summ 1986;35(No. SS-2):11–15.
- Zimmermann WJ, ed. The current status of trichinellosis in the United States. Third International Conference on Trichinellosis. New York, NY: Intext Educational Publishers; 1975.
- CDC. Trichinellosis (Trichinosis) (Trichinella spp.) 1996 case definition. Atlanta, GA: US Department of Health and Human Services, CDC; 2014.
- Hall RL, Lindsay A, Hammond C, et al. Outbreak of human trichinellosis in Northern California caused by Trichinella murrelli. Am J Trop Med Hyg 2012;87:297–302.
- Bailey TM, Schantz PM. Trends in the incidence and transmission patterns of trichinosis in humans in the United States: comparisons of the periods 1975–1981 and 1982–1986. Rev Infect Dis 1990;12:5–11.
- Moretti A, Piergili-Fioretti D, Grelloni V, Antognoni MT, Leonardi L, Tacconi G. Experimental trichinellosis in fallow-deer (Dama dama L.). Parasite 2001;8(Suppl):S200–2.
- Oksanen A, Oivanen L, Eloranta E, Tirkkonen T, Asbakk K. Experimental trichinellosis in reindeer. J Parasitol 2000;86:763–7.
- US Department of Agriculture. Economic Research Service. Organic production. Washington, DC: US Department of Agriculture; 2013. Available at http://ers.usda.gov/Data-products/organic-production.aspx.
- Ribicich M, Gamble HR, Bolpe J, et al. Evaluation of the risk of transmission of Trichinella in pork production systems in Argentina. Vet Parasitol 2009;159:350–3.
- Gamble HR. Parasites associated with pork and pork products. Rev Sci Tech 1997;16:496–506.
- US Department of Agriculture. Safe minimum internal temperature chart. In: US Department of Agriculture. Food safety information. Washington, DC: US Department of Agriculture; 2012.
- Worley DE, Seesee FM, Espinosa RH, Sterner MC. Survival of sylvatic Trichinella spiralis isolates in frozen tissue and processed meat products. J Am Vet Med Assoc 1986;189:1047–9.
* According to the NNDSS geographic classification, the Pacific region includes Alaska, California, Hawaii, Oregon, and Washington.
† Federal Swine Health Protection Act (Public Law 96-468) of October 17, 1980.
§ Code of Federal Regulations. Prescribed treatment of pork and products containing pork to destroy trichinae, 9 C.F.R., Sect. 318.10 (2014).
FIGURE 1. Age distribution of persons with confirmed cases of trichinellosis,* by sex — National Notifiable Disease Surveillance System, United States, 2008–2012
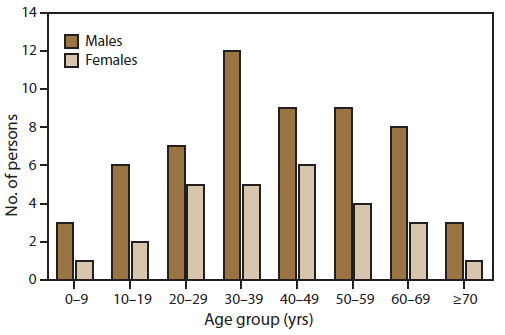
* N = 84.
Alternate Text: The figure shows the age distribution, by sex, of 84 persons in the United States with confirmed cases of trichinellosis using data from the National Notifiable Disease Surveillance System for 2008-2012. The age group with the highest number of ill persons was age 30-39 years. Men were more likely than women to have become ill across all age groups.
FIGURE 2. Number* of persons with confirmed cases of trichinellosis, by month of illness onset — National Notifiable Disease Surveillance System, United States, 2008–2012
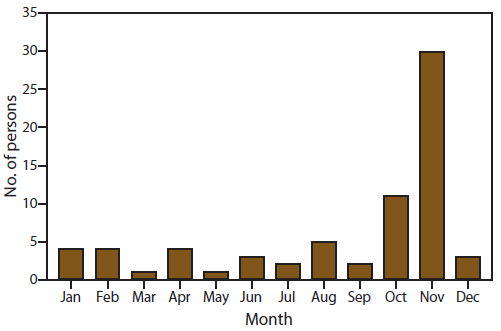
* N = 70. Of the 30 of cases in November, 26 (87%) were linked to an outbreak in California associated with bear meat.
