Ebola Virus Disease in Health Care Workers — Guinea, 2014
Please note: An erratum has been published for this article. To view the erratum, please click here.
1; , MD2; , MD3; , MD4; , MD5; , PhD6; , DSc7; , MD8; , MD8; , PhD2
An outbreak of Ebola virus disease (Ebola) began in Guinea in December 2013 and has continued through September 2015 (1). Health care workers (HCWs) in West Africa are at high risk for Ebola infection owing to lack of appropriate triage procedures, insufficient equipment, and inadequate infection control practices (2,3). To characterize recent epidemiology of Ebola infections among HCWs in Guinea, national Viral Hemorrhagic Fever (VHF) surveillance data were analyzed for HCW cases reported during January 1–December 31, 2014. During 2014, a total of 162 (7.9%) of 2,210 laboratory-confirmed or probable Ebola cases among Guinean adults aged ≥15 years occurred among HCWs, resulting in an incidence of Ebola infection among HCWs 42.2 times higher than among non-HCWs. The disproportionate burden of Ebola infection among HCWs taxes an already stressed health infrastructure, underscoring the need for increased understanding of transmission among HCWs and improved infection prevention and control measures to prevent Ebola infection among HCWs.
Surveillance data from the national VHF database were analyzed for cases with a notification date in 2014. Using case definitions described previously (4), a standardized case investigation form was completed for every suspected, probable, or confirmed Ebola case that included age, sex, location of residence, occupation, symptom onset date, whether or not the patient was isolated in an Ebola treatment unit (ETU), and clinical outcome. Any person working in nonhousehold settings and who had contact with patients or patient waste was considered to be an HCW, including, but not limited to, doctors, nurses, midwives, hospital cleaners, ambulance drivers, laboratory workers, and ancillary health care staff. Traditional healers were not included. Only confirmed and probable Ebola cases in persons aged ≥15 years were included in the analysis. Incidence of Ebola infection was calculated using population denominators from the preliminary 2014 Guinea census and HCW denominators from the Guinea Ministry of Health (MOH) (5,6). Population denominators for persons aged ≥15 years were calculated assuming that 58% of the total population was aged ≥15 years (7). Outside of the capital Conakry, Guinea is divided into 33 administrative regions called prefectures. Geographic trends were analyzed by prefecture, with cases assigned to the location of the patient's permanent residence. Characteristics of HCW and non-HCW cases were compared using Chi-square tests; p-values <0.05 were considered statistically significant.
In 2014, a total of 162 (7.9%) of 2,210 laboratory-confirmed or probable Ebola cases reported from Guinea in persons aged ≥15 years occurred among HCWs. With an estimated 11,529 HCWs in Guinea and a national population of 6.15 million persons aged ≥15 years, the incidence of laboratory-confirmed or probable Ebola infections among HCWs in Guinea was 140.5 per 10,000 HCWs, compared with 3.3 per 10,000 non-HCWs aged ≥15 years (relative risk = 42.2; 95% confidence interval = 36.0–49.5).
Cases of Ebola infections among HCWs during this outbreak were first reported in January 2014 (2014 notification week 4). The highest number of Ebola case notifications in HCWs in Guinea in a single week occurred during week 51 with 15 cases (Figure 1). This also corresponded to the week with the highest number of total Ebola cases (HCW and non-HCW) in Guinea during 2014.
During 2014, Ebola cases among HCWs were reported in Conakry and 17 (52%) of the 33 prefectures in Guinea (Figure 2). HCW case counts were highest in Conakry (64 cases) and N'Zérékoré (17 cases). HCW cases made up the largest percentage of total cases in Dabola (33.3%), Yomou (20.0%), and Conakry (19.6%).
Among persons with confirmed and probable Ebola, HCWs were more likely to be male than non-HCWs (Table). The majority of Ebola cases among both HCWs and non-HCWs occurred among persons aged 15–49 years. The fatality rate was higher among non-HCWs. Among Ebola patients, non-HCWs were also more likely to be identified in the community after their death. Although HCWs with Ebola were more likely than non-HCW Ebola patients to be isolated in an ETU, the time between symptom onset and isolation was similar for HCWs (4.9 days) and non-HCWs (5.2 days); however, time from symptom onset until isolation was missing for 38% of non-HCWs and 20% of HCWs. Data on Ebola exposures were not complete for all Ebola patients; among Ebola patients with complete information, HCWs were significantly less likely to report attendance at a funeral than were non-HCWs and were also less likely to report any contact with a person known to have Ebola than were non-HCWs.
The most common occupations of HCWs with Ebola were doctor, nurse, and health technician (Table); these accounted for almost two thirds of occupations of HCWs with Ebola. Among Guinean HCWs, incidence of Ebola infection was highest among laboratory technicians (34.7 per 1,000) and doctors (26.6 per 1,000), followed by midwives (8.7 per 1,000) and nurses (5.5 per 1,000). Place of work was known for 114 (70%) HCWs with Ebola; among those, only one worked at an ETU.
