State and Territorial Ebola Screening, Monitoring, and Movement Policy Statements — United States, August 31, 2015
, JD1; , JD1; , MD2; , JD1
The 2014–2015 Ebola virus disease (Ebola) outbreak in West Africa is the largest in history, and as of October 4, 2015, had claimed 11,297 lives in Guinea, Liberia, and Sierra Leone (1). On August 7, 2014, CDC first posted guidance on monitoring and movement of persons who might have been exposed to Ebola virus to prevent the spread of Ebola into the United States. Since that time, the Interim U.S. Guidance for Monitoring and Movement of Persons with Potential Ebola Virus Exposure (2) has been regularly updated based on the latest information available, most recently on May 13, 2015. On October 11, 2014, after the first case of Ebola was diagnosed in the United States, entry screening was implemented in five U.S. airports to identify travelers from countries with widespread Ebola transmission who might have been exposed to Ebola during the days before arrival or who had signs or symptoms of Ebola at the time of arrival (3).
On October 24, 2014, New York and New Jersey, both home to airports conducting entry screening, announced monitoring and movement policies for incoming travelers returning from Ebola-affected countries (4). The New York and New Jersey policies included mandatory quarantine for any person who had direct contact with a person with Ebola while in one of the Ebola-affected countries, including any medical personnel who had provided medical services for persons infected with Ebola, as well as active monitoring and possible quarantine for all persons with travel history to the affected countries, including those who had no direct contact with an infected person (4).
On October 27, 2014, CDC guidance was updated by establishing a "low (but not zero) risk" category; adding a "no identifiable risk" category; modifying the recommended public health actions in the high, some, and low (but not zero) risk categories; and adding recommendations for specific groups and settings (2). Unlike the policies announced by New York and New Jersey, CDC guidance did not recommend mandatory quarantine. Instead, CDC guidance recommended active monitoring or direct active monitoring, and certain travel restrictions for symptomatic and some asymptomatic persons (2). Within a few months after issuance of the updated CDC guidance in October 2014, states began announcing state-specific monitoring and movement policies or amending existing policies. Some of these policies included stricter requirements than those recommended in CDC's guidance. Because of concerns about the potential impact of inconsistencies between state and federal monitoring and movement policies, CDC's Public Health Law Program* assessed jurisdictional differences in guidance by systematically reviewing and evaluating publically available official Ebola screening, monitoring, and movement policies for each state and territory. These policies included executive orders, health orders, press releases, informational websites, and frequently asked questions (FAQ) resources. Each published policy was compared with CDC guidance to determine whether it was more or less restrictive than CDC guidance, equivalent to CDC guidance, unclear, or if no policy was publically available. Only policies contained on official government websites were examined, and the implementation of policies was not assessed.
Policies that require more extensive movement restrictions or more frequent reporting were considered more restrictive than CDC guidance, as were those that would place the traveler into a higher risk category than would CDC guidance. Policies that mirror CDC recommendations, or those that state that the jurisdiction follows CDC guidance, with no further articulation as to how that state's monitoring and movement policies were being implemented, were considered equivalent to CDC guidance. Policies were considered less restrictive than CDC recommendations if they require asymptomatic persons to undergo public health actions that are less stringent than CDC's recommendations, such as permitting all travelers from Ebola-affected countries to return to work regardless of risk level. Policies were considered to be unclear if they were ambiguous regarding the categorization, monitoring, and movement of persons, including policies that state that movement restrictions would be implemented on a case-by-case basis, or that link to CDC guidance, without indicating whether the jurisdiction was following this guidance, or simply providing the resource for informational purposes. If no policy could be found on any publically available websites managed by government authorities, that state or territory was considered to have no published policy.
As of August 31, 2015, a total of 17 states and the District of Columbia had policies that were more restrictive than current CDC guidance, 35 states and territories had policies that were equivalent to CDC guidance, no states or territories had policies that were less restrictive than CDC guidance, one territory had an unclear policy, and two territories did not have a publicly available monitoring and movement policy (Figure).† The results were published online as the Interim Table of State Ebola Screening and Monitoring Policies for Asymptomatic Individuals (5). Although states have the prerogative to set their own public health policies under the police powers reserved to them by the 10th Amendment of the U.S. Constitution (6), the differences in policies have the potential to create confusion among members of the public, persons considering whether to join the response effort, and responders returning from West Africa (7). Confusion can be minimized when states make their policies clear and readily accessible to the public.