Alternate Text: The figure shows the number of persons in the United States, by month of illness onset, with confirmed cases of trichinellosis using data from the National Notifiable Disease Surveillance System for 2008-2012. Of the 70 cases reported, the highest number (30) occurred in November, of which 26 were linked to an outbreak in California associated with bear meat.
FIGURE 3. Number* of persons with confirmed cases of trichinellosis associated with eating nonpork products, by month of illness onset — National Notifiable Disease Surveillance System, United States, 2008–2012
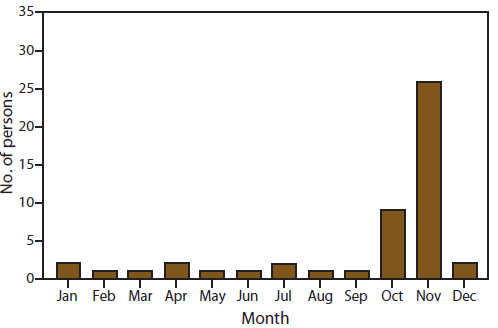
* N = 45. Of the 26 of cases in November, all were linked to an outbreak in California associated with bear meat.
Alternate Text: The figure shows the number of persons in the United States, by month of illness onset, with confirmed cases of trichinellosis associated with eating nonpork products using data from the National Notifiable Disease Surveillance System for 2008-2012. Of the 45 cases reported, 26 occurred in November and were linked to an outbreak in California associated with bear meat.
FIGURE 4. Number of reported confirmed cases of trichinellosis, by year — National Notifiable Disease Surveillance System, United States, 1947–2012
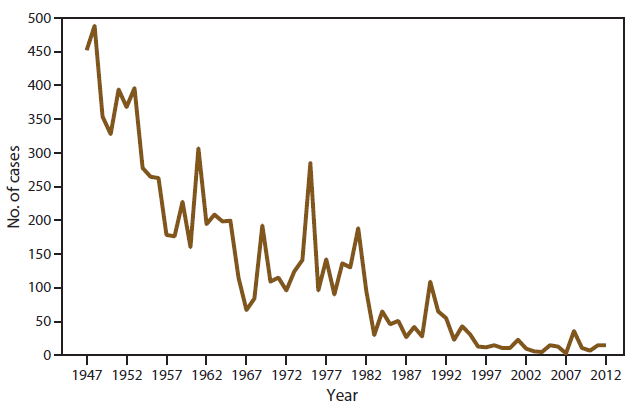
Alternate Text: The figure shows the number of reported confirmed cases of trichinellosis in the United States, by year, using data from the National Notifiable Disease Surveillance System, United States for 1947-2012. The number of cases has declined steadily during that time period.
FIGURE 5. Number of reported confirmed cases of trichinellosis, by source of infection as reported in surveillance summaries — National Notifiable Disease Surveillance System, United States, 1975–2012
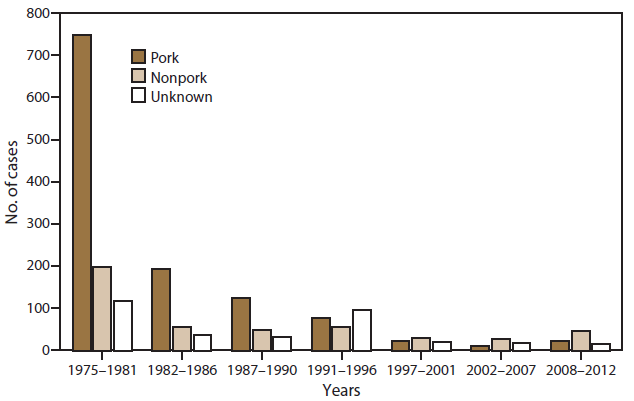
Alternate Text: The figure shows the number of reported confirmed cases of trichinellosis in the United States, by source of infection, using data from the National Notifiable Disease Surveillance System, United States for 1975-2012. During that time period, the number of cases declined steadily, and the number of cases associated with pork decreased substantially. Currently nonpork meat is more often a source of infection than pork.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
