FIGURE 1. Principal city of each metropolitan statistical area participating in the National HIV Behavioral Surveillance System: Men Who Have Sex With Men --- 21 U.S. Cities, 2008
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
HIV Risk, Prevention, and Testing Behaviors Among Men Who Have Sex With Men --- National HIV Behavioral Surveillance System, 21 U.S. Cities, United States, 2008
Corresponding author: Teresa Finlayson, PhD, Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC, 1600 Clifton Rd., NE, M.S. E-46, Atlanta, GA 30333. Telephone: 404-639-2083; Fax: 404-639-8640; E-mail: tfinlayson@cdc.gov.
Abstract
Problem/Condition: Approximately 1.1 million persons in the United States are living with human immunodeficiency virus (HIV) infection. More than half of those infected are men who have sex with men (MSM).
Reporting Period: June--December 2008.
Description of System: The National HIV Behavioral Surveillance (NHBS) System collects risk behavior data from three populations at high risk for HIV infection: MSM, injection-drug users, and heterosexual adults at increased risk for HIV infection. Data for NHBS are collected in rotating cycles. NHBS participants must be aged ≥18 years, live in a participating metropolitan statistical area, and be able to complete a behavioral survey in English or Spanish. Men who reported being infected with HIV or who had no male sex partners during the past 12 months were excluded from this analysis.
Results: This report summarizes data gathered from 8,175 MSM during the second data collection cycle of NHBS. In addition to having at least one male sex partner, 14% of participants had at least one female sex partner during the past 12 months. Unprotected anal intercourse with a male partner was reported by 54% of the participants; 37% reported having unprotected anal sex with a main male partner (someone with whom the participant had sex and to whom he felt most committed, such as a boyfriend, spouse, significant other, or life partner), and 25% reported having unprotected anal sex with a casual male partner (someone with whom the participant had sex but with whom he did not feel committed, did not know very well, or had sex with in exchange for something such as money or drugs). Noninjection drug use during the past 12 months was reported by 46% of participants. Specifically, 38% used marijuana, 18% cocaine, 13% poppers (amyl nitrate), and 11% ecstasy. Two percent of the participants reported injecting drugs for nonmedical purposes in the past 12 months. Of the participants surveyed, 90% had been tested for HIV during their lifetime, 62% had been tested during the past 12 months, 51% had received a hepatitis vaccination, 35% had been tested for syphilis during the past 12 months, and 18% had participated in an individual- or group-level HIV behavioral intervention.
Interpretation: MSM in the United States continue to engage in sexual and drug-use behaviors that increase the risk for HIV infection. Although many MSM had been tested for HIV infection, many had not received hepatitis vaccinations or syphilis testing, and only a small proportion had recently participated in a behavioral intervention.
Public Health Action: To reduce HIV infection among MSM, additional effort is needed to decrease the number of men who are engaging in risk behaviors while increasing the number who recently have been tested for HIV. The National HIV/AIDS Strategy for the United States delineates a coordinated response to reduce infections and HIV-related health disparities among MSM and other disproportionately affected groups. NHBS data can be used to monitor progress toward the goals of the national strategy and to guide national and local planning efforts to maximize the impact of HIV prevention programs.
Introduction
At the end of 2006, more than 1.1 million people in the United States were living with human immunodeficiency virus (HIV) infection (1) and an estimated 56,000 people were infected annually (2). Among new HIV infections in 2006, approximately 53% were men who have sex with men (MSM), 31% were infected through heterosexual contact, 12% were injection-drug users (IDU), and 4% were both MSM and IDU (2). The number of persons living with HIV infection, particularly among groups at increased risk for infection, will likely continue to increase without a substantially improved and coordinated response to HIV in the United States (3). The National HIV/AIDS Strategy for the United States, released in July 2010, addresses the urgent need to reduce HIV incidence, improve access to care and health outcomes for people living with HIV, reduce HIV-related disparities and health inequities, and improve coordination of HIV programs across federal, state, territorial, tribal, and local governments (3).
The primary objective of the National HIV/AIDS Strategy is to lower the annual number of new infections by 25% in 5 years. This objective can be achieved by implementing three critical steps to reduce HIV infections: intensifying HIV prevention efforts in communities where HIV is most heavily concentrated (including MSM, blacks, Hispanics/Latinos, and substance users); expanding efforts to prevent HIV infection by using a combination of effective, evidence-based approaches; and educating the general public about the threat of HIV and how to prevent it. State and local health departments as well as federal agencies are expected to monitor progress toward the goals of the National HIV/AIDS Strategy.
The National HIV Behavioral Surveillance (NHBS) System was designed to help state and local health departments in areas with high AIDS prevalence monitor selected risk behaviors, HIV testing experiences, use of prevention programs, and HIV prevalence in three populations at high risk for HIV infection: MSM, injection-drug users, and heterosexual adults at increased risk (4). NHBS is the primary source of data for monitoring behaviors among populations at risk for HIV infection in the United States. The behavioral data collected through NHBS along with seroprevalence data help characterize the epidemic among these populations. Findings from NHBS enhance the understanding of HIV risk and testing behaviors and identify gaps in prevention efforts. NHBS data are used at the state and local levels to renew and maintain efforts to prevent HIV infection as well as other bloodborne and sexually transmitted diseases (STDs). Thus, NHBS serves as a key component of CDC's comprehensive approach to reducing the spread of HIV in the United States. Data from this system also will be used to monitor efforts toward achieving the National HIV/AIDS Strategy's goal of reducing HIV incidence in these populations. This report summarizes results from the second NHBS data collection cycle among MSM, which was conducted during June--December 2008. Data from the first cycle among MSM (2004--2005) were reported previously (5). This report provides descriptive data from the second cycle that can be used to monitor the percentages of men reporting specific risk behaviors, HIV testing, and participation in prevention programs. Monitoring these data is useful for assessing the proportion of MSM who engage in risk behaviors and for identifying HIV prevention opportunities in this population. HIV prevalence data from the second cycle were reported previously (6).
Methods
NHBS data are collected in annual cycles from one risk group per year so that each group is surveyed once every 3 years. A period of data collection with each specific population is referred to as a cycle, and the cycles for each population are numbered consecutively. NHBS does not collect participant names or any other identifying information other than birth date and zip code. The same basic eligibility criteria are used in each cycle: age ≥18 years, current residence in the metropolitan statistical area (MSA) or specified MSA division, no previous participation in NHBS during the current survey cycle, ability to complete the survey in either English or Spanish, and ability to provide informed consent. In addition to these basic eligibility criteria, participation in the MSM cycle is limited to persons who reported assignment of male sex at birth and self-identified as male.
For each survey cycle, a standardized questionnaire is used to collect information about behavioral risks for HIV infection, HIV testing, and use of HIV prevention services. The in-person survey is administered by a trained interviewer using a handheld computer. Each participating area attempts to interview 450--500 eligible persons, depending on the survey cycle. All participants are offered an anonymous HIV test, which is linked to the survey data though a unique survey identifier.
Participating Areas
State and local health departments that were eligible to participate in NHBS were those whose jurisdictions included an MSA or a specified MSA division where AIDS prevalence in 2006 was ranked among the highest. The first cycle of NHBS among MSM was conducted in 15 MSAs. The second cycle of the NHBS among MSM was conducted in the following 21 MSAs; if a metropolitan division is indicated, the survey was conducted within that specific division of the MSA: Atlanta-Sandy Springs-Marietta, Georgia; Baltimore-Towson, Maryland; Boston-Cambridge-Quincy, Massachusetts-New Hampshire: Boston-Quincy Division; Chicago-Joliet-Naperville, Illinois-Indiana-Wisconsin: Chicago-Joliet-Naperville Division; Dallas-Fort Worth-Arlington, Texas: Dallas-Plano-Irving Division; Denver-Aurora-Broomfield, Colorado; Detroit-Warren-Livonia, Michigan: Detroit- Livonia-Dearborn Division; Houston-Sugar Land-Baytown, Texas; Los Angeles-Long Beach-Santa Ana, California: Los Angeles-Long Beach-Glendale Division; Miami-Ft Lauderdale-Pompano Beach, Florida: Miami Division; New Orleans-Metairie-Kenner, Louisiana; New York-Northern New Jersey-Long Island, New York-New Jersey-Pennsylvania: New York-White Plains-Wayne Division; New York-Northern New Jersey-Long Island, New York-New Jersey-Pennsylvania: Nassau-Suffolk Division; New York-Northern New Jersey-Long Island, New York-New Jersey-Pennsylvania: Newark-Union Division; Philadelphia-Camden-Wilmington, Pennsylvania, New Jersey, Delaware, Maryland: Philadelphia Division; San Diego-Carlsbad-San Marcos, California; San Francisco-Oakland-Fremont, California: San Francisco-San Mateo-Redwood City Division; San Juan-Caguas-Guaynabo, Puerto Rico; Seattle-Tacoma-Bellevue, Washington: Seattle-Bellevue-Everett Division; St. Louis, Missouri-Illinois; and Washington-Arlington-Alexandria, District of Columbia (DC)-Virginia-Maryland-West Virginia; Washington-Arlington-Alexandria Division. These metropolitan areas represented approximately 60% of all AIDS cases in urban areas with a population size of at least 500,000 in 2008 (7). Throughout this report, MSAs are referred to by the name of the primary principal city (Figure 1).
Sampling Method
Participants for the survey were recruited through time-location sampling methods (8). The primary steps included identifying venues frequented by MSM, determining the best time for sampling at each venue and the sampling events to be conducted each month, and selection and recruitment of men.
Identification of Venues Frequented by MSM
In each city, a team of staff members familiar with the local community conducted formative research to establish a list of venues frequented by MSM (9). To identify possible venues for inclusion in the venue list, the team consulted local publications, online media, members of the local MSM community, business owners, staff members at community-based organizations, key health department staff members, and persons providing medical and social services to MSM. If a venue did not exclusively serve MSM, the team observed and conducted brief interviews at the venue. Brief interviews were used to assess the eligibility of male patrons for NHBS and their sexual history with other men. If the information from these brief interviews indicated that the venue would yield a sufficient number of MSM (i.e., ≥75% of men approached would meet the eligibility criteria and reported sex with other men), the venue was included on the venue list. Clinics and other health-care settings were specifically excluded because of the potential for introducing bias in several key indicators (e.g., HIV testing history and access to health care). Venues on the list were categorized as a bar, dance club, fitness club or gymnasium, Gay Pride event, park or beach, large dance party (e.g., rave or circuit party), café or restaurant, retail business, sex establishment or sex environment, social organization, street location, or another venue type, such as an event hosted by the local house ball community.*
Determination of the Best Time for Sampling at Each Venue
After the venues frequented by MSM were identified, the team determined the best days of the week and the best times (typically 4-hour periods) at each venue to interview safely a sufficient number of eligible men. Days and times for each venue were placed on a list that was later used to determine sampling events for each month. This venue list became the sampling frame.
