World Health Organization Guidelines for Containment of Poliovirus Following Type-Specific Polio Eradication — Worldwide, 2015
, PhD1; , MD1; 1; , MD1
In 1988, the World Health Assembly of the World Health Organization (WHO) resolved to eradicate polio worldwide. Among the three wild poliovirus (WPV) types (type 1, type 2, and type 3), WPV type 2 (WPV2) has been eliminated in the wild since 1999, and WPV type 3 (WPV3) has not been reported since 2012. In 2015, only Afghanistan and Pakistan have reported WPV transmission (1). On May 25, 2015, all WHO Member States endorsed World Health Assembly resolution 68.3 on full implementation of the Polio Eradication and Endgame Strategic Plan 2013–2018 (2,3) (the Endgame Plan), and with it, the third Global Action Plan to minimize poliovirus facility-associated risk (4) (GAPIII). All WHO Member States have committed to implementing appropriate containment of WPV2 in essential laboratory and vaccine production facilities* by the end of 2015 and of type 2 oral poliovirus vaccine (OPV2) within 3 months of global withdrawal of OPV2, which is planned for April 2016 (5). This report summarizes critical steps for essential laboratory and vaccine production facilities that intend to retain materials confirmed to contain or potentially containing type-specific WPV, vaccine-derived poliovirus (VDPV), or OPV/Sabin viruses, and steps for nonessential facilities† that process specimens that contain or might contain polioviruses. National authorities will need to certify that the essential facilities they host meet the containment requirements described in GAPIII. After certification of WPV eradication, the use of all OPV will cease; final containment of all polioviruses after polio eradication and OPV cessation will minimize the risk for reintroduction of poliovirus into a polio-free world.
Background
The Endgame Plan (3) set the goal of eradicating WPV and VDPV. Achieving this goal requires 1) detection of circulating polioviruses and interruption of transmission; 2) sequential cessation of the use of type-specific OPV to eliminate the risks for vaccine-associated paralytic poliomyelitis, chronic VDPV infections of immunodeficient persons, and outbreaks of circulating VDPV (cVDPV) (6,7); and 3) implementation of measures for the safe handling and containment of polioviruses to minimize the risks for facility-associated reintroduction of virus into polio-free communities. The first step toward OPV cessation will be the global, synchronized withdrawal of OPV2, which has caused approximately 90% of cVDPV cases since WPV2 was last reported in 1999. OPV2 withdrawal will be accomplished by replacing trivalent OPV (tOPV) with bivalent OPV (bOPV, protecting against types 1 and 3 in all countries using OPV for routine immunization, preceded by the introduction of a minimum of 1 dose of inactivated poliovirus vaccine (IPV), which protects against all three virus types (5). Approval to confirm the global switch from tOPV to bOPV, anticipated in April 2016, will follow review in October 2015 of whether a number of readiness criteria are met, including progress toward completion of the initial phase of poliovirus containment activities and establishment of readiness for appropriate handling of residual type 2 materials, as described below.