Acknowledgments
Office for State, Tribal, Local, and Territorial Support, Public Health Law Program, CDC; Office of the Associate Director for Policy, CDC; Deployment Risk Mitigation Unit, CDC; Global Migration Task Force, CDC; State Coordination Task Force, CDC; Joint Information Center, CDC; Office for State, Tribal, Local, and Territorial Support, Program Planning, and Communication Unit, CDC.
1Office for State, Tribal, Local, and Territorial Support, Public Health Law Program, CDC; 2Division of Global Migration and Quarantine, National Center for Emerging and Zoonotic Infectious Diseases, CDC.
Corresponding author: Gregory Sunshine, gsunshine@cdc.gov, 404-498-0457.
References
- CDC. 2014 Ebola outbreak in West Africa: case counts. Atlanta, GA: US Department of Health and Human Services, CDC; 2015. Available at http://www.cdc.gov/vhf/ebola/outbreaks/2014-west-africa/case-counts.html.
- CDC. Interim U.S. guidance for monitoring and movement of persons with potential Ebola virus exposure. Atlanta, GA: US Department of Health and Human Services, CDC; 2014. Available at http://www.cdc.gov/vhf/ebola/exposure/monitoring-and-movement-of-persons-with-exposure.html.
- Brown CM, Aranas AE, Benenson GA, et al. Airport exit and entry screening for Ebola—August–November 10, 2014. MMWR Morb Mortal Wkly Rep 2014;63:1163–7.
- Governor's Press Office (New York State). Governor Andrew Cuomo and Governor Chris Christie announce additional screening protocols for Ebola at JFK and Newark Liberty International airports. October 24, 2014. Available at https://www.governor.ny.gov/news/governor-andrew-cuomo-and-governor-chris-christie-announce-additional-screening-protocols-ebola.
- CDC. State Ebola protocols. Atlanta, GA: US Department of Health and Human Services, CDC; 2015. Available at http://www.cdc.gov/phlp/publications/topic/ebola.html.
- Jacobson v. Massachusetts, 197 U.S. 11 (1905). Available at http://caselaw.findlaw.com/us-supreme-court/197/11.html.
- Shah R. Combating Ebola in West Africa: the international response. Testimony before the House Committee on Foreign Affairs, 113th Congress, 2nd Session. November 13, 2014. Available at http://www.gpo.gov/fdsys/pkg/CHRG-113hhrg91450/html/CHRG-113hhrg91450.htm.
* CDC's Public Health Law Program works to advance the use of law as a public health tool through legal epidemiology and workforce development and by creating resources to improve understanding of law and policy decision-making for CDC programs and state, tribal, local, and territorial professionals.
† Additional information available at http://www.cdc.gov/phlp/docs/interim-ebolascreening.pdf.
FIGURE. Ebola screening and monitoring policies for asymptomatic persons, by restrictiveness relative to CDC policy — United States, August 31, 2015
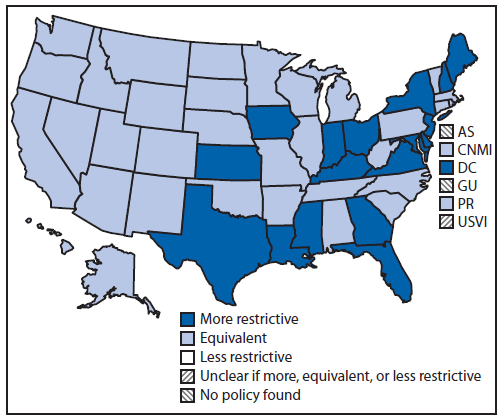
Abbreviations: AS = American Samoa; CNMI = Commonwealth of the Northern Mariana Islands; DC = District of Columbia; GU = Guam; PR = Puerto Rico; USVI = U.S. Virgin Islands.
Alternate Text: The figure above is a map of the United States showing Ebola screening and monitoring policies for asymptomatic persons, by restrictiveness relative to CDC policy, as of August 31, 2015.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