Determination of the Sampling Events for a Given Month
On average, 14 sampling events were conducted in each MSA every month. A sampling event consisted of a single visit to a venue during one day and time specified for that venue. From the sampling frame, the team would first randomly select 14 venues without replacement. Then for each of the 14 venues, the team would randomly select a day and time period. These sampling periods were scheduled on a calendar for the month so that the local team would know where to conduct sampling events.
Selection and Recruitment of Men at a Sampling Event
During each sampling event, a team of recruiters and interviewers visited the venue to enroll men in the study. After arrival, the team would establish boundaries (an area or a line) for recruiting potential participants. The established boundaries were unknown to potential participants. All men entering the defined area or crossing the defined line were approached sequentially for recruitment.
Data Collection
Men who were recruited were escorted to a private area for the interview. A brief interview was conducted to determine eligibility for NHBS; men who were deemed eligible were invited to participate. Men who accepted the invitation to participate were asked to provide informed consent for the interview. Men who consented to the interview were offered an anonymous HIV test as part of the survey. Trained interviewers conducted face-to-face interviews using handheld computers. Interviews took about 30 minutes to complete and consisted of questions about demographic characteristics, HIV testing history, sexual and drug use behaviors, hepatitis testing and vaccination, STD testing and diagnosis, and use of HIV prevention services and programs. Participants received $20--$30 in cash or as a gift certificate for participation; the specific amount was determined locally. For participants who consented to the anonymous HIV testing, local testing procedures were followed, and an additional incentive was provided. The results of HIV testing from this cycle have been reported elsewhere (6).
Data Analysis
Participants
This surveillance summary presents the results of a descriptive analysis of key behavioral surveillance indicators for MSM in the 21 MSAs or MSA divisions where data were collected during June--December 2008; no statistical tests were performed. In addition to the NHBS eligibility criteria, three criteria were applied for inclusion in this report. During the interview, participants must have reported 1) being male at birth, 2) having had oral or anal sex with at least one male partner during the 12 months before the interview, and 3) not being infected with HIV. Men who were aware that they were infected with HIV were excluded from this analysis to focus the summary on risk behaviors related to acquiring HIV infection and experiences with HIV prevention services. Data and the related percentages were suppressed for cells with fewer than five cases.
The data for participants were analyzed according to race/ethnicity, age group, education level, sexual identity, health insurance status, annual household income, and MSA. Responses for race/ethnicity were categorized into mutually exclusive categories: non-Hispanic white; non-Hispanic black; Hispanic or Latino; American Indian or Alaska Native; Asian, Native Hawaiian, or other Pacific Islander; and some other racial group, which included persons of multiple racial backgrounds. Persons of Hispanic or Latino ethnicity might be of any race. Education level was categorized as less than high school, high school diploma or equivalent (e.g., general educational development [GED] diploma), some college or technical degree, and college degree or postgraduate education. Health insurance was categorized as none, private only (e.g., health insurance obtained through a private insurance policy or employer, TRICARE, CHAMPUS, or membership in a health maintenance organization), public only (e.g., Medicare, Medicaid, or Veterans Administration coverage), or other coverage. Annual household income was collected from participants in ranges, which were combined into four categories: ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total number of men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. In addition, three time frames for self-reported behaviors or experiences were included in analyses: ever (i.e., at any point in the participant's lifetime), during the 12 months before the interview, and the most recent time the participant engaged in the behavior.
Sexual Behavior
The sexual behavior that carries the highest risk for HIV transmission between MSM is unprotected anal sex (12--16); sexual transmission of HIV has been associated with drug use and nondisclosure of HIV infection (14). Details about anal sex with male partners (in the 12 months before the interview and the most recent encounters) are presented as key risk behaviors for HIV transmission among MSM. Male sex partners were categorized as main or casual partners. A main partner was someone with whom the participant felt most committed (e.g., boyfriend, spouse, significant other, or life partner). A casual partner was someone with whom the participant did not feel committed, whom he did not know very well, or with whom he had sex in exchange for something such as money or drugs. Participants could report having more than one main or casual partner in the past 12 months. Participants who reported new main or casual male partners during the past 12 months were asked whether they had discussed their own and their partner's HIV infection status before having sex for the first time. Characteristics of the most recent sexual encounter with a male sex partner and the participant's relationship with that partner include unprotected anal sex (i.e., without a condom) and type of anal sex, either insertive (participant placed his penis in the anus of his sex partner) or receptive (participant's sex partner placed his penis in the participant's anus). Participants who reported being in a relationship with the most recent sexual partner for ≤3 years were asked where they met that partner.
Participants who reported both male and female sex partners, were asked about their sexual behaviors during the past 12 months with partners of both sexes. For female partners, data are presented for vaginal and anal sex. Unprotected vaginal sex was defined as having vaginal sex without a condom.
Alcohol and Drug Use
Participants were asked about their use, during the past 12 months, of multiple types of drugs (injection or noninjection) that had not been prescribed for them. All participants were asked whether they used an erectile dysfunction drug (i.e., a phosphodiesterase type 5 inhibitor such as sildenafil, vardenafil, or tadalafil) during the past 12 months. However, participants who reported methamphetamine use (injection or noninjection) during the past 12 months also were asked whether they had used methamphetamine in combination with an erectile dysfunction drug. Alcohol use was defined as drinking any alcohol such as beer, wine, malt liquor, or hard liquor. Both heavy drinking and binge drinking are reported; heavy drinking was defined as drinking, on average, more than two alcoholic beverages per day in the 30 days before the interview. Binge drinking was defined as drinking more than five alcoholic beverages at one sitting in the 30 days before the interview. Participants who reported using alcohol and drugs also were asked whether they had ever participated in a drug or alcohol treatment program.
Use of Prevention Services and Programs
HIV Testing
Ideally, HIV-infected persons who know their HIV infection status receive treatment and prevention services, which can reduce the likelihood that they will transmit HIV to others. Because sexually active MSM are at increased risk for HIV infection, CDC recommends they be tested for HIV infection at least annually (17). Data are presented on whether participants had an HIV test ever and during the 12 months before the interview. The facility administering the most recent HIV test and the reasons for not having been tested during the past 12 months are also presented. Participants were asked to select from a list of reasons for not having been tested during the past 12 months (e.g., thought at low risk for HIV infection, fear of finding out about HIV infection, and lack of time, money, or transportation).
Hepatitis Vaccination
Because MSM are at increased risk for infection with hepatitis A and hepatitis B virus, public health recommendations for sexually active MSM include both hepatitis A and B vaccinations (18,19). Hepatitis A vaccination was defined as having ever received at least 1 dose of hepatitis A vaccine. Hepatitis B vaccination was defined as having ever received at least 1 dose of hepatitis B vaccine.
STD Testing
MSM are at increased risk for acquiring STDs (20); moreover, STDs can increase the likelihood of acquiring HIV (21). Public health recommendations for sexually active MSM include testing at least annually for common STDs, including syphilis, gonorrhea, and chlamydia (22). More frequent STD testing (i.e., every 3--6 months) is recommended for MSM who have anonymous or multiple sex partners, have sex while using illegal drugs, including methamphetamine, or have sex partners who engage in these behaviors (22). The only STD testing data presented in this report are for syphilis because the questionnaire did not ask about testing for STDs other than syphilis and HIV. Participants were asked whether they had been tested for syphilis during the 12 months before the interview and whether they had been told during the past 12 months by a nurse, physician, or other health-care provider that they had an STD.
Behavioral Interventions
Behavioral interventions can substantially reduce sexual risk behaviors and thus the likelihood of acquiring HIV (23). Knowing the characteristics of persons who participated in behavioral interventions during the 12 months before the interview can be an indicator of whether these interventions are reaching the intended populations. Participants were asked about participation in individual- or group-level HIV-related behavioral interventions during the past 12 months. The definitions for both intervention levels were based on the intervention types in CDC's evaluation system (24). Conversations that took place solely as a part of obtaining HIV testing (e.g., pretest or posttest counseling) were not considered HIV behavioral interventions.
Results
In 2008, a total of 28,468 persons were approached for participation at 626 venues in 21 cities. Of the 12,474 who were screened for participation in NHBS, 11,074 (89%) were eligible for the survey interview. A total of 1,400 were not eligible: 1,138 lived outside the MSA, 45 were aged <18 years, 71 were previous participants, 91 did not identify themselves as male, and 83 were not able to provide their consent to the survey (e.g., men who were intoxicated or who did not speak either English or Spanish well); exclusion categories are not mutually exclusive. Of the 11,074 eligible men, 10,729 agreed to participate, and 10,678 completed the survey interview. For this report, 2,503 completed interviews from the following participants were excluded: 1,379 participants who had not had sex with another man during the 12 months before the interview, 1,206 who reported being infected with HIV, and 33 who provided potentially invalid responses; categories are not mutually exclusive. This report includes data from 8,175 completed interviews.
Characteristics of Participants
Participants were of diverse racial/ethnic backgrounds; however, the largest proportion was white (not Hispanic/Latino) (Table 1). Most (71%) of the men reported at least some college or technical school education, and most (80%) identified themselves as homosexual; a smaller percentage (19%) identified as bisexual. Approximately half (55%) reported having private health insurance, and 33% had no health insurance.
Although all venues in the sampling frame had an equal probability of being selected for sampling events, most were bars or dance clubs. Sixty-six percent of the men included in this summary were recruited from a bar or dance club. Each participating area, on average, had 389 interviews (range: 86--544) included in this analysis.
Sexual Behavior
Type of Partner
Of the 8,175 participants, 6,181 (76%) reported having more than one male sex partner during the 12 months before the interview. A total of 5,303 (65%) reported a main male sex partner (median: 1; intraquartile range: 1--2), and 5,868 (72%) reported having a casual male sex partner (median: 3; intraquartile range: 2--9). Overall, 2,997 (37%) reported having both types of partners.
Sexual Behavior with Male Partners
A total of 4,403 (54%) participants reported having unprotected anal sex with a male partner during the past 12 months. Of the 8,175 participants, 37% reported having unprotected anal sex with a main male partner, and 25% reported having unprotected anal sex with a casual male partner. Anal sex with main male partners was most common in younger age groups and among men who identified themselves as homosexual (Table 2). However, the percentages of men who had anal sex with casual male partners were similar among men in all categories of age and sexual identity. Although the percentages of men who reported anal sex and unprotected anal sex were relatively consistent in terms of race and ethnicity, unprotected anal sex with main male sex partners was least common among black participants. Unprotected anal sex with casual male partners was lower among men in the highest categories of education and income.