Methods
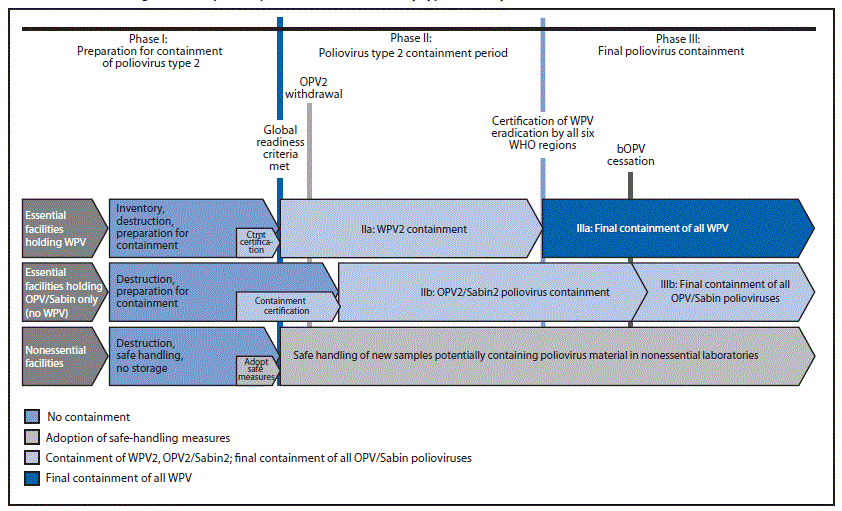
The Endgame Plan includes phased withdrawal of OPV strains. GAPIII was aligned to the Endgame Plan and comprises three phases (Figure): Phase I, Preparation for containment of poliovirus type 2, lasting until global readiness criteria for the switch are met (current target is end of 2015); Phase II, Poliovirus type 2 containment, lasting until all WHO regions certify WPV elimination; and Phase III, Final poliovirus containment. National authorities in all countries are currently tasked with completing Phase I and preparing for Phase II (Table 1).
The controls described in GAPIII reflect containment best practices, and are largely derived from the European Committee for Standardization Workshop Agreement 15793 (2011) — Laboratory Biorisk Management (8), with input from leaders in the field of poliovirus transmission and biorisk management.
Rationale
Reintroduction of WPV from a poliovirus facility after type-specific eradication risks the potentially disastrous consequence of reestablishing WPV transmission. When OPV use stops, many countries will maintain high population coverage with IPV, other countries will have suboptimal IPV coverage, and still others might discontinue use of IPV and all national polio immunization activities. Reintroduction of an OPV/Sabin strain from a facility creates risks for unrecognized virus transmission, reversion to cVDPV, and reestablishment of poliovirus transmission.
Most countries will have no need to retain polioviruses following WPV eradication and cessation of OPV use. Facility-associated risks in these countries can be eliminated by a thorough nationwide search for, and destruction of, all infectious and potentially infectious materials, including WPV, VDPV, and OPV/Sabin viruses. Some countries will host a limited number of essential laboratory and vaccine production facilities that serve critical program and research functions, including production of IPV and Sabin-IPV (IPV produced using attenuated strains from the Sabin oral vaccine as seed), production and storage of monovalent OPV stockpiles of each type, vaccine quality assurance, diagnostic reagent production, and crucial research. Each essential poliovirus facility should manage biorisk appropriately to minimize the risk for virus reintroduction into the community, with effective national certification and WHO verification programs to assure compliance with GAPIII. The risk for a poliovirus reintroduction can further be minimized by ensuring that essential facilities are located in areas with high levels of population immunity and acute flaccid paralysis and environmental surveillance, supplemented by efficient public health and response capacity (Table 2). Minimizing the number of essential facilities worldwide will further reduce the magnitude of risk, facilitate national and international oversight, and strengthen the likelihood that global containment standards can be met and successfully maintained.
Policy and Implementation
Phase I: Preparation for containment of all type 2 polioviruses. Phase I is currently in progress. Phase I for WPV2 will continue until the conditions of global readiness for OPV2 withdrawal have been met (Table 1), which include elimination of persistent cVDPV2 and certification of WPV2 eradication, currently planned for review in October 2015. Phase I for OPV2/Sabin2 will continue until 3 months after the switch from tOPV to bOPV. Surveyed national laboratories should include 1) all public or private facilities working with WPV2/VDPV2 and all facilities working with OPV2/Sabin2 or with fecal or respiratory materials that could contain WPV2, VDPV2, or OPV2/Sabin2 (collected at a time and place when OPV was in use), and 2) all public or private facilities that might have collections of infectious or potentially infectious WPV2, VDPV2 or OPV2/Sabin2 materials of any origin that are maintained for any reason.