Discussion
In 2014, Guinean HCWs had an incidence of Ebola infection 42.2 times higher than that of non-HCWs. Doctors and male HCWs were more affected than HCWs in other roles and female HCWs. Among Ebola cases, HCW patients were less likely than non-HCW patients to report risk factors such as funeral attendance or contact with a person know to have Ebola, although data completeness was poor for these measures.
Higher incidence of Ebola infection among HCWs than non-HCWs has also been reported in Sierra Leone and Liberia, two neighboring countries with intense Ebola transmission in 2014 (3). In Guinea, doctors represented the largest proportion of Ebola cases among HCWs, unlike Liberia, where nurses were the most affected group (8). In settings with an inadequate health infrastructure, high incidence of Ebola infection among HCWs not only limits the country's ability to respond to the Ebola outbreak, but also limits its baseline ability to address routine health care needs.
This evaluation found that 27% of Ebola infections among HCWs in Guinea occurred among doctors, who account for 14% of the health care workforce (5). Although no significant difference in infection rates among HCWs by sex has been reported from Sierra Leone or Liberia (3,8), male HCWs in Guinea appear to be at increased risk compared with female HCWs; in this evaluation, 75% of Ebola infections among HCWs occurred among males. Information on a subset of HCWs employed by the Guinea MOH indicates that males represent 46.4% of the overall health care workforce and 67.4% of doctors (Guinea MOH, unpublished data, September 2015). The male predominance in Ebola infections among HCWs in not completely explained by the predominance of doctors. When stratified by occupation, a majority of Ebola infections within each occupation except midwifery and nursing occurred among males. In this evaluation, 67% of Ebola infections among nondoctor HCWs occurred among males.
In response to Ebola infections among HCWs, the Guinea MOH is continuing to focus on HCW training and availability of personal protective equipment (PPE). Additionally, the Guinea MOH is focusing additional resources on investigating cases of Ebola among HCWs as sentinel public health events. Guinea's Ebola case investigation form lacks detailed questions needed to determine routes of transmission among HCWs. An HCW-focused survey tool with questions about specific job tasks, infection control training, use of PPE, and known Ebola exposures in the community, among patients or among fellow HCWs, was implemented in December 2014 and continues to be used to investigate HCW infections in Guinea. Subsequent analysis of these data might help inform the response to HCW infections by identifying infection prevention and control failures, training gaps, or specific HCW groups at higher risk for infection. Additionally, analysis of these data might help determine if HCWs are being infected in the health care setting or in the community.
The findings in this report are subject to at least two limitations. First, surveillance data on potential Ebola exposures were not consistently available. For example, data on funeral attendance or contact with a person known to have Ebola were missing for more than half of HCWs with Ebola and almost three quarters of non-HCWs with Ebola. More complete data collection could increase understanding of potential Ebola exposures. Second, no standard definition of an HCW exists. For Ebola surveillance purposes, a broader definition of HCW was used than was used in the MOH estimate of the number of HCWs, which likely resulted in an overestimate of the actual incidence of Ebola infection among HCWs.
Ebola infections among HCWs are an important focus area for the outbreak response, and an increased understanding of potential Ebola exposures is needed to better tailor infection prevention and control trainings and practices. The finding that HCWs were less likely than non-HCWs to report contact with a person known to have Ebola suggests a failure to identify Ebola cases in patients who present to non-ETU settings. The finding that only one infected HCW worked at an ETU underscores the importance of infection prevention and control. HCWs working in ETUs might have had more comprehensive infection prevention and control training, more access to infection prevention and control resources such as PPE, more practice donning and doffing PPE, and heightened awareness of Ebola compared with HCWs in non-ETU settings. Currently, substantial uncertainty exists about Ebola infections among HCWs, including source and place of exposure, reasons for delay in isolation after symptom onset, and particular job tasks that might increase the risk for infection. An enhanced understanding of HCW risks factors for infection, along with continuous infection prevention and control efforts, are necessary to prevent Ebola infection in this high-risk occupational group.
Acknowledgments
Ministry of Health, Guinea; World Health Organization; Médecins Sans Frontières; Guinea Ebola Response Team, CDC.
1Divsion of Population Health, National Center for Chronic Disease Prevention and Health Promotion, CDC; 2Division of Global HIV/AIDS, Center for Global Health, CDC; 3Division of STD Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC; 4Division of Global Health Protection, Center for Global Health, CDC; 5Guinea Ministry of Health and Public Hygiene; 6Division of Surveillance, Hazard Evaluations, and Field Studies, National Center for Occupational Safety and Health, CDC; 7Division of Parasitic Diseases and Malaria, Center for Global Health, CDC; 8World Health Organization, Conakry, Guinea.