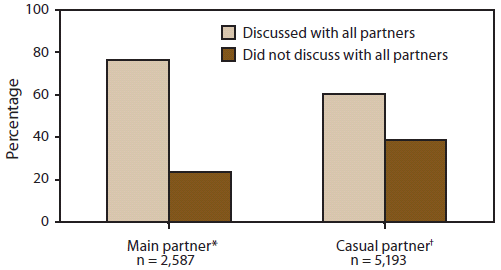
Of the 8,175 participants, 2,587 (32%) reported having new main male partners (median: 1, intraquartile range: 1--2), and 5,193 (64%) reported having new casual male partners (median: 3, intraquartile range: 2--8) during the past 12 months. A larger proportion of men had discussed the HIV infection status of themselves and their partners with all main partners than with all casual partners (Figure 2).
A total of 3,042 (37%) participants did not know the HIV infection status of their most recent male partner. This was more common for casual partners; 53% of men whose most recent partner was a casual partner did not know the status of that partner, compared with 19% of men whose most recent partner was a main partner. The percentages of men who had anal sex and unprotected anal sex during their most recent sexual encounter were higher with main than casual male partners (Table 3). More participants reported having insertive than receptive anal sex during their most recent sexual encounter. Unprotected insertive and receptive anal sex were reported by similar proportions of men whose most recent male sex partners were HIV-negative, HIV-positive, or of unknown HIV status. Overall, during their most recent sexual encounter, 12% of the men engaged in either unprotected insertive or receptive anal sex with an HIV-positive partner or partner of unknown HIV status. Of the 6,855 men who reported that the duration of the relationship with their most recent sex partner was ≤3 years, 2,699 (39%) had met the partner at a bar or club, and 1,392 (20%) had met the partner on the Internet or through a chat line.
Sexual Behavior with Male and Female Partners
Fourteen percent of the men surveyed (1,109) also reported having anal, vaginal, or oral sex with a female partner (Table 4). Of men who had sex with both male and female partners, 20% engaged only in oral sex with their male partners, and 4% engaged only in oral sex with their female partners. Of the participants who had sex with both male and female partners, more had unprotected vaginal or anal sex with their female partners (63%) than unprotected anal sex with their male partners (54%). However, among men who identified as homosexual, more had unprotected anal sex with male partners (65%) than unprotected vaginal or anal sex with female partners (54%). Unprotected vaginal or anal sex with female partners was reported by a higher percentage of participants with less than a high school education or an annual household income of <$20,000.
Alcohol and Drug Use
Injection Drug Use
Among the 8,175 participants, 436 (5%) had ever injected drugs for nonmedical purposes, and 188 (2%) had injected drugs during the past 12 months. Of those who had injected drugs during the past 12 months, 84 (45%) had injected methamphetamine and 59 (31%) reported high-risk injection practices such as sharing needles, syringes, or other drug-injection or preparation equipment. Most (61%) participants who had injected drugs during the past 12 months had participated in a drug or alcohol treatment program during their lifetime.
Noninjection Drug Use
During the past 12 months, 3,832 (47%) participants had used noninjection drugs that were not prescribed for them. Of the 8,175 participants, most had used marijuana (38%), followed by cocaine (18%), poppers (i.e., amyl nitrate; 13%), and ecstasy (11%) (Table 5). Noninjection methamphetamine use was less common (6%). Of the 3,832 participants who used noninjection drugs, 1,132 (30%) only used marijuana, and 749 (20%) had participated in a drug or alcohol treatment program during their lifetime.
More white than black participants reported noninjection use of cocaine and poppers during the past 12 months (Table 6). The use of poppers increased with educational attainment, whereas marijuana and methamphetamine use decreased with increasing educational attainment. More men who identified themselves as homosexual used poppers than did men who did not identify themselves as homosexual. The percentage of men who used marijuana was higher among men aged <30 years and lower among men who identified as homosexual.
Erectile Dysfunction Drugs and Methamphetamine
Of those surveyed, 982 (12%) had used an erectile dysfunction drug during the past 12 months; of those, 557 (57%) had taken the drug for a purpose other than the treatment of erectile dysfunction. Among the 556 participants who had used injection or noninjection methamphetamine during the past 12 months, 101 (18%) had used methamphetamine in combination with an erectile dysfunction drug.
Alcohol Use
Most (84%) participants had consumed an alcoholic beverage during the past 30 days (i.e., were current drinkers) (Table 7). The percentage of current drinkers increased with education and income. Seventeen percent reported heavy drinking, and 57% reported binge drinking during the 30 days before the interview. The percentages of men who reported heavy alcohol use was highest among whites (20%) and Hispanics/Latinos (18%), men who did not identify as homosexual (22%), and men with less than a high school education (24%). Binge drinking increased with income and education. The percentage of men reporting binge drinking was highest among those who were aged 25-- 29 years (56%), identified as homosexual (49%), and had completed at least some college (50%) or attained a college degree or postgraduate education (49%).
Use of Prevention Services and Programs
HIV Testing
Almost all participants (90%) had been tested for HIV infection during their lifetime, and many (62%) had been tested during the past 12 months (Table 8). Although a high percentage of participants had been tested, the percentages of men who had been tested within the past 12 months increased with education and were higher among men aged <40 years and those who identified as homosexual. Men who had been tested during the past 12 months were tested in the offices of private physicians (26%), HIV counseling and testing programs (23%), and public health clinics or community health centers (19%) (Table 9).
A total of 3,068 (38%) participants had not been tested during the past 12 months. The most frequently reported main reason for not having an HIV test during the past 12 months was that the participant thought he was at low risk for HIV infection (42%), followed by fear of testing positive (24%) (Table 10). Although men reported structural barriers to HIV testing (e.g., lack of transportation, money, or health insurance), these were not frequently reported reasons (i.e., ≤3% of men reported these as the main reason) for not being tested during the past 12 months.
Hepatitis Vaccination
About one half of the participants (51%) reported ever receiving at least one dose of either hepatitis A or hepatitis B vaccine. A somewhat greater percentage of men received hepatitis B vaccine (48%) than hepatitis A vaccine (43%). Compared with their counterparts, the percentage of men receiving a hepatitis B vaccine was lower among men who had no health insurance (42%), had only public insurance (41%), or were black (39%). The percentages of men who received a hepatitis B vaccine decreased with age and increased with education. Receipt of a hepatitis B vaccine was higher among men who identified as homosexual than among those who did not.
STD Testing
Of the 8,175 participants, 2,844 (35%) had been tested for syphilis during the past 12 months (Table 12). A larger percentage of men aged <30 years (40% of 3,587 men) reported being tested for syphilis during the past 12 months than men aged ≥30 years (31% of 4,588 men). Fewer men who did not have health insurance than those who had some type of health insurance reported having been tested for syphilis.
A total of 946 (12%) men had been diagnosed with an STD during the past 12 months. Specifically, 197 (2%) men were diagnosed with syphilis, 391 (5%) with gonorrhea, 268 (3%) with chlamydia, and 346 (4%) with some other STD. Other STD diagnoses reported by fewer numbers of men included herpes simplex virus, genital or anal warts, and pubic lice.
Behavioral Interventions
Overall, 1,436 (18%) of the men surveyed had participated in either an individual-level (14%) or group-level (7%) behavioral intervention during the past 12 months (Table 13). The percentages of men participating in HIV behavioral interventions were lowest among white men (13%) and highest among men aged 18--24 years (26%) and those who had public health insurance (24%). Among participants who participated in an HIV behavioral intervention in the 12 months before the interview, an HIV/AIDS-focused community-based organization was the most commonly reported provider for both individual-level (65%) and group-level (59%) interventions (Table 14).
Discussion
Sexual Behavior
Among MSM, unprotected anal sex is the sexual behavior with the highest risk for HIV transmission (12--16). Sexual transmission has been associated with nondisclosure of HIV infection with casual partners. Not discussing HIV status and not knowing a partner's HIV status were particularly common in the casual partnerships of the men surveyed. Efforts to improve communication skills related to HIV status and condom use with sexual partners might reduce the sexual transmission of HIV among MSM (25,26). However, almost half of the men who tested positive for HIV infection during the survey were unaware of their infection (6), highlighting the importance of consistent and correct condom use in the reduction of HIV infection. NHBS data, which are collected in venues frequented by MSM, indicate that participants meet most new partners in bars and clubs, on the Internet, or through chat lines. Therefore, interventions delivered in these settings might reach a large proportion of MSM at risk for HIV infection (27,28). NHBS data can be used to monitor the prevalence of risky sexual behaviors among MSM and identify areas of focus for reducing sexual transmission of HIV infection among MSM (3).
Alcohol and Drug Use
Use of alcohol or drugs can lead to HIV transmission either directly through injection-drug use or indirectly by facilitating risky sexual behaviors when a person is under the influence of alcohol or drugs. Among MSM, substance use is linked to risky sexual behaviors (29--31), particularly engaging in unprotected anal sex while under the influence of alcohol and some illegal drugs (32--35). Many men in this survey reported using alcohol and noninjection drugs during the past 12 months. This finding is not surprising because substance use generally is prevalent among urban gay and bisexual men (36). Especially concerning is that approximately half of the men who had used alcohol or drugs during their most recent sexual encounter also reported engaging in unprotected anal sex. In addition, some participants reported recreational use of erectile dysfunction drugs, poppers, and methamphetamine, which have been associated with greater risk for unsafe sex (37--40) and HIV infection among MSM (41--45). Reducing substance use among MSM can help reduce HIV transmission among MSM; however, to be as effective as possible, substance abuse treatment programs must address substance abuse and risky sexual behaviors simultaneously and educate counselors on sexual risky behaviors that are common among gay and bisexual men who use alcohol or drugs (46). Efforts have been made to create more culturally sensitive substance abuse programs for gay, lesbian, bisexual, and transgender persons (47). Because the NHBS data indicate that only a small proportion of the men surveyed had ever participated in an alcohol or drug treatment program, additional measures are needed to educate MSM about the risks associated with alcohol and drug use. Individual- and group-level behavioral interventions should focus on decreasing alcohol and drug use and reducing the risky sexual behaviors of MSM (48,49); community-level interventions that address both substance abuse and risky sexual behaviors might be needed. (Additional information available at http://www.cdc.gov/hiv/topics/research/prs/evidence-based-interventions.htm.) To continue to improve prevention efforts among MSM who use alcohol and drugs, data are needed to monitor emerging substance-use trends to inform the development or modification of HIV behavioral interventions because alcohol and drug-use patterns among MSM and their impact on the HIV epidemic continue to change (50).
