Combustible and Smokeless Tobacco Use Among High School Athletes — United States, 2001–2013
, DMD1; , MD, PhD1,2; , PhD, JD3; , PhD1; , MBBS1; , PhD1; , PhD1
Athletes are not a typical at-risk group for smoking combustible tobacco products, because they are generally health conscious and desire to remain fit and optimize athletic performance (1). In contrast, smokeless tobacco use historically has been associated with certain sports, such as baseball (2). Athletes might be more likely to use certain tobacco products, such as smokeless tobacco, if they perceive them to be harmless (3); however, smokeless tobacco use is not safe and is associated with increased risk for pancreatic, esophageal, and oral cancers (4). Tobacco use among youth athletes is of particular concern, because most adult tobacco users first try tobacco before age 18 years (5). To examine prevalence and trends in current (≥1 day during the past 30 days) use of combustible tobacco (cigarettes, cigars) and smokeless tobacco (chewing tobacco, snuff, or dip [moist snuff]) products among athlete and nonathlete high school students, CDC analyzed data from the 2001–2013 National Youth Risk Behavior Surveys. Current use of any tobacco (combustible or smokeless tobacco) significantly declined from 33.9% in 2001 to 22.4% in 2013; however, current smokeless tobacco use significantly increased from 10.0% to 11.1% among athletes, and did not change (5.9%) among nonathletes. Furthermore, in 2013, compared with nonathletes, athletes had significantly higher odds of being current smokeless tobacco users (adjusted odds ratio [AOR] = 1.77, p<0.05), but significantly lower odds of being current combustible tobacco users (AOR = 0.80, p<0.05). These findings suggest that opportunities exist for development of stronger tobacco control and prevention measures targeting youth athletes regarding the health risks associated with all forms of tobacco use.
The national Youth Risk Behavior Survey is a biennial, school-based survey of U.S. high school students.* For each survey, a three-stage cluster sample design was used to produce a nationally representative sample of students in grades 9–12 who attend public and private schools. Students completed the self-administered questionnaire during one class period and recorded their responses directly on a computer scannable booklet or answer sheet. During 2001–2013, sample sizes ranged from 13,583 to 16,410; overall response rates ranged from 63% to 71%.
Current use of combustible tobacco products, smokeless tobacco products, and any tobacco product was self-reported.† Athletic status was assessed with the question, "During the past 12 months, on how many sports teams did you play? (Count any teams run by your school or community groups.)" Response options were "0 teams," "1 team," "2 teams," or "3 or more teams." Students who selected a response other than "0 teams" were categorized as athletes; all other responses were categorized as nonathletes.
Data were weighted to yield nationally representative estimates. Prevalence estimates were computed overall and by grade (9th, 10th, 11th, or 12th), sex (male or female), race/ethnicity (non-Hispanic white, non-Hispanic black, or Hispanic),§ and athletic status (athlete or nonathlete). Estimates were also computed on the basis of the number of sports teams on which students participated (0, 1, 2, ≥3). Estimates with relative standard errors >30% are not reported. Logistic regression models were fit, controlling for grade, sex, and race/ethnicity, to assess linear trends in tobacco use during 2001–2013, as well as measure the association between athletic status and tobacco use during each survey year.
Among U.S. high school students during 2001–2013, significant declines occurred in current use of any tobacco (33.9% to 22.4%) and combustible tobacco products (31.5% to 19.5%) (p<0.05 for linear trend); no significant change was observed in current smokeless tobacco use (Table). During the same period, significant declines in current use of any tobacco product occurred among all subgroups (sex, grade, race/ethnicity, and athletic status), with the exception of 11th grade athletes. Significant declines in current use of combustible tobacco occurred among all subgroups (sex, grade, race/ethnicity, and athletic status). Significant increases in current smokeless tobacco use were observed among 12th grade students and athletes overall. Among athletes, significant increases in current smokeless tobacco use were observed among both sexes, 11th- and 12th-grade students, and Hispanic students; among nonathletes, a significant increase was observed among Hispanic students only (p<0.05 for linear trends).
During 2013, the adjusted odds of current use of any tobacco, combustible tobacco, and smokeless tobacco were significantly higher among male students than female students, overall, and among athletes (p<0.05). Among nonathletes, the odds of current use of any tobacco and smokeless tobacco were significantly higher among male students, whereas no sex difference was observed for combustible tobacco use. Students in 9th and 10th grades had significantly lower odds of current use of any tobacco and combustible tobacco than 12th grade students, overall as well as among athletes and nonathletes; however, with the exception of 9th grade athletes, no significant grade differences existed for current use of smokeless tobacco. Students in 11th grade did not differ significantly in current use of any tobacco, combustible tobacco, or smokeless tobacco compared with 12th grade students, overall or among athletes or nonathletes. Overall and among both athletes and nonathletes, non-Hispanic black and Hispanic students had significantly lower odds of current use of any tobacco, combustible tobacco, and smokeless tobacco compared with non-Hispanic white students, with one exception: Hispanic athletes did not differ significantly from non-Hispanic white athletes in current use of combustible tobacco.