Corresponding author: Margaret Grinnell, mhgrinnell@gmail.com.
References
- Briand S, Bertherat E, Cox P, et al. The international Ebola emergency. N Engl J Med 2014;371:1180–3.
- World Health Organization. Fact sheet no. 103: Ebola virus disease. Available at http://www.who.int/mediacentre/factsheets/fs103/en.
- Kilmarx PH, Clarke KR, Dietz PM, et al. Ebola virus disease in health care workers—Sierra Leone, 2014. MMWR Morb Mortal Wkly Rep 2014;63:1168–71.
- Dixon MG, Schafer IJ. Ebola viral disease outbreak—West Africa, 2014. MMWR Morb Mortal Wkly Rep 2014;63:548–51.
- Guinea Ministry of Planning. Publication of preliminary results of the Third General Census of Population and Housing conducted March 1–April 2, 2014 [French]. Conakry, Guinea: Guinea Ministry of Planning; 2014. Available at http://www.stat-guinee.org/index.php/result-prelim-rgph3?download=55:res-pre-rgph3.
- Guinea Division of Human Resources. Census of health workers 2009 [French]. Conakry, Guinea: Guinea Division of Human Resources; 2011.
- US Central Intelligence Agency. The world factbook: Guinea. Available at https://www.cia.gov/library/publications/the-world-factbook/geos/gv.html.
- Matanock A, Arwady MA, Ayscue P, et al. Ebola virus disease cases among health care workers not working in Ebola treatment units—Liberia, June–August, 2014. MMWR Morb Mortal Wkly Rep 2014;63:1077–81.
Summary
What is already known on this topic?
Health care workers (HCWs) are at high risk for infection in outbreaks of Ebola virus disease (Ebola). Ebola infections in HCW can be reduced through thorough appropriate triage and adherence to good infection prevention and control practices.
What is added by this report?
During 2014, a total of 162 (7.9%) of 2,210 laboratory-confirmed or probable Ebola cases among Guineans aged ≥15 years occurred among HCWs, resulting in a cumulative incidence of Ebola infection among HCWs 42.2 times higher than among non-HCWs. Doctors and male HCWs were disproportionally affected compared with HCWs in other roles and female HCWs.
What are the implications for public health practice?
Ebola infections among HCWs are an important focus area for Ebola outbreak response, and thorough investigation of cases in HCWs is important to better understand sources of exposure, reasons for delay in isolation once symptoms develop, particular job tasks that increase the risk for infection, and reasons that particular groups, such as males and doctors, are disproportionally affected. An increased understanding of HCW risks for infection along with continuous infection prevention and control efforts are necessary to prevent Ebola infection in this high-risk occupational group.
FIGURE 1. Number of confirmed and probable cases of Ebola virus disease per 10,000 persons among health care workers and non–health care workers aged ≥15 years, by notification week — Guinea, 2014
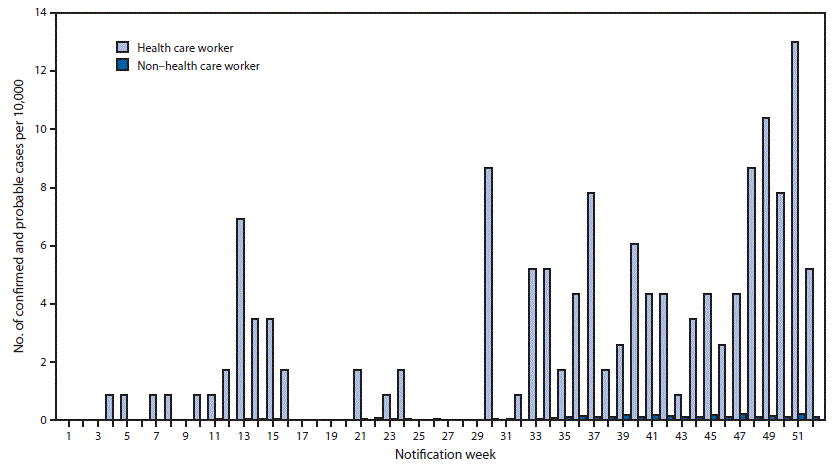
Alternate Text: The figure above is a bar chart showing the number of confirmed and probable cases of Ebola virus disease per 10,000 persons among health care workers and non-health care workers aged ≥15 years, by notification week, in Guinea during 2014.
FIGURE 2. Geographic distribution of confirmed and probable Ebola virus disease (Ebola) cases among health care workers aged ≥15 years — Guinea, 2014
Alternate Text: The figure above is a map showing geographic distribution of confirmed and probable Ebola virus disease cases among health care workers aged ≥15 years in Guinea during 2014.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