Use of Prevention Services and Programs
HIV Testing
HIV-infected persons must know they are infected if they are to seek and receive treatment and prevention services, which are designed to reduce the likelihood that they will transmit HIV to others. Therefore, CDC recommends that all sexually active MSM be tested for HIV infection at least annually and that MSM with additional risk factors be tested every 3--6 months (17,22). In 2006, CDC revised HIV testing recommendations to promote routine, opt-out screening in health-care settings to increase HIV screening of patients, foster earlier detection of HIV infection, and link persons with previously unrecognized HIV infection to medical care and prevention services (17). Although HIV testing rates among MSM in this report were high, almost 40% of the men had not received an HIV test during the past year. A separate publication of NHBS data from this cycle indicated HIV prevalence was 19% for this sample and that a large proportion (44%) of the infected men were unaware of their infection (6). To increase the proportion of MSM who are tested annually, CDC recently expanded its enhanced HIV testing initiative to reach more MSM. (Additional information available at http://www.cdc.gov/hiv/topics/funding/ps10-10138/index.htm.) In addition, the reasons provided by NHBS participants for not being tested for HIV during the past 12 months indicate that some MSM might benefit from prevention efforts that increase their awareness of personal risk and decrease the fear associated with being infected. Structural interventions that decrease the social stigma associated with being infected with HIV could help decrease the fear associated with being HIV-positive and improve HIV testing rates because HIV-related stigma might cause some men to delay testing to avoid the social stress resulting from HIV infection (51).
Hepatitis Vaccination
The Advisory Committee on Immunization Practices (ACIP) first recommended vaccination to prevent the spread of hepatitis B virus among sexually active MSM in 1982 (52). However, only about half of the participants in NHBS had received a hepatitis vaccination. Two recent changes might increase the likelihood that men will receive a hepatitis vaccination. First, the Patient Protection and Affordable Care Act of 2010 expanded adult vaccination coverage by allowing individuals enrolled in group and individual health plans to have access (no copayment or other cost-sharing requirements) to ACIP-recommended vaccines, including those for hepatitis A and hepatitis B (53). (Additional information available at http://www.healthcare.gov/news/factsheets/affordable_care_act_immunization.html.) Second, ACIP recently recommended strategies for identifying unvaccinated adults who are at risk for hepatitis B infection. For example, providers of primary and specialty medical care should provide information about hepatitis B and the health benefits of hepatitis B vaccination to all adult patients (19). Still, these efforts might not reach all MSM at risk for hepatitis infection. Of NHBS participants, the lowest rates of hepatitis vaccination were among black men and men without private health insurance. More studies are needed to increase understanding of and reduce disparities in the receipt of hepatitis vaccinations.
STD Testing
To prevent STDs among sexually active MSM, CDC recommends annual testing for syphilis, gonorrhea, and chlamydia (22). Fewer than half of the sexually active men in the survey had been tested for syphilis during the past 12 months. Findings from the survey suggest that syphilis testing rates decline with age and increase with education. Therefore, efforts to educate sexually active MSM who are either older or less educated about the importance of STD testing might reduce STD transmission. To improve the monitoring of STD testing recommendations, the third cycle of NHBS questionnaires will include items to assess both gonorrhea and chlamydia testing.
Behavioral Interventions
Individual- and group-level behavioral interventions with demonstrated effectiveness have been a focus of CDC's prevention efforts (54). CDC has increased the number of effective behavioral interventions for young or minority MSM. (Additional information available at http://www.cdc.gov/hiv/topics/research/prs/evidence-based-interventions.htm.) During the past few years, CDC funded several community-based programs to provide HIV prevention services and improve the delivery and effectiveness of HIV prevention services in racial/ethnic minority communities at increased risk for infection. (Additional information available at http://www.cdc.gov/hiv/topics/funding/announcements.htm.) Of the men who reported participation in an individual- or a group-level intervention, a greater percentage were young or members of minority racial or ethnic groups. These findings suggest that these effective prevention programs are reaching the intended audience. However, only a small percentage of the men in the intended audience are being reached. More needs to be done to increase participation among both young men and men of color, as a separate analysis of these NHBS data showed disparities in HIV infection among of MSM (55).
HIV prevention has evolved over the past 30 years. What began as a grass-roots effort to provide HIV infection information has expanded to include HIV testing and linkage to medical care, partner services, biomedical and structural interventions, and behavioral interventions proven to be effective at reducing risk behaviors and HIV transmission among persons living with and at high risk for HIV infection (23,56). As HIV prevention activities for MSM continue to be developed and implemented, NHBS will provide updated data on the delivery of these services and programs to the populations who most need them. This report indicates a critical need to expand HIV prevention for MSM, emphasizing a combination of cost-effective and evidence-based biomedical, behavioral, and structural approaches that can result in the greatest possible improvements in HIV incidence, access to care, and HIV-related disparities.
Limitations
The findings in this report are subject to several limitations. First, a single standard for obtaining a representative sample of the MSM population in the United States has yet to be established (57). The venue-based, time-location sampling methods are used to produce estimates for hard-to-reach populations when sampling frames of the individual members of those populations do not exist or are difficult to construct. However, the data in this report are not weighted to account for variations in venue attendance or likelihood of being selected to participate in the survey. Second, these data might not include all MSM living in the MSA because the venue sampling frames do not account for MSM who do not attend those venues. In addition, certain venues attended by MSM at high risk (e.g., cruising locations) might have been underrepresented. Third, findings from the MSAs included in this report might not be generalizable to other U.S. states or cities. Fourth, because the survey was administered by an interviewer, certain behaviors might have been underreported or overreported. For example, participants might have underreported socially undesirable behaviors (e.g., drug use) or might have overreported socially desirable behaviors (e.g., using condoms during anal sex or being tested recently). Fifth, perceived knowledge of a partner's HIV status should be interpreted with caution because this information might be inaccurate, especially in groups for which high rates of undiagnosed HIV infection have been reported (6). Sixth, the estimates of hepatitis vaccination might not represent the percentage of persons adequately vaccinated for hepatitis because maximum protection requires multiple doses of the vaccine. In addition, participants had difficulty differentiating between hepatitis A and hepatitis B vaccine, and some participants might be unaware that they had been vaccinated against hepatitis B at birth. Others might not have been eligible for vaccination because of chronic hepatitis infection or immunity from previous vaccination or infection. Such information was not collected in the NHBS interview. Seventh, in some instances, stratification by demographic characteristics might have produced numbers that were too small for reliable interpretation. Because statistical tests were not performed, differences in behaviors between groups should be interpreted with caution. Finally, because most of the NHBS participants were recruited at bars and dance clubs, the percentage of MSM who reported drinking alcoholic beverages might be higher than the actual percentage among MSM in general. However, the percentage of participants who drank alcohol in the past year was similar to that found in an urban household survey of MSM (36).
Caution should be used when comparing these numbers with previous NHBS MSM data (5). The percentages reported in this report might have been influenced by differences in the survey instruments (e.g., the definition of casual partner or assessment of the most recent partner) and in the venues on the monthly sampling frame. In addition, the data in this report might have been influenced by the six participating areas that contributed to this cycle of NHBS data collection but not to the first cycle.
Conclusion
The White House Office of National AIDS Policy coordinates government efforts to reduce the number of HIV infections in the United States. For the first time in U.S. history, a national strategy has been developed to address the domestic HIV epidemic (3). The primary objectives of the National HIV/AIDS Strategy are to reduce HIV incidence, increase access to care and optimize health outcomes for people living with HIV, and reduce HIV-related health disparities. One important step in achieving the strategy's goal of a 25% reduction in new infections by 2015 is for HIV programs across the federal government and among state and local governments to coordinate intensified HIV prevention efforts in the communities where HIV is most heavily concentrated by using a combination of effective evidence-based approaches. In addition, state and local health departments as well as federal agencies are expected to monitor progress towards the strategy's goals. A nationally united effort and strategy will help reduce the effects of HIV in groups at risk, especially MSM.
In addition to the National HIV/AIDS Strategy, recent efforts to improve health care could serve as a structural intervention in preventing HIV infection. Health-care reform, which is yet to be fully enacted, could decrease disparities seen in HIV infection by expanding Medicaid programs to provide coverage to more persons living in or almost in poverty, improving access to preventive services covered by Medicaid, requiring that states participating in Medicaid establish procedures for conducting outreach to and enrolling vulnerable and underserved populations eligible for medical assistance, including persons with HIV, and the elimination of preexisting conditions exclusions by private insurers. (Additional information available at http://www.healthcare.gov.) Once enacted, expanded health insurance coverage should also increase access to services such as HIV testing, hepatitis vaccination, and STD screening. CDC is committed to exploring the integration of these services to further improve the delivery of health services to persons with multiple risks (http://www.cdc.gov/nchhstp/programintegration) and has prioritized the development of programs that take into consideration the social determinants of health to promote health equity (http://www.cdc.gov/socialdeterminants). As these structural interventions in health care are developed and implemented, NHBS will provide updated data regarding the impact of these interventions on populations at risk for HIV infection.
Multiple indicators are relevant to HIV risk and prevention among MSM of various backgrounds. A better understanding of the behaviors and circumstances associated with HIV transmission can improve the development of appropriate prevention responses. Of particular importance is the high proportion of MSM of all races and ethnicities who engage in unprotected anal sex and do not discuss their HIV status beforehand, which are behaviors that can lead to HIV infection. Many MSM in the survey reported recent receipt of an HIV test. MSM should consistently share their HIV test results with all their sex partners and ask sex partners about their recent HIV status and whether they have been tested recently. Persons need to know their own HIV status and that of their partners to make healthy decisions about sexual behavior. Use of noninjection drugs can increase risky sexual behaviors, and the use of noninjection drugs in combination with sex is prevalent among MSM. The combination of drug use and unprotected sex with partners of unknown HIV serostatus should be explored more fully to better explain how this behavior contributes to continued HIV transmission among MSM.
NHBS is a key component of the comprehensive CDC approach to reducing the spread of HIV in the United States and will continue to be the primary source of data for monitoring behaviors of populations at high risk for HIV infection. Data from NHBS can be used to monitor specific risk behaviors, HIV testing experiences, and use of prevention programs; identify the demographic and behavioral correlates of risk; and direct future prevention activities to reduce HIV transmission.
Acknowledgments
This report is based, in part, on the contributions of members of the NHBS working group: J. Taussig, R. Gern, T. Hoyte, L. Salazar, Atlanta, Georgia; C. Flynn, F. Sifakis, Baltimore, Maryland; D. Isenberg, M. Driscoll, E. Hurwitz, Boston, Massachusetts; N. Prachand, N. Benbow, Chicago, Illinois; S. Melville, P. Pannala, R. Yeager, A. Sayegh, J. Dyer, A. Novoa, Dallas, Texas; M. Thrun, A. Al-Tayyib, R. Wilmoth, Denver, Colorado; E. Higgins, V. Griffin, E. Mokotoff, Detroit, Michigan; M.Wolverton, J. Risser, H. Rehman, Houston, Texas; T. Bingham, E. Sey, Los Angeles, California; M. LaLota, L. Metsch, D. Beck, D. Forrest, G. Cardenas, Miami, Florida; W.T. Robinson, D. Gruber, New Orleans, Louisiana; C. Nemeth, C. Watson, Nassau-Suffolk, New York; C. Murrill, A. Neaigus, S. Jenness, H. Hagan, T. Wendel, New York City, New York; H. Cross, B. Bolden, S. D'Errico, Newark, New Jersey; K. Brady, A. Kirkland, Philadelphia, Pennsylvania; M. Herbert, Y. Friedberg, D. Wrigley, J. Fisher, St. Louis, Missouri; V. Miguelino, A. Velasco, San Diego, California; H. Raymond, W. McFarland, San Francisco, California; S.M. De León, Y. Rolón-Colón, San Juan, Puerto Rico; M. Courogen, H. Thiede, N. Snyder, R. Burt, Seattle, Washington; and P. Cunningham, M. Sansone, T. West-Ojo, M. Magnus, I. Kuo, District of Columbia; and by members of the Behavioral Surveillance team and M. Morgan, Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC.