Athletes had significantly lower adjusted odds of current combustible tobacco use than nonathletes during 2001–2013; conversely, athletes had significantly higher adjusted odds of current smokeless tobacco use than nonathletes in 2001, 2005, 2011, and 2013 (p<0.05) (Figure 1). An inverse association between level of sports team participation and the prevalence of combustible tobacco use was identified; during 2013, prevalence of combustible tobacco use was 21.3%, 19.6%, 17.1%, and 15.8% among students participating in zero, one, two, or three or more sports teams, respectively (p<0.05) (Figure 2). In contrast, a positive association between the level of sports team participation and the prevalence of smokeless tobacco use was identified; during 2013, prevalence of smokeless tobacco use was 5.9%, 10.2%, 11.5%, and 12.5% among students participating in zero, one, two, or three or more sports teams, respectively (p<0.05).
Discussion
During 2001–2013, current use of smokeless tobacco increased significantly among high school athletes, but not among high school nonathletes; athletes reported higher use of smokeless tobacco, but lower use of combustible tobacco products than nonathletes. The lower use of combustible tobacco products among athletes might reflect an awareness of the adverse consequences of smoking on athletic performance, including reduced lung and cardiovascular function, reduced overall fitness, and poor wound healing (6). However, the higher smokeless tobacco use among athletes compared with nonathletes suggests athletes might perceive these products as being harmless, socially acceptable, or even a way to enhance athletic performance (3,7). Using smokeless tobacco products can adversely affect athletic performance and cause disease and premature death because they can contain nicotine, toxins, and carcinogens (4,6). For example, several professional U.S. athletes with a history of smokeless tobacco use have had a diagnosis of, or died from, oral cancer (8). Given that use of tobacco by youth in any form is unsafe, efforts are warranted to educate youth about the dangers of use of all forms of tobacco products, irrespective of whether they are combustible, noncombustible, or electronic (6).¶
The tobacco industry has marketed smokeless tobacco products as an alternative to cigarettes in situations where smoking is prohibited (9), which might further promote smokeless tobacco use among athletes. Although smokeless tobacco use is prohibited in minor league baseball, its use is restricted but not prohibited in major league baseball.** Smokeless tobacco use among professional athletes is an important issue because they often are considered role models by youth (5). On May 8, 2015, San Francisco, California, became the first U.S. city to pass a law prohibiting the use of smokeless tobacco at all baseball venues and athletic fields, effective January 1, 2016.†† The city of Boston, Massachusetts has also proposed an ordinance prohibiting smokeless tobacco use at all professional and amateur sports venues in Boston.§§ Implementing and enforcing tobacco-free policies that prohibit all tobacco use on school campuses and at all public recreational facilities, including stadiums, parks, and school gymnasiums, by players, coaches, referees, and fans might help reduce tobacco use among student athletes (5). In addition to tobacco-free policies, continued implementation of other population level, evidence-based interventions outlined in the CDC Best Practices for Comprehensive Tobacco Control Programs¶¶ is also critical to reducing all forms of tobacco use among youth; these interventions include increasing tobacco product prices, warning about the dangers of tobacco use, and increasing access to tobacco use cessation resources.
The differences in tobacco use among population subgroups (overall and among athletes), including the higher prevalence of both combustible tobacco and smokeless tobacco use among male students, non-Hispanic white students, and students in 11th and 12th grade, might be related to dissimilarities among these groups in socialization with tobacco-using peers, exposure and receptivity to pro-tobacco advertising, and targeted marketing of tobacco products by the tobacco industry (5).
The findings in this report are subject to at least six limitations. First, sports team participation and tobacco use were self-reported and might be subject to misreporting of tobacco use, which could lead to under- or overestimating tobacco use, as well as misclassification of athlete status (e.g., respondents who engaged fitness activities, but did not play on a school or community team would have been classified as nonathletes). Second, the prevalence of tobacco use among athletes and nonathletes might be underestimated since emerging smokeless tobacco products (e.g., snus [a smokeless tobacco product developed in Sweden], electronic cigarettes, hookah, and dissolvable tobacco) were not assessed. Third, differential time frames in assessing current tobacco use (past 30 days) and sports team participation (past 12 months) might miss seasonal patterns of tobacco use (e.g., tobacco use patterns during a sports season might differ from off-season use among athletes). Fourth, tobacco use by type of sport could not be assessed, because these data were not collected. Fifth, although the data were weighted to adjust for school and student nonresponse and the distribution of students by grade, sex, and race/ethnicity in each jurisdiction, nonresponse bias is possible and might have affected the results. Finally, these data apply only to youth who attend school and are not representative of all youth, including those who are homeschooled or who have dropped out of school nationwide. However, in 2013, 96.1% of U.S. youth aged 14–17 years were enrolled in traditional schools (10); thus, the extent of any bias from this exclusion is likely minimal.