Facilities that retain specimens that might contain WPV2/VDPV2 viruses must destroy or contain such materials before Phase IIa can begin. Facilities that wish to retain specimens that might contain OPV2/Sabin2 viruses (i.e., fecal or respiratory samples collected in places when OPV was in use) must destroy or contain such materials before commencement of Phase IIb. Laboratories wishing to retain historic collections of clinical materials potentially containing polioviruses, but that are not planning to implement the poliovirus containment measures described in GAPIII, must explore transfer options with designated certified essential poliovirus facilities for handling and storage arrangements.
Phase II: Poliovirus type 2 containment period. Phase II begins as soon as the criteria for global readiness for OPV2 withdrawal are met (5) and is currently planned for January 2016 (Table 1). This phase comprises two parts: the first (Phase IIa) addresses the containment of WPV2, and the second (Phase IIb) the containment of OPV2/Sabin2 polioviruses in certified essential facilities. Phase IIa begins after elimination of persistent cVDPV2 and certification of WPV2 eradication, at the time of global readiness for OPV2 withdrawal, and ends after all six WHO regions have certified WPV eradication. Phase IIb begins within 3 months of withdrawal of tOPV and the switch to bOPV, and ends within 3 months after global bOPV cessation. Essential poliovirus facilities handling and storing WPV2 or OPV2/Sabin2 materials in Phase II must be certified to implement containment procedures, and be regularly reassessed against WPV2 containment provisions described in GAPIII, including primary and secondary safeguards (Table 2). Once Phase II begins, facilities that have not received national certification for WPV2 containment will no longer be permitted to handle and store WPV2 materials. Countries or concerned facilities may apply to WHO through their national authorities for verification of containment in essential poliovirus facilities, certified by the ministries of health or other designated national authority, and declared to meet all biorisk management criteria consistent with GAPIII.
Phase III: Final poliovirus containment. Phase III also has two parts (Phases IIIa and IIIb). Phase IIIa (final containment of all WPV after polio eradication) begins when all six WHO regions have completed the certification of WPV eradication, at least 3 years after the last isolation of WPV (Table 1). Certified essential laboratories and IPV production facilities handling and storing any WPV or VDPV materials must implement final containment of all WPV provisions, including primary, secondary, and tertiary safeguards (Table 2). Once Phase III begins, facilities that have not received national certification for final containment of all WPV will no longer be permitted to handle and store any WPV materials. At the time of global bOPV cessation (currently planned for 1 year after the global declaration of WPV eradication), all countries must recall and destroy bOPV stocks. WHO will provide specific implementation guidelines for collection and destruction of bOPV from designated collection points, health facilities, or private practitioners, and national and subnational storage facilities (9).
Phase IIIb (final containment of all OPV poliovirus after bOPV cessation) will begin 3 months after global bOPV cessation (Figure) (Table 1). Certified essential poliovirus laboratories and Sabin-IPV vaccine production facilities handling and storing OPV/Sabin materials (but no WPV) must implement final provisions for containment of all OPV/Sabin polioviruses, including primary and secondary safeguards (Table 2). Once Phase IIIb begins, facilities that have not received national certification for final containment of all OPV/Sabin polioviruses will no longer be permitted to handle and store OPV/Sabin materials. Within 6 months of bOPV cessation, all countries must submit documentation that requirements for final containment of all OPV/Sabin polioviruses have been met.
Discussion
An estimated 500 facilities worldwide are currently holding type 2 polioviruses. One of the goals of poliovirus containment is to reduce this number substantially (10), dissuading candidate facilities not meeting the GAPIII containment criteria for essential facilities from holding any polioviruses.
It is important to note that poliovirus diagnostic laboratories will continue to be critical for surveillance and will remain so for years to come. Poliovirus diagnostic laboratories are not required to become certified essential poliovirus facilities to continue to perform their jobs, as long as they do not retain live polioviruses. However, laboratories that perform reference (and diagnostic) functions need to retain live polioviruses and thus be certified to meet the criteria for essential poliovirus facilities. Only designated essential poliovirus facilities that are certified to meet GAPIII containment requirements will handle and store polioviruses.