References
- CDC. HIV prevalence estimates---United States, 2006. MMWR 2008;57:1074--7.
- Hall HI, Song R, Rhodes P, et al. Estimation of HIV incidence in the United States. JAMA 2008;300:520--9.
- The White House, Office of National AIDS Policy. National HIV/AIDS strategy for the United States. Washington, DC: Office of National AIDS Policy. Available at http://www.whitehouse.gov/onap. Accessed September 15, 2011.
- Gallagher KM, Sullivan PS, Lansky A, Onorato IM. Behavioral surveillance among people at risk for HIV infection in the U.S.: the National HIV Behavioral Surveillance System. Public Health Rep 2007;(Suppl 1):32--8.
- Sanchez T, Finlayson T, Drake A, et al. Human immunodeficiency virus (HIV) risk, prevention, and testing behaviors---United States, National HIV Behavioral Surveillance System: men who have sex with men, November 2003--April 2005. MMWR 2006;55(No. SS-6).
- CDC. Prevalence and awareness of HIV infection among men who have sex with men---21 cities, United States, 2008. MMWR 2010;59:1202--7.
- CDC. HIV/AIDS surveillance report, 2008. Vol. 20. Atlanta, GA: CDC; 2010. Available at http://www.cdc.gov/hiv/topics/surveillance/resources/reports. Accessed September 15, 2011.
- MacKellar D, Gallagher K, Finlayson T, Sanchez T, Lansky A, Sullivan PS. Surveillance of HIV risk and prevention behaviors of men who have sex with men: a national application of venue-based, time-space sampling. Public Health Rep 2007; (Suppl 1):39--48.
- Allen DR, Finlayson T, Abdul-Quader A, Lansky A. The role of formative research in the National HIV Behavioral Surveillance System. Public Health Rep 2009;124:26--33.
- Murrill, CS, Kai-lih, L, Guilin, V, et al. HIV prevalence and associated risk behaviors in New York City's house ball community. Am J Public Health 2008; 98:1074--80.
- Roberts, FR. There's no place like home: a history of house ball culture. Wiretap. June 6, 2007. Available at http://www.wiretapmag.org/arts/43120.
- Koblin BA, Husnki MJ, Colfax G, et al. Risk factors for HIV infection among men who have sex with men. AIDS 2006;20:731--9.
- Ekstrand ML, Stall RD, Paul JP, Osmond DH, Coates TJ. Gay men report high rates of unprotected anal sex with partners of unknown or discordant HIV status. AIDS 1999;13:1525--33.
- Morin SF, Steward WT, Charlebois ED, et al. Predicting HIV transmission risk among HIV-infected men who have sex with men: findings from the healthy living project. J Acquir Immune Defic Syndr 2005;40:226--35.
- Chen SY, Gibson S, Katz M, et al. Continued increases in sexual risk behavior and sexually transmitted diseases among men who have sex with men: San Francisco, Calif. 1999--2001. Am J Public Health 2002;92:1387--8.
- Crepaz N, Marks G, Liau A, et al. Prevalence of unprotected anal intercourse among HIV-diagnosed MSM in the United States: a meta-analysis. AIDS 2009;23:1617--29.
- CDC. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR 2006;55(No. RR-14):1--17.
- CDC. Prevention of hepatitis A through active or passive immunization. MMWR 2006;55(RR-7).
- CDC. A comprehensive immunization strategy to eliminate transmission of hepatitis B virus infection in the United States. MMWR 2006;55(No. RR-16).
- Stall R, Hays R, Waldo C, Ekstrand M, McFarland W. The gay '90s: a review of research in the 1990s on sexual behavior and HIV risk among men who have sex with men. AIDS 2000;14:S1--S14
- Fleming DT, Wasserheit JN. From epidemiologic synergy to public health policy and practice: the contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect 1999;75:3--17.
- CDC. Sexually transmitted diseases treatment guidelines, 2010. MMWR 2010;59(No. RR-12)
- Herbst JH, Sherba T, Crepaz N, et al. A meta-analytic review of HIV behavioral interventions for reducing sexual risk behaviors of men who have sex with men. J Acquir Immune Defic Syndr 2005;39:228--41.
- CDC. Evaluating CDC-funded health department HIV prevention programs. Atlanta, GA: CDC; 1999. Available at http://www.cdc.gov/hiv/topics/evaluation/health_depts/guidance. Accessed September 15, 2011.
- Molitor F, Facer M, Ruiz JD. Safer sex communication and unsafe sexual behavior among young men who have sex with men in California. Arch Sex Behav 1999;28:335--43.
- Chesney MA, Koblin BA, Barresi PJ, et al. An individually tailored intervention for HIV prevention: baseline data from the EXPLORE Study. Am J Public Health 2003;93:933--8.
- Kegeles SM, Hays RB, Coates TJ. The Mpowerment project: a community-level HIV prevention intervention for young gay men. Am J Public Health 1996;86:1129--36.
- Wohlfeiler D. Structural interventions for HIV prevention among gay men/men who have sex with men (MSM). Richmond, CA: California Department of Health Services; 2005. Available at http://www.effectiveinterventions.org/files/structintervmsm.pdf. Accessed September 16, 2011.
- Irwin TW, Morgenstern J, Parsons JT, Wainberg M, Labouvie E. Alcohol and sexual HIV risk behavior among problem drinking men who have sex with men: an event level analysis of timeline followback data. AIDS Behav 2006;10:299--307.
- Mustanski B. Moderating effects of age on the alcohol and sexual risk taking association: an online daily diary study of men who have sex with men. AIDS Behav 2008;12:118--26.
- Stall R, Purcell, DW Intertwining epidemics: a review of research on substance use among men who have sex with men and its connection to the AIDS epidemic. AIDS Behav 2000;4:181--92.
- Purcell DW, Parsons JT, Halkitis PN, Mizuno Y, Woods WJ. Substance use and sexual transmission risk behavior of HIV-positive men who have sex with men. J Subst Abuse 2001;13(1--2):185--200.
- Mansergh G, Colfax GN, Marks G, Rader M, Guzman R, Buchbinder S. The Circuit Party Men's Health Survey: findings and implications for gay and bisexual men. Am J Public Health 2001;91:953--8.
- Celentano DD, Valleroy LA, Sifakis F, et al. Associations between substance use and sexual risk among very young men who have sex with men. Sex Transm Dis 2006;33:265--71.
- Hirshfield S, Remien RH, Humbersone M, Walavalkar I, Chiasson MA. Substance use and high-risk sex among men who have sex with men: a national online study in the USA. AIDS Care 2004;16:1036--47.
- Stall R, Paul JP, Greenwood G, et al. Alcohol use, drug use and alcohol-related problems among men who have sex with men: the Urban Men's Health Study. Addiction 2001;96:1589--601.
- Semple SJ, Strathdee SA, Zians J, Patterson TL. Sexual risk behavior associated with co-administration of methamphetamine and other drugs in a sample of HIV-positive men who have sex with men. Am J Addict 2009;18:65--72.
- Colfax G, Coates TJ, Husnik MJ, et al. Longitudinal patterns of methamphetamine, popper (amyl nitrite), and cocaine use and high-risk sexual behavior among a cohort of San Francisco men who have sex with men. J Urban Health 2005;82(Suppl 1):i62--70. Doi: 10.1093/jurban/jti025.
- Purcell DW, Wolitski RJ, Hoff CC, Parsons JT, Woods WJ, Halkitis PN. Predictors of the use of Viagra, testosterone, and antidepressants among HIV-seropositive gay and bisexual men. AIDS 2005;19 (Suppl 1):S57--66.
- Drumright LN, Strathdee SA, Little SJ, et al. Unprotected anal intercourse and substance use before and after HIV diagnosis among recently HIV-infected men who have sex with men. Sex Transm Dis 2007;34:401--7.
- Buchbinder SP, Vittinghoff E, Heagerty PJ, et al. Sexual risk, nitrite inhalant use, and lack of circumcision associated with HIV seroconversion in men who have sex with men in the United States. J Acquir Immune Defic Syndr 2005;39:82--9.
- Chesney M, Barret DC, Stall R. Histories of substance abuse and HIV risk behavior: precursors to HIV seroconversion in homosexual men. Am J Public Health 1998;88:113--6.
- Drumright LN, Gorbach PM, Little SJ, et al. Associations between substance use, erectile dysfunction medication and recent HIV infection among men who have sex with men. AIDS Behav 2009;13:328--36.
- Ostrow DG, Plankey MW, Cox C, et al. Specific sex drug combinations contribute to the majority of recent HIV seroconversions among MSM in the MACS. J Acquir Immune Defic Syndr 2009;51:349--55.
- Carey JW, Mejia R, Bingham T, et al. Drug use, high-risk sex behaviors, and increased risk for recent HIV infection among men who have sex with men in Chicago and Los Angeles. AIDS Behav 2009;13:1084--96. Doi:10.1007/s10461--008--9404--3 .
- Shoptaw S, Frosch D. Substance abuse treatment as HIV prevention for men who have sex with men. AIDS Behav 2000;4:193--203.
- Substance Abuse and Mental Health Services Administration. A provider's introduction to substance abuse treatment for lesbian, gay, bisexual, and transgender individuals. Rockville, MD: US Department of Health and Human Services, SAMHSA; 2001. Available at http://kap.samhsa.gov/products/manuals/pdfs/lgbt.pdf. Accessed September 15, 2011.
- Colfax G. The epidemiology of substance use and sexual risk behavior among men who have sex with men: implications for HIV prevention interventions [abstract No. 55]. Paper presented at the 12th Conference on Retroviruses and Opportunistic Infections. Boston, MA; February 22--25, 2005. Available at http://www.retroconference.org/2005/cd/abstracts/25846.htm. Accessed September 15, 2011.
- Tieu HV, Koblin BA. HIV, alcohol, and noninjection drug use. Curr Opin HIV AIDS 2009;4:314--8.