Sports activities present opportunities to reach young persons with public health interventions.*** Tobacco education programs tailored to high school athletes, coupled with other population-level evidence-based interventions, have the potential to increase awareness of the dangers of tobacco use and to reduce the use of all forms of tobacco, including smokeless tobacco, among youth.
1Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC; 2Epidemic Intelligence Service, CDC; 3Division of Adolescent and School Health, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, CDC.
Corresponding author: Israel Agaku, IAgaku@cdc.gov, 770-488-5138.
References
- Terry-McElrath YM, O'Malley PM, Johnston LD. Exercise and substance use among American youth, 1991–2009. Am J Prev Med 2011;40:530–40.
- Severson HH, Klein K, Lichtensein E, Kaufman N, Orleans CT. Smokeless tobacco use among professional baseball players: survey results, 1998 to 2003. Tob Control 2005;14:31–6.
- Walsh MM, Ellison J, Hilton JF, Chesney M, Ernster VL. Spit (smokeless) tobacco use by high school baseball athletes in California. Tob Control 2000;9(Suppl 2):II32–9.
- International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans: personal habits and indoor combustions. Vol. 100E. Lyon, France: International Agency for Research on Cancer, World Health Organization; 2012. Available at http://monographs.iarc.fr/ENG/Monographs/vol100E/index.php.
- US Department of Health and Human Services. Preventing tobacco use among youth and young adults: a report of the surgeon general. Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2012.
- US Department of Health and Human Services. The health consequences of smoking: 50 years of progress: a report of the surgeon general. Atlanta, GA: US Department of Health and Human Services, CDC; 2014. Available at http://www.surgeongeneral.gov/library/reports/50-years-of-progress.
- Myers KA. Cigarette smoking: an underused tool in high-performance endurance training. CMAJ 2010;182:E867–9.
- The Oral Cancer Foundation. Sports figures. Newport Beach, CA: The Oral Cancer Foundation; 2014. Available at http://www.oralcancerfoundation.org/people/sports-figures.php.
- Carpenter CM, Connolly GN, Ayo-Yusuf OA, Wayne GF. Developing smokeless tobacco products for smokers: an examination of tobacco industry documents. Tob Control 2009;18:54–9.
- US Census Bureau. School enrollment: current population survey 2013 [detailed tables]. Washington, DC: US Census Bureau. Available at https://www.census.gov/hhes/school/data/cps/2013/tables.html.
* The national Youth Risk Behavior Survey (YRBS), conducted by CDC, is part of a larger school-based surveillance system, the Youth Risk Behavior Surveillance System (YRBSS). In addition to the national YRBS, the YRBSS includes other state, territorial, tribal government, and local surveys, conducted by departments of health and education, which provide data representative of mostly public high school students in each jurisdiction. Available at http://www.cdc.gov/yrbss.
† To ascertain past 30-day use of cigarettes, cigars, and smokeless tobacco, respondents were asked the following questions: 1) "During the past 30 days, on how many days did you smoke cigarettes?"; 2) "During the past 30 days, on how many days did you smoke cigars, cigarillos, or little cigars?"; and 3) "During the past 30 days, on how many days did you use chewing tobacco, snuff, or dip, such as Redman, Levi Garrett, Beechnut, Skoal, Skoal Bandits, or Copenhagen?" Categorical response options to all three questions were "0 days," "1 or 2 days," "3 to 5 days," "6 to 9 days," "10 to 19 days," "20 to 29 days," or "all 30 days." Students who provided a response other than "0 days" were categorized as current users of each respective product.
§ Data are presented only for non-Hispanic white, non-Hispanic black, and Hispanic students because sample sizes for other race/ethnic groups were too small to provide statistically reliable estimates.
¶ Additional information available at http://cancercontrol.cancer.gov/brp/tcrb/global-perspective/index.html.
** Additional information available at http://mlb.mlb.com/mlb/downloads/2011_CBA.pdf.
†† Additional information available at https://www.tobaccofreekids.org/press_releases/post/2015_05_08_baseball.
§§ Additional information available at http://tobaccofreebaseball.org/content/press-release-08_05_15/.
¶¶ Additional information available at http://www.cdc.gov/tobacco/stateandcommunity/best_practices/pdfs/2014/comprehensive.pdf.
*** Additional information available at http://www.cdc.gov/tobacco/youth/sports.
Summary
What is already known on this topic?