The timeline presented in GAPIII for the type-specific containment of polioviruses is short, both for candidate essential poliovirus facilities to be assessed and certified to meet GAPIII requirements, and for national authorities responsible for containment to deliver containment certificates. However, continuation of polio vaccine production, surveillance, and research is critical and must continue. To help manage the practical challenges associated with implementation of containment for essential laboratory and vaccine production facilities, interim certification of containment has been proposed. Interim certification would allow containment certification to proceed during the endgame phases of eradication in a controlled and structured manner, as issues associated with meeting the requirements for full containment certificates are addressed within pressing timelines. The proposed mechanisms will provide some degree of flexibility as facilities make the required changes, and national authorities and other governing bodies develop the required capacity to implement certification requirements.
The final containment of all WPV/VDPVs, including types 1 and 3, is approaching. After WPV transmission has been stopped, final containment of all polioviruses will minimize the risk for poliovirus reintroduction into a polio-free world once all OPV use is phased out. As is the case with variola virus, containment requirements will have to be regularly assessed and maintained, until a global decision is made to destroy all remaining poliovirus materials and prohibit any de novo synthesis.
1Polio Eradication Department, World Health Organization.
Corresponding author: Nicoletta Previsani, PhD, previsanin@who.int, 41-22-791-2866.
References
- Hagan JE, Wassilak SGF, Craig AS, et al. Progress toward polio eradication—worldwide, 2014–2015. MMWR Morb Mortal Wkly Rep 2015;64:527–31.
- World Health Organization. Poliomyelitis. Geneva, Switzerland: Sixty-eighth World Health Assembly Resolution WHA68.3, May 26, 2015. Available at http://apps.who.int/gb/ebwha/pdf_files/WHA68/A68_R3-en.pdf.
- Global Polio Eradication Initiative. Polio Eradication and Endgame Strategic Plan 2013–2018. Geneva, Switzerland: Global Polio Eradication Initiative; 2013. Available at http://www.polioeradication.org/portals/0/document/resources/strategywork/endgamestratplan_20130414_eng.pdf.
- World Health Organization. GAPIII: WHO global action plan to minimize poliovirus facility-associated risk. Geneva, Switzerland: World Health Organization; 2014. Available at http://www.polioeradication.org/Portals/0/Document/Resources/PostEradication/GAPIII_2014.pdf.
- Immunization Systems Management Group of the Global Polio Eradication Initiative. Introduction of inactivated poliovirus vaccine and switch from trivalent to bivalent oral poliovirus vaccine—worldwide, 2013–2016. MMWR Morb Mortal Wkly Rep 2015;64:699–702.
- Platt LR, Estívariz CF, Sutter RW. Vaccine-associated paralytic poliomyelitis: a review of the epidemiology and estimation of the global burden. J Infect Dis 2014;210(Suppl 1):S380–9.
- Diop OM, Burns CC, Sutter RW, Wassilak SG, Kew OM. Update on vaccine-derived polioviruses—worldwide, January 2014–March 2015. MMWR Morb Mortal Wkly Rep 2015;64:640–6.
- European Committee for Standardization. Laboratory biorisk management. CEN Workshop Agreement 15793:2011, September 2011. Available at http://www.uab.cat/doc/CWA15793_2011.
- World Health Organization. The switch from tOPV to bOPV Implementation guidelines. Geneva, Switzerland: World Health Organization; 2014. Available at http://www.who.int/immunization/diseases/poliomyelitis/endgame_objective2/oral_polio_vaccine/switch_guidelines-april2015.pdf?ua=1.
- Dowdle W, van der Avoort H, de Gourville E, et al. Containment of polioviruses after eradication and OPV cessation: characterizing risks to improve management. Risk Anal 2006;26:1449–69.