- Lambert E, Normand J, Stall R, Aral S, Vlahov D. Introduction: new dynamics of HIV risk among drug-using men who have sex with men. J Urban Health 2005;82(Suppl 1):i1--8. Doi: 10.1093/jurban/jti018.
- Chesney MA, Smith AW. Critical delays in HIV testing and care: the potential role of stigma. Am Behav Sci 1999;42:1162--74.
- CDC. Recommendation of the Immunization Practices Advisory Committee (ACIP) inactivated hepatitis B virus vaccine. MMWR 1982;31:317--22,327--8.
- The Patient Protection and Affordable Care Act of 2010. Pub. L. No. 111--148, 124 Stat. 119.
- CDC. Compendium of HIV prevention interventions with evidence of effectiveness. Atlanta, GA: US Department of Health and Human Services; 1999. Available at http://www.cdc.gov/hiv/resources/reports/hiv_compendium/pdf/HIVcompendium.pdf. Accessed September 16, 2011.
- Oster A, Weigand R, Sionean C, et al. Understanding disparities in HIV infection between black and white men who have sex with men in the United States: data from the National HIV Behavioral Surveillance system. Paper presented at the International AIDS Conference. Vienna, Austria; July 18--20, 2010.
- CDC. Evolution of HIV/AIDS Prevention Programs---United States, 1981--2006. MMWR 2006;55:597--603.
- Lansky A, MacKellar D, Gallagher KM, Lin LS, Sullivan PS, Onorato IM. [Untitled letter]. Sex Transm Dis 2006;33:272-3. Doi: 10.1097/01.olq.0000215745.61542.d4.
* The house ball community is a social network of black and Hispanic youths who are generally considered to be gay, lesbian, bisexual, or transgender. The community culture started in Harlem during the 1920s with drag balls and later incorporated alternate kinship networks known as houses. Today, house ball communities are present in many U.S. cities (10,11).
Alternate Text: This figure is a map of the United States and Puerto Rico showing the following principal cities of each metropolitan statistical area participating in the 2008 National HIV Behavioral Surveillance System: Men Who Have Sex With Men: Atlanta, Georgia; Baltimore, Maryland; Boston, Massachusetts; Chicago, Illinois; Dallas, Texas; Denver, Colorado; Detroit, Michigan; Houston, Texas; Los Angeles, California; Miami, Florida; Nassau-Suffolk, New York; New Orleans, Louisiana; New York, New York; Newark, New Jersey; Philadelphia, Pennsylvania; St. Louis, Missouri; San Diego, California; San Francisco, California; San Juan, Puerto Rico; Seattle, Washington; and Washington, DC.
FIGURE 2. Percentage of participants who had a new male partner during the past 12 months (N = 7,780) and discussed HIV status before first sexual encounter --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008
Abbreviations: HIV = human immunodeficiency virus.
* A man with whom the participant had sex and to whom he felt most committed (e.g., boyfriend, spouse, significant other, or life partner).
† A man with whom the participant had sex but to whom he did not feel committed, whom he did not know very well, or with whom the participant had sex in exchange for something such as money or drugs.
Alternate Text: This figure is a bar chart showing the percentage of participants in the 2008 National HIV Behavioral Surveillance System: Men Who Have Sex With Men who had a new male partner during the past 12 months (N = 7,780) and discussed HIV status before first sexual encounter. Of the 8,175 participants, 2,587 (32%) reported having new main male partners, and 5,193 (64%) reported having new casual male partners during the past 12 months. A larger proportion of men had discussed the HIV infection status of themselves and their partners with all main partners than with all casual partners.
|
TABLE 1. (Continued) Number* and percentage† of participants, by selected characteristics, recruitment venue, and metropolitan statistical area --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
||
|---|---|---|
|
Characteristic |
No. |
(%) |
|
Metropolitan statistical area (division) |
|
|
|
Atlanta, Georgia |
334 |
(4) |
|
Baltimore, Maryland |
455 |
(6) |
|
Boston, Massachusetts |
252 |
(3) |
|
Chicago, Illinois |
516 |
(6) |
|
Dallas, Texas |
444 |
(5) |
|
Denver, Colorado |
452 |
(6) |
|
Detroit, Michigan |
362 |
(4) |
|
Houston, Texas |
355 |
(4) |
|
Los Angeles, California |
469 |
(6) |
|
Miami, Florida |
455 |
(6) |
|
Nassau-Suffolk, New York |
264 |
(3) |
|
New Orleans, Louisiana |
395 |
(5) |
|
New York, New York |
483 |
(6) |
|
Newark, New Jersey |
86 |
(1) |
|
Philadelphia, Pennsylvania |
544 |
(7) |
|
St. Louis, Missouri |
332 |
(4) |
|
San Diego, California |
476 |
(6) |
|
San Francisco, California |
395 |
(5) |
|
San Juan, Puerto Rico |
343 |
(4) |
|
Seattle, Washington |
314 |
(4) |
|
Washington, DC |
449 |
(5) |
|
Total |
8,175 |
(100) |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to total because of missing or unknown data. † Percentages might not add to 100 because of rounding. § Persons of Hispanic/Latino ethnicity might be of any race. ¶ Other race; includes multiple races. ** GED diploma. †† Coverage through private insurance policies or employer, TRICARE, CHAMPUS, or membership in a health maintenance organization. §§ Coverage through Medicare, Medicaid, or Veterans Administration. ¶¶ Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. |
||
|
TABLE 2. (Continued) Number* and percentage of participants who reported having had anal sex with a main or casual male partner during the past 12 months, by selected demographic and other characteristics and metropolitan statistical area --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Characteristic |
Main partner† anal sex |
Casual partner§ anal sex |
Total |
||||||
|
Total |
Unprotected¶ |
Total |
Unprotected |
||||||
|
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%) |
||
|
Metropolitan statistical area |
|||||||||
|
Atlanta, Georgia |
128 |
(38) |
110 |
(86) |
223 |
(67) |
114 |
(51) |
334 |
|
Baltimore, Maryland |
266 |
(58) |
156 |
(59) |
258 |
(57) |
97 |
(38) |
455 |
|
Boston, Massachusetts |
127 |
(50) |
89 |
(70) |
144 |
(57) |
54 |
(38) |
252 |
|
Chicago, Illinois |
322 |
(62) |
184 |
(57) |
276 |
(53) |
115 |
(42) |
516 |
|
Dallas, Texas |
263 |
(59) |
175 |
(67) |
247 |
(56) |
142 |
(57) |
444 |
|
Denver, Colorado |
245 |
(54) |
170 |
(69) |
262 |
(58) |
131 |
(50) |
452 |
|
Detroit, Michigan |
220 |
(61) |
127 |
(58) |
193 |
(53) |
77 |
(40) |
362 |
|
Houston, Texas |
219 |
(62) |
156 |
(71) |
193 |
(54) |
104 |
(54) |
355 |
|
Los Angeles, California |
259 |
(55) |
168 |
(65) |
257 |
(55) |
123 |
(48) |
469 |
|
Miami, Florida |
245 |
(54) |
168 |
(69) |
321 |
(71) |
142 |
(44) |
455 |
|
Nassau-Suffolk, New York |
149 |
(56) |
102 |
(68) |
131 |
(50) |
47 |
(36) |
264 |
|
New Orleans, Louisiana |
220 |
(56) |
139 |
(63) |
187 |
(47) |
71 |
(38) |
395 |
|
New York, New York |
278 |
(58) |
171 |
(62) |
278 |
(58) |
103 |
(37) |
483 |
|
Newark, New Jersey |
56 |
(65) |
37 |
(66) |
39 |
(45) |
10 |
(26) |
86 |
|
Philadelphia, Pennsylvania |
374 |
(69) |
187 |
(50) |
198 |
(36) |
96 |
(48) |
544 |
|
St. Louis, Missouri |
208 |
(63) |
145 |
(70) |
158 |
(48) |
68 |
(43) |
332 |
|
San Diego, California |
257 |
(54) |
180 |
(70) |
252 |
(53) |
133 |
(53) |
476 |
|
San Francisco, California |
202 |
(51) |
149 |
(74) |
245 |
(62) |
111 |
(45) |
395 |
|
San Juan, Puerto Rico |
229 |
(67) |
145 |
(63) |
193 |
(56) |
81 |
(42) |
343 |
|
Seattle, Washington |
174 |
(55) |
138 |
(79) |
206 |
(66) |
118 |
(57) |
314 |
|
Washington, DC |
251 |
(56) |
164 |
(65) |
291 |
(65) |
133 |
(46) |
449 |
|
Total |
4,692 |
(57) |
3,060 |
(65) |
4,552 |
(56) |
2,070 |
(45) |
8,175 |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † A man with whom the participant had sex and to whom he felt most committed (e.g., boyfriend, spouse, significant other, or life partner). § A man with whom the participant had sex but to whom he did not feel committed, whom he did not know very well, or with whom the participant had sex in exchange for something such as money or drugs. ¶ Neither the participant nor his partner used a condom. Proportion reported is that of all participants who engaged in anal sex with that type of partner. ** Persons of Hispanic/Latino ethnicity might be of any race. †† Other race; includes multiple races §§ GED diploma. ¶¶ Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. |
|||||||||
|
TABLE 4. (Continued) Number* and percentage of participants who reported having had sex both with male and female partners during the past 12 months, by selected demographic and other characteristics and metropolitan statistical area --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
Characteristic |
Female partner |
Male partner |
Total with male and female partners§ |
|||||||
|
Vaginal or anal sex |
Unprotected vaginal or anal sex† |
Anal sex |
Unprotected anal sex† |
|||||||
|
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%)¶ |
|
|
Metropolitan statistical area |
||||||||||
|
Atlanta, Georgia |
15 |
(94) |