Athletes might be more likely to use certain tobacco products, such as smokeless tobacco, if they perceive them to be harmless; however, smokeless tobacco use is not safe, and is associated with increased risk for oral, esophageal, and pancreatic cancers.
What is added by this report?
Data from national Youth Risk Behavior Surveys indicate that current (≥1 day during the past 30 days) use of any tobacco product by U.S. high school students declined from 33.9% in 2001 to 22.4% in 2013; however, current smokeless tobacco use increased from 10.0% to 11.1% among high school athletes. Compared with nonathletes, athletes had higher odds of being current smokeless tobacco users, but lower odds of being current combustible tobacco users.
What are the implications for public health?
Tobacco education programs tailored to high school athletes, coupled with other population-level, evidence-based interventions, have the potential to increase awareness of the harmfulness of all tobacco products and reduce all forms of tobacco use, including smokeless tobacco, among youth.
FIGURE 1. Adjusted odds ratios,* with 95% confidence intervals, for current use of combustible† and smokeless§ tobacco products among high school athletes¶ compared with nonathletes — Youth Risk Behavior Surveys, United States, 2001–2013
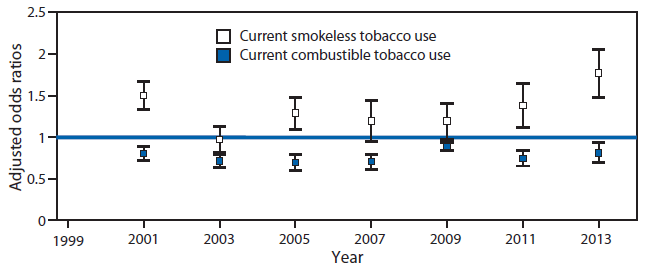
* Adjusted for grade, sex, and race/ethnicity in a binary logistic regression model. Adjusted odds ratios are for athletes, using nonathletes as the reference category.
† Current combustible tobacco use was defined as having smoked cigarettes or cigars, cigarillos, or little cigars on ≥1 day during the 30 days before the survey.
§ Current smokeless tobacco use was defined as having used chewing tobacco, snuff, or dip on ≥1 day during the 30 days before the survey.
¶ Athletes were defined as students who played on at least one sports team, run by their school or community groups, during the 12 months before the survey. Nonathletes were students who did not play on a sports team during the 12 months before the survey.
Alternate Text: The figure above is a bar chart showing adjusted odds ratios, with 95% confidence intervals, for current use of combustible and smokeless tobacco products among high school athletes compared with nonathletes in United States during 2001-2013.
FIGURE 2. Percentage of high school students who reported current use of combustible tobacco* and smokeless tobacco,† by extent of sport team participation§ — Youth Risk Behavior Surveys, United States, 2001–2013
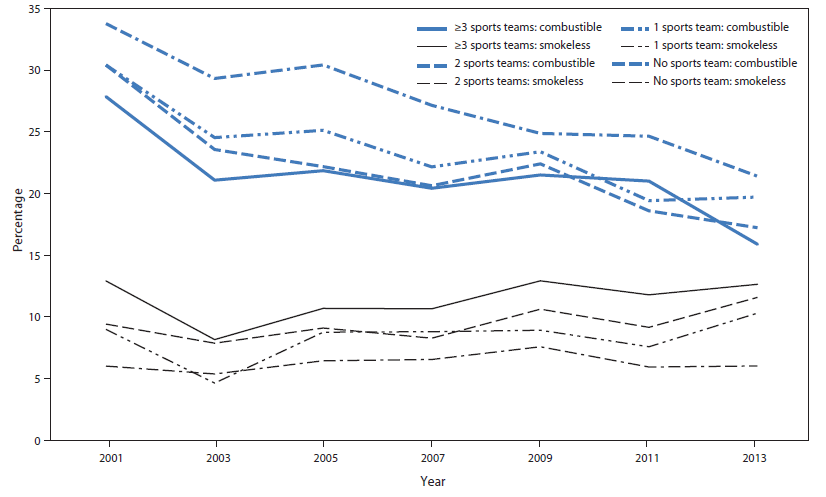
* Current combustible tobacco use was defined as having smoked cigarettes or cigars, cigarillos, or little cigars on ≥1 day during the 30 days before the survey.
† Current smokeless tobacco use was defined as have used chewing tobacco, snuff, or dip on ≥1 day during the 30 days before the survey.
§ Extent of sport participation was defined with the question "During the past 12 months, on how many sports teams did you play? (Count any teams run by your school or community groups.)" Response options were "0 teams," "1 team," "2 teams," or "3 or more teams."
Alternate Text: The figure above is a line chart showing the percentage of high school students who reported current use of combustible tobacco and smokeless tobacco, by extent of sports team participation in the United States during 2001-2013.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