* A facility designated by the ministry of health or other designated national body or authority as serving critical national or international functions that involve handling and storage of needed poliovirus infectious materials or potentially infectious materials under conditions set out in GAPIII.
† Any facility that is likely to investigate new WPV2, type 2 attenuated vaccine-derived poliovirus (aVDPV2), type 2 circulating vaccine-derived poliovirus (cVDPV2), or inactivated type 2 vaccine-derived poliovirus (VDPV2) isolates, or new fecal or respiratory samples originating from recent OPV-using countries, and adopts and implements 1) safe and secure working practices based on a risk assessment and the implementation of appropriate biorisk management systems as described in GAPIII, 2) a nonretention policy for WPV2 materials as of the beginning of Phase IIa of the poliovirus type 2 containment period, and 3) a nonretention policy for OPV2/Sabin2 materials as of the beginning of Phase IIb of the poliovirus type 2 containment period.
|
TABLE 1. Phased implementation of poliovirus containment activities in the third Global Action Plan (GAPIII)* to minimize poliovirus facility-associated risk, worldwide |
|||
|---|---|---|---|
|
Prerequisites |
Begins |
Target for completion |
Key activities |
|
Phase I: Preparation for containment of PV type 2 |
|||
|
None |
Ongoing |
For WPV2: global readiness for OPV2 withdrawal (target for global readiness review is October 2015) For OPV2/Sabin2: 3 months after the withdrawal of tOPV |
• Governments, institutions, and laboratory and vaccine production facilities informed about the upcoming need for type-specific poliovirus containment • Inventory and survey of laboratory facilities and vaccine production facilities handling or storing infectious or potentially infectious poliovirus materials Essential facilities†: • National certification of WPV2-holding laboratories and IPV production facilities Nonessential facilities§: • Destruction of unneeded PV material • Transfer of needed PV type 2 material to essential laboratory facilities • If specimen investigations continue, adoption of nonretention policy for new WPV2 isolates, to be implemented in Phase IIa |
|
Phase IIa: WPV2 containment |
|||
|
Elimination of circulating WPV2 Elimination of persistent cVDPV2 |
As soon as the criteria for global readiness for OPV2 withdrawal are met (target is January 2016) |
After all six WHO Regions have certified WPV eradication |
Essential facilities†: • Handle and store WPV2 materials in "Containment of WPV2" conditions outlined in GAPIII Nonessential facilities§: • Destroy remaining unneeded OPV2 material • Transfer needed OPV2 material to certified essential laboratory facilities Nonessential facilities that continue specimen investigations¶: • Implement nonretention policy • Destroy unneeded recently isolated PV material • Transfer needed recently isolated PV material to certified essential facilities |
|
Phase IIb: OPV/Sabin PV type 2 (OPV2/Sabin2) containment |
|||
|
Licensed, available bOPV (types 1 and 3) Global IPV introduction Global tOPV-bOPV switch |
Within 3 months of global tOPV to bOPV switch (target for global switch is April 2016) |
Within 3 months of global bOPV cessation (planned 1 year after global certification of WPV eradication) |
Essential facilities†: • Handle and store OPV materials in "Containment of OPV2/Sabin2 polioviruses" conditions outlined in GAPIII |
|
Phase IIIa: Final containment of all WPV after polio eradication |
|||
|
3 years pass without isolation of WPV |
As soon as all six WHO Regions certify WPV eradication |
Long-term eradication (beyond global bOPV cessation) |
Essential facilities†: • Handle and store all WPV materials in "Final containment of all WPV" conditions, as outlined in GAPIII |
|
Phase IIIb: Final biocontainment of all OPV/Sabin PV after bOPV cessation |
|||
|
Global bOPV cessation |
Within 3 months of global bOPV cessation (planned 1 year after global certification of WPV eradication) |
Long-term eradication (beyond global bOPV cessation) |