11 |
(73) |
16 |
(100) |
11 |
(69) |
16 |
(5) |
|
Baltimore, Maryland |
108 |
(97) |
57 |
(53) |
84 |
(76) |
33 |
(39) |
111 |
(24) |
|
Boston, Massachusetts |
13 |
(100) |
8 |
(62) |
8 |
(62) |
---** |
---** |
13 |
(5) |
|
Chicago, Illinois |
50 |
(94) |
28 |
(56) |
46 |
(87) |
25 |
(54) |
53 |
(10) |
|
Dallas, Texas |
101 |
(96) |
79 |
(78) |
77 |
(73) |
52 |
(68) |
105 |
(24) |
|
Denver, Colorado |
35 |
(92) |
22 |
(63) |
27 |
(71) |
16 |
(59) |
38 |
(8) |
|
Detroit, Michigan |
60 |
(97) |
42 |
(70) |
52 |
(84) |
26 |
(50) |
62 |
(17) |
|
Houston, Texas |
58 |
(95) |
36 |
(62) |
42 |
(69) |
29 |
(69) |
61 |
(17) |
|
Los Angeles, California |
56 |
(100) |
33 |
(59) |
45 |
(80) |
25 |
(56) |
56 |
(12) |
|
Miami, Florida |
143 |
(98) |
110 |
(77) |
125 |
(86) |
70 |
(56) |
146 |
(32) |
|
Nassau-Suffolk, New York |
38 |
(95) |
21 |
(55) |
27 |
(68) |
8 |
(30) |
40 |
(15) |
|
New Orleans, Louisiana |
53 |
(96) |
31 |
(58) |
41 |
(75) |
23 |
(56) |
55 |
(14) |
|
New York, New York |
76 |
(96) |
46 |
(61) |
65 |
(82) |
34 |
(52) |
79 |
(16) |
|
Newark, New Jersey |
9 |
(100) |
7 |
(78) |
7 |
(78) |
---** |
---** |
9 |
(10) |
|
Philadelphia, Pennsylvania |
52 |
(93) |
29 |
(56) |
46 |
(82) |
26 |
(57) |
56 |
(10) |
|
St. Louis, Missouri |
26 |
(96) |
13 |
(50) |
20 |
(74) |
13 |
(65) |
27 |
(8) |
|
San Diego, California |
24 |
(96) |
14 |
(58) |
24 |
(96) |
13 |
(54) |
25 |
(5) |
|
San Francisco, California |
40 |
(98) |
28 |
(70) |
31 |
(76) |
18 |
(58) |
41 |
(10) |
|
San Juan, Puerto Rico |
46 |
(98) |
27 |
(59) |
41 |
(87) |
22 |
(54) |
47 |
(14) |
|
Seattle, Washington |
22 |
(88) |
13 |
(59) |
23 |
(92) |
12 |
(52) |
25 |
(8) |
|
Washington, DC |
42 |
(95) |
22 |
(52) |
37 |
(84) |
19 |
(51) |
44 |
(10) |
|
Total |
1,067 |
(96) |
677 |
(63) |
884 |
(80) |
481 |
(54) |
1,109 |
(14) |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † Neither the participant nor his partner used a condom. Proportion reported is that of all participants who engaged in sexual intercourse with a partner of that sex. § Includes main and casual partners of any sex. ¶ Proportion of all participants in each demographic group who reported both male and female sex partners during the past 12 months. ** Suppressed because the number or numerator was less than 5. †† Persons of Hispanic/Latino ethnicity might be of any race. §§ Other race; includes multiple races. ¶¶ GED diploma. *** Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. |
||||||||||
|
TABLE 6. (Continued) Number* and percentage of participants who reported substance use during the past 12 months, by type of drug, selected demographic and other characteristics, and metropolitan statistical area --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Characteristic |
Marijuana |
Cocaine |
Popper (amyl nitrate) |
Ecstasy |
Methamphetamine |
Total |
|||||
|
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%) |
No. |
(%) |
||
|
Metropolitan statistical area |
|||||||||||
|
Atlanta, Georgia |
90 |
(27) |
35 |
(10) |
55 |
(16) |
35 |
(10) |
28 |
(8) |
334 |
|
Baltimore, Maryland |
230 |
(51) |
72 |
(16) |
26 |
(6) |
48 |
(11) |
13 |
(3) |
455 |
|
Boston, Massachusetts |
109 |
(43) |
54 |
(21) |
56 |
(22) |
21 |
(8) |
15 |
(6) |
252 |
|
Chicago, Illinois |
202 |
(39) |
59 |
(11) |
65 |
(13) |
38 |
(7) |
20 |
(4) |
516 |
|
Dallas, Texas |
174 |
(39) |
89 |
(20) |
42 |
(9) |
48 |
(11) |
39 |
(9) |
444 |
|
Denver, Colorado |
165 |
(37) |
85 |
(19) |
75 |
(17) |
60 |
(13) |
44 |
(10) |
452 |
|
Detroit, Michigan |
161 |
(44) |
67 |
(19) |
37 |
(10) |
37 |
(10) |
11 |
(3) |
362 |
|
Houston, Texas |
144 |
(41) |
74 |
(21) |
43 |
(12) |
52 |
(15) |
34 |
(10) |
355 |
|
Los Angeles, California |
191 |
(41) |
82 |
(17) |
70 |
(15) |
59 |
(13) |
60 |
(13) |
469 |
|
Miami, Florida |
137 |
(30) |
113 |
(25) |
74 |
(16) |
39 |
(9) |
27 |
(6) |
455 |
|
Nassau-Suffolk, New York |
91 |
(34) |
44 |
(17) |
36 |
(14) |
13 |
(5) |
6 |
(2) |
264 |
|
New Orleans, Louisiana |
165 |
(42) |
102 |
(26) |
67 |
(17) |
64 |
(16) |
41 |
(10) |
395 |
|
New York, New York |
210 |
(43) |
124 |
(26) |
62 |
(13) |
55 |
(11) |
26 |
(5) |
483 |
|
Newark, New Jersey |
33 |
(38) |
5 |
(6) |
---† |
---† |
15 |
(17) |
---† |
---† |
86 |
|
Philadelphia, Pennsylvania |
103 |
(19) |
53 |
(10) |
---† |
---† |
39 |
(7) |
10 |
(2) |
544 |
|
St. Louis, Missouri |
115 |
(35) |
56 |
(17) |
41 |
(12) |
24 |
(7) |
10 |
(3) |
332 |
|
San Diego, California |
168 |
(35) |
55 |
(12) |
36 |
(8) |
44 |
(9) |
40 |
(8) |
476 |
|
San Francisco, California |
204 |
(52) |
108 |
(27) |
73 |
(18) |
77 |
(19) |
37 |
(9) |
395 |
|
San Juan, Puerto Rico |
71 |
(21) |
32 |
(9) |
24 |
(7) |
---† |
---† |
---† |
---† |
343 |
|
Seattle, Washington |
180 |
(57) |
78 |
(25) |
71 |
(23) |
54 |
(17) |
40 |
(13) |
314 |
|
Washington, DC |
175 |
(39) |
86 |
(19) |
98 |
(22) |
44 |
(10) |
24 |
(5) |
449 |
|
Total |
3,118 |
(38) |
1,473 |
(18) |
1,057 |
(13) |
868 |
(11) |
528 |
(6) |
8,175 |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † Suppressed because the number or numerator was less than 5. § Persons of Hispanic/Latino ethnicity might be of any race. ¶ Other race; includes multiple races. ** GED diploma. †† Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. §§ Length of time since participating in an alcohol or drug treatment program. |
|||||||||||
|
TABLE 7. (Continued) Number* and percentage of participants who reported current alcohol use and heavy or binge drinking during the past 30 days, by selected demographic and other characteristics and metropolitan statistical area --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
|||||||
|---|---|---|---|---|---|---|---|
|
Characteristic |
Current† |
Heavy§ |
Binge¶ |
Total |
|||
|
No. |
(%) |
No. |
(%) |
No. |
(%) |
||
|
Metropolitan statistical area |
|||||||
|
Atlanta, Georgia |
279 |
(84) |
27 |
(8) |
158 |
(47) |
334 |
|
Baltimore, Maryland |
380 |
(84) |
69 |
(15) |
200 |
(44) |
455 |
|
Boston, Massachusetts |
230 |
(91) |
38 |
(15) |
127 |
(50) |
252 |
|
Chicago, Illinois |
472 |
(91) |
98 |
(19) |
264 |
(51) |
516 |
|
Dallas, Texas |
370 |
(83) |
87 |
(20) |
227 |
(51) |
444 |
|
Denver, Colorado |
407 |
(90) |
95 |
(21) |
276 |
(61) |
452 |
|
Detroit, Michigan |
297 |
(82) |
59 |
(16) |
167 |
(46) |
362 |
|
Houston, Texas |
320 |
(90) |
101 |
(28) |
201 |
(57) |
355 |
|
Los Angeles, California |
390 |
(83) |
42 |
(9) |
208 |
(44) |
469 |
|
Miami, Florida |
368 |
(81) |
69 |
(15) |
176 |
(39) |
455 |
|
Nassau-Suffolk, New York |
221 |
(84) |
20 |
(8) |
115 |
(44) |
264 |
|
New Orleans, Louisiana |
361 |
(91) |
106 |
(27) |
234 |
(59) |
395 |
|
New York, New York |
391 |
(81) |
92 |
(19) |
222 |
(46) |
483 |
|
Newark, New Jersey |
62 |
(72) |
13 |
(15) |
30 |
(35) |
86 |
|
Philadelphia, Pennsylvania |
324 |
(60) |
48 |
(9) |
103 |
(19) |
544 |
|
St. Louis, Missouri |
299 |
(90) |
64 |
(19) |
198 |
(60) |
332 |
|
San Diego, California |
377 |
(79) |
64 |
(13) |
193 |
(41) |
476 |
|
San Francisco, California |
343 |
(87) |
75 |
(19) |
219 |
(55) |
395 |
|
San Juan, Puerto Rico |
289 |
(84) |
90 |
(26) |
178 |
(52) |
343 |
|
Seattle, Washington |
284 |
(90) |
76 |
(24) |
192 |
(61) |
314 |
|
Washington, DC |
420 |
(94) |
68 |
(15) |
265 |
(59) |
449 |
|
Total |
6,884 |
(84) |
1,401 |
(17) |
3,953 |
(57) |
8,175 |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † Participants who drank at least one alcoholic beverage during the past 30 days. Alcoholic beverage was defined as a 12-oz beer, 5-oz glass of wine, or 1.5 shot of liquor. § The proportion of participants who drank on average more than two alcoholic beverages per day in the 30 days before the interview. ¶ The proportion of participants who drank more than five alcoholic beverages at one sitting in the 30 days before the interview. ** Persons of Hispanic/Latino ethnicity might be of any race. †† Other race; includes multiple races. §§ GED diploma. ¶¶ Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. *** Length of time since participating in an alcohol or drug treatment program. |
|||||||
|
TABLE 8. (Continued) Number* and percentage of participants who reported having ever been tested for HIV infection or tested during the past 12 months, by selected demographic and other characteristics and metropolitan statistical area ---National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
|||||
|---|---|---|---|---|---|
|
Characteristic |
Ever tested |
Tested during past 12 mos |
Total |
||
|
No. |
(%)† |
No. |
(%)§ |
||
|
Metropolitan statistical area |
|||||
|
Atlanta, Georgia |
300 |
(90) |
190 |
(57) |
334 |
|
Baltimore, Maryland |
410 |
(90) |
264 |
(58) |
455 |
|
Boston, Massachusetts |
239 |
(95) |
162 |
(64) |
252 |
|
Chicago, Illinois |
472 |
(91) |
344 |
(67) |
516 |
|
Dallas, Texas |
369 |
(83) |
229 |
(52) |
444 |
|
Denver, Colorado |
417 |
(92) |
288 |
(64) |
452 |
|
Detroit, Michigan |
301 |
(83) |
212 |
(59) |
362 |
|
Houston, Texas |
326 |
(92) |
221 |
(62) |
355 |
|
Los Angeles, California |
442 |
(94) |
306 |
(65) |
469 |
|
Miami, Florida |
407 |
(89) |
272 |
(60) |
455 |
|
Nassau-Suffolk, New York |
225 |
(85) |
127 |
(48) |
264 |
|
New Orleans, Louisiana |
359 |
(91) |
244 |
(62) |
395 |
|
New York, New York |
420 |
(87) |
315 |
(65) |
483 |
|
Newark, New Jersey |
75 |
(87) |
58 |
(67) |
86 |
|
Philadelphia, Pennsylvania |
424 |
(78) |
324 |
(60) |
544 |
|
St. Louis, Missouri |
306 |
(92) |
200 |
(60) |
332 |
|
San Diego, California |
452 |
(95) |
339 |
(71) |
476 |
|
San Francisco, California |
379 |
(96) |
290 |
(73) |
395 |
|
San Juan, Puerto Rico |
299 |
(87) |
179 |
(52) |
343 |
|
Seattle, Washington |
291 |
(93) |
196 |
(62) |
314 |
|
Washington, DC |
427 |
(95) |
322 |
(72) |
449 |
|
Total |
7,340 |
(90) |
5,082 |
(62) |
8,175 |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † Proportion of participants who reported ever having been tested for HIV. § Proportion of participants who reported having been tested during the past 12 months. ¶ Persons of Hispanic/Latino ethnicity might be of any race. ** Other race; includes multiple races. †† GED diploma. §§ Coverage through private insurance policies or employer, TRICARE, CHAMPUS, or membership in a health maintenance organization. ¶¶ Coverage through Medicare, Medicaid, or Veterans Administration. *** Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. |
|||||
|
TABLE 11. (Continued) Number* and percentage of participants who reported each type of hepatitis vaccination, by selected demographic and other characteristics and metropolitan statistical area --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
|||||
|---|---|---|---|---|---|
|
Characteristic |
Hepatitis A† |
Hepatitis B§ |
Total |
||
|
No. |
(%) |
No. |
(%) |
||
|
Metropolitan statistical area |
|||||
|
Atlanta, Georgia |
174 |
(52) |
147 |
(44) |
334 |
|
Baltimore, Maryland |
137 |
(30) |
187 |
(41) |
455 |
|
Boston, Massachusetts |
119 |
(47) |
136 |
(54) |
252 |
|
Chicago, Illinois |
259 |
(50) |
269 |
(52) |
516 |
|
Dallas, Texas |
138 |
(31) |
156 |
(35) |
444 |
|
Denver, Colorado |
217 |
(48) |
249 |
(55) |
452 |
|
Detroit, Michigan |
124 |
(34) |
165 |
(46) |
362 |
|
Houston, Texas |
97 |
(27) |
115 |
(32) |
355 |
|
Los Angeles, California |
188 |
(40) |
206 |
(44) |
469 |
|
Miami, Florida |
145 |
(32) |
222 |
(49) |
455 |
|
Nassau-Suffolk, New York |
68 |
(26) |
81 |
(31) |
264 |
|
New Orleans, Louisiana |
172 |
(44) |
194 |
(49) |
395 |
|
New York, New York |
275 |
(57) |
281 |
(58) |
483 |
|
Newark, New Jersey |
46 |
(53) |
48 |
(56) |
86 |
|
Philadelphia, Pennsylvania |
154 |
(28) |
157 |
(29) |
544 |
|
St. Louis, Missouri |
164 |
(49) |
168 |
(51) |
332 |
|
San Diego, California |
288 |
(61) |
300 |
(63) |
476 |
|
San Francisco, California |
233 |
(59) |
250 |
(63) |
395 |
|
San Juan, Puerto Rico |
163 |
(48) |
193 |
(56) |
343 |
|
Seattle, Washington |
176 |
(56) |
200 |
(64) |
314 |
|
Washington, DC |
165 |
(37) |
194 |
(43) |
449 |
|
Total |
3,502 |
(43) |
3,918 |
(48) |
8,175 |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † Ever had at least one vaccination for hepatitis A. § Ever had at least one vaccination for hepatitis B. ¶ Persons of Hispanic/Latino ethnicity might be of any race. ** Other race; includes multiple races. †† GED diploma. §§ Coverage through private insurance policies or employer, TRICARE, CHAMPUS, or membership in a health maintenance organization. ¶¶ Coverage through Medicare, Medicaid, or Veterans Administration. *** Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. |
|||||
|
TABLE 12. (Continued) Number* and percentage of participants who reported syphilis testing† during the past 12 months, by selected demographic and other characteristics and metropolitan statistical area --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
|||
|---|---|---|---|
|
Characteristic |
No. |
(%) |
Total |
|
Metropolitan statistical area |
|||
|
Atlanta, Georgia |
23 |
(7) |
334 |
|
Baltimore, Maryland |
178 |
(39) |
455 |
|
Boston, Massachusetts |
97 |
(38) |
252 |
|
Chicago, Illinois |
215 |
(42) |
516 |
|
Dallas, Texas |
135 |
(30) |
444 |
|
Denver, Colorado |
161 |
(36) |
452 |
|
Detroit, Michigan |
125 |
(35) |
362 |
|
Houston, Texas |
136 |
(38) |
355 |
|
Los Angeles, California |
184 |
(39) |
469 |
|
Miami, Florida |
112 |
(25) |
455 |
|
Nassau-Suffolk, New York |
45 |
(17) |
264 |
|
New Orleans, Louisiana |
84 |
(21) |
395 |
|
New York, New York |
197 |
(41) |
483 |
|
Newark, New Jersey |
23 |
(27) |
86 |
|
Philadelphia, Pennsylvania |
112 |
(21) |
544 |
|
St. Louis, Missouri |
97 |
(29) |
332 |
|
San Diego, California |
169 |
(36) |
476 |
|
San Francisco, California |
201 |
(51) |
395 |
|
San Juan, Puerto Rico |
213 |
(62) |
343 |
|
Seattle, Washington |
147 |
(47) |
314 |
|
Washington, DC |
190 |
(42) |
449 |
|
Total |
2,844 |
(35) |
8,175 |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † Does not include 197 men who reported being diagnosed with syphilis during the past 12 months. § Persons of Hispanic/Latino ethnicity might be of any race. ¶ Other race; includes multiple races. ** GED diploma. †† Coverage through private insurance policies or employer, TRICARE, CHAMPUS, or membership in a health maintenance organization. §§ Coverage through Medicare, Medicaid, or Veterans Administration. ¶¶ Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. |
|||
|
TABLE 13. (Continued) Number* and percentage of participants who reported having used HIV prevention services or programs during past 12 months, by selected characteristics --- National HIV Behavioral Surveillance System: Men Who Have Sex with Men, 21 U.S. Cities, 2008 |
|||||||
|---|---|---|---|---|---|---|---|
|
Characteristic |
Intervention |
Total |
|||||
|
Individual† |
Group§ |
Either |
|||||
|
No. |
(%) |
No. |
(%) |
No. |
(%) |
||
|
Metropolitan statistical area |
|||||||
|
Atlanta, Georgia |
17 |
(5) |
15 |
(4) |
28 |
(8) |
334 |
|
Baltimore, Maryland |
89 |
(20) |
51 |
(11) |
113 |
(25) |
455 |
|
Boston, Massachusetts |
31 |
(12) |
21 |
(8) |
42 |
(17) |
252 |
|
Chicago, Illinois |
81 |
(16) |
38 |
(7) |
102 |
(20) |
516 |
|
Dallas, Texas |
38 |
(9) |
8 |
(2) |
42 |
(9) |
444 |
|
Denver, Colorado |
105 |
(23) |
42 |
(9) |
118 |
(26) |
452 |
|
Detroit, Michigan |
61 |
(17) |
37 |
(10) |
78 |
(22) |
362 |
|
Houston, Texas |
61 |
(17) |
16 |
(5) |
68 |
(19) |
355 |
|
Los Angeles, California |
54 |
(12) |
50 |
(11) |
88 |
(19) |
469 |
|
Miami, Florida |
52 |
(11) |
19 |
(4) |
60 |
(13) |
455 |
|
Nassau-Suffolk, New York |
32 |
(12) |
24 |
(9) |
51 |
(19) |
264 |
|
New Orleans, Louisiana |
61 |
(15) |
36 |
(9) |
77 |
(19) |
395 |
|
New York, New York |
69 |
(14) |
41 |
(8) |
93 |
(19) |
483 |
|
Newark, New Jersey |
23 |
(27) |
10 |
(12) |
24 |
(28) |
86 |
|
Philadelphia, Pennsylvania |
38 |
(7) |
20 |
(4) |
54 |
(10) |
544 |
|
St. Louis, Missouri |
36 |
(11) |
23 |
(7) |
48 |
(14) |
332 |
|
San Diego, California |
43 |
(9) |
21 |
(4) |
56 |
(12) |
476 |
|
San Francisco, California |
53 |
(13) |
30 |
(8) |
71 |
(18) |
395 |
|
San Juan, Puerto Rico |
75 |
(22) |
36 |
(10) |
94 |
(27) |
343 |
|
Seattle, Washington |
48 |
(15) |
15 |
(5) |
56 |
(18) |
314 |
|
Washington, DC |
47 |
(10) |
34 |
(8) |
73 |
(16) |
449 |
|
Total |
1,114 |
(14) |
587 |
(7) |
1,436 |
(18) |
8,175 |
|
Abbreviations: GED = general educational development; HIV = human immunodeficiency virus. * Numbers might not add to totals because of missing or unknown data. † One-on-one conversation with an outreach worker, a counselor, or a prevention program worker about ways to protect against HIV or other sexually transmitted diseases; excludes conversations that took place solely as a part of obtaining HIV testing (e.g., pretest or posttest counseling). § Small-group discussion about ways to protect against HIV or other sexually transmitted diseases. ¶ Suppressed because the number or numerator was less than 5. ** Persons of Hispanic/Latino ethnicity might be of any race. †† Other race; includes multiple races. §§ GED diploma. ¶¶ Coverage through private insurance policies or employer, TRICARE, CHAMPUS, or membership in a health maintenance organization. *** Coverage through Medicare, Medicaid, or Veterans Administration. ††† Annual household income was collected from participants in ranges. These ranges were combined into four categories (i.e., ≤$19,999, $20,000--$39,999, $40,000--$74,999, and ≥$75,000). Each category consisted of approximately one fourth of the total men surveyed. Income was not adjusted for household size because most of the participants had a household size of one. |
|||||||
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
References to non-CDC sites on the Internet are provided as a service to MMWR readers and do not constitute or imply endorsement of these organizations or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of pages found at these sites. URL addresses listed in MMWR were current as of the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.