Essential facilities†: • Handle and store OPV materials in "Final containment of all OPV/Sabin polioviruses" conditions, as outlined in GAPIII |
|
Abbreviations: bOPV = bivalent oral polio vaccine (types 1 and 3); cVDPV2 = type 2 circulating vaccine-derived poliovirus; GAPIII = third Global Action Plan to minimize poliovirus facility-associated risk; IPV = inactivated poliovirus vaccine; OPV = oral poliovirus vaccine; OPV2 = type 2 OPV; PV = poliovirus; tOPV = trivalent OPV (types 1, 2 and 3); WHO = World Health Organization; WPV = wild poliovirus; WPV2 = type 2 WPV. * Available at http://www.polioeradication.org/Portals/0/Document/Resources/PostEradication/GAPIII_2014.pdf. † A facility designated by the ministry of health or other designated national body or authority as serving critical national or international functions that involve handling and storage of needed poliovirus infectious materials or potentially infectious materials under conditions set out in GAPIII. § Any facility that is likely to investigate new WPV2, aVDPV2, cVDPV2 or iVDPV2 isolates, or new fecal or respiratory samples originating from recent OPV-using countries, and adopts and implements a) safe and secure working practices based on a risk assessment and the implementation of appropriate biorisk management systems as described in GAPIII, b) a nonretention policy for WPV2 materials as of the beginning of Phase IIa of the poliovirus type 2 containment period, and c) a nonretention policy for OPV2/Sabin2 materials as of the beginning of Phase IIb of the poliovirus type 2 containment period. ¶ All nonessential laboratories investigating new WPV2; aVDPV2, cVDPV2, or iVDPV2 isolates, or new fecal and respiratory samples originating from recent OPV-using countries. |
|||
|
TABLE 2. Containment safeguards to minimize poliovirus facility-associated risks after type-specific eradication of wild polioviruses and sequential cessation of oral polio vaccine use, worldwide |
|||
|---|---|---|---|
|
Safeguards |
Poliovirus type 2 biocontainment (phases IIa and IIb) |
Final poliovirus biocontainment |
|
|
All type 2 polioviruses |
All OPV/Sabin polioviruses |
All wild polioviruses |
|
|
Primary safeguards: prevention of infection with and release of contaminated materials |
|||
|
Operator protection* |
Yes |
Yes |
Yes |
|
Decontamination of materials/equipment |
Yes |
Yes |
Yes |
|
Dedicated effluent treatment plant |
No† |
No† |
Yes§ |
|
Air/exhaust treatment |
No |
No |
Yes¶ |
|
Secondary safeguards: population immunity in country hosting facility |
|||
|
Number of IPV doses |
≥1 |
≥1 |
≥3 |
|
IPV coverage |
= DTP3 coverage** |
= DTP3 coverage** |
>90% |
|
Tertiary safeguards: environment and location |
|||
|
Situating facilities in areas with low transmission potential for wild polioviruses |
No |
No |
Yes |
|
* Because the operator is considered to be one of the sources of release of poliovirus from the facility, specific measures of protection are required, including use of personal protective equipment, use of primary containment devices, and vaccination. † Untreated release into a closed sewage system with secondary effluent treatment in facility location (Note: all waste from facilities, potentially containing live poliovirus, should be inactivated before release through adequate and validated inactivation procedures. For facilities without a dedicated effluent treatment plant, this would normally be done through the application of heat or chemicals as part of a validated treatment process. Under no circumstances should raw poliovirus containing effluents be discharged to drains, unless the effluent treatment plant has been designed and validated to handle such effluents, effectively acting as part of the primary containment system). § Facility effluent treatment before release into closed sewage system with secondary or greater effluent treatment in facility location. ¶ HEPA (high efficiency particulate arresting) filtration on exhaust air. ** Diphtheria-tetanus-pertussis (DTP3) vaccine third dose coverage; available at http://www.who.int/gho/immunization/dtp3/en/. |
|||
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
