Invasive Cancer Incidence — Puerto Rico, 2007–2011
, MPH1, S. , MSPH1, , MD1, , MPH1, , MA, MPH2, , MS2, , MPH2, , MD, PhD2, , PhD2, , PhD1 (Author affiliations at end of text)
Cancer is a leading cause of morbidity and death in Puerto Rico (1). To set a baseline for identifying new trends and patterns of cancer incidence, Puerto Rico Central Cancer Registry staff and CDC analyzed data from Puerto Rico included in U.S. Cancer Statistics (USCS) for 2007–2011, the most recent data available. This is the first report of invasive cancer incidence rates for 2007–2011 among Puerto Rican residents by sex, age, cancer site, and municipality. Cancer incidence rates in Puerto Rico were compared with those in the U.S. population for 2011. A total of 68,312 invasive cancers were diagnosed and reported in Puerto Rico during 2007–2011. The average annual incidence rate was 330 cases per 100,000 persons. The cancer sites with the highest cancer incidence rates included prostate (152), female breast (84), and colon and rectum (43). Cancer incidence rates varied by municipality, particularly for prostate, lung and bronchus, and colon and rectum cancers. In 2011, cancer incidence rates in Puerto Rico were lower for all cancer sites and lung and bronchus, but higher for prostate and thyroid cancers, compared with rates within the U.S. population. Identifying these variations can aid evaluation of factors associated with high incidence, such as cancer screening practices, and development of targeted cancer prevention and control efforts. Public health professionals can monitor cancer incidence trends and use these findings to evaluate the impact of prevention efforts, such as legislation prohibiting tobacco use in the workplace and public places and the Puerto Rico Cessation Quitline (2) in decreasing lung and other tobacco-related cancers.
Data on new cases of invasive cancer* diagnosed during 2007–2011 were abstracted from medical records at health-care facilities, including hospitals, physician's offices, and pathology laboratories, following the North American Association of Central Cancer Registries data standards (3).The USCS dataset includes incidence data from CDC's National Program of Cancer Registries and the National Cancer Institute's Surveillance, Epidemiology, and End Results program (3,4). The National Program of Cancer Registries incidence data in this report were reported to the CDC as of November 30, 2013, and are the most recent available data.
Completeness of case ascertainment is one of six USCS publication criteria† (3,4). It is estimated using North American Association of Central Cancer Registries' completeness algorithm (3), which is based on comparing observed cancer incidence and death rates with expected rates.§ A variation on this algorithm was used to derive the completeness of case ascertainment in Puerto Rico because of differences in population attributes: expected rates were based on U.S. Hispanic data only rather than on expected rates for the total U.S. population.
Incident cases were classified by anatomic site using the International Classification of Diseases for Oncology, Third Edition (ICD-O-3). Cases with hematopoietic histologies were further classified using the WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, Fourth Edition. Denominators for Puerto Rico's incidence rates were sex-specific population estimates for Puerto Rico from the 2010 U.S. Census;¶ denominators used to calculate Puerto Rico municipality incidence rates were sex- and municipality-specific population estimates provided by the U.S. Census Bureau.** Annual incidence rates per 100,000 population were age-adjusted by the direct method to the 2000 U.S. standard population using 19 age-categories. When <16 cases were reported, the number and rate are not presented because of the potential for statistically unreliable estimates and the need to protect confidentiality (3).
Incidence rates of selected cancers over a 5-year period (2007–2011) were calculated for Puerto Rico. The incidence rates in 2011 of selected cancers in Puerto Rico and the United States (total population and by racial and ethnic groups) were compared. All central cancer registries included in the U.S. comparison met the USCS publication criteria for 2011, representing 99% coverage of the U.S. population (3). Maps were created using ArcGIS by rank-ordering the Puerto Rico municipalities' incidence rates and then grouping into quartiles.
From 2007 to 2011, a total of 68,312 invasive cancers were diagnosed in Puerto Rico, approximately 13,662 invasive cases per year. The average annual age-adjusted incidence rate was 330 cases per 100,000 persons over the 5-year period. Age-adjusted incidence rates were higher among males (395 per 100,000) than among females (281 per 100,000) (Table). By age group, rates per 100,000 population during 2007–2011 were 14 among persons aged 0–19 years, 128 among those aged 20–49 years, 594 among those aged 50–64 years, 1,281 among those aged 65–74 years, and 1,597 among those aged ≥75 years (Table).
By cancer site, average annual rates were highest for cancers of the prostate (152 per 100,000 men), female breast (84 per 100,000 women), and colon and rectum (43 overall, 53 among men, and 35 among women) (Table). These three sites combined accounted for approximately half of cancers diagnosed between 2007 and 2011 (Table). Among men, the first, second, and third most common cancers were prostate, colon and rectum, and lung and bronchus (rates of 152, 53, and 25 per 100,000 men, respectively), while among women the leading sites were breast, colon and rectum, and thyroid (rates of 84, 35, and 29 per 100,000 women, respectively).
In 2011, Puerto Rico had a lower age-adjusted all-sites cancer incidence rate (339 per 100,000) than the United States (451), regardless of U.S. racial or ethnic group (467 for U.S. non-Hispanic blacks, 462 for U.S. non-Hispanic whites, and 351 for U.S. Hispanics) (data not shown). Prostate cancer incidence was higher in Puerto Rico (150 per 100,000 men) than the U.S. overall (128) and the U.S. Hispanic population (104), but lower than the U.S. non-Hispanic black population (198) (Figure 1). Breast cancer incidence in Puerto Rico (93 per 100,000 women) was similar to the U.S. Hispanic incidence (92), both of which were lower than the U.S. overall population (122). Lung and bronchus cancer incidence in Puerto Rico was lower than in the U.S. overall population (17 versus 61 per 100,000). Colon and rectum cancer incidence in Puerto Rico (43 per 100,000) was similar to the U.S. overall population (40), regardless of race or ethnicity (Figure 1). Thyroid cancer incidence in Puerto Rico (21 per 100,000) was higher than in U.S. non-Hispanic white (15), U.S. Hispanic (12), and U.S. non-Hispanic black populations (9) (Figure 1).
Prostate cancer had notably higher incidence rates in the southeastern municipalities than in the west; colon and rectum cancer appeared to be more commonly diagnosed in the south and west (Figure 2). Lung cancers were prominent in the eastern and central municipalities; female breast cancer rates are highest among many coastline municipalities. Thyroid cancer incidence rates were highest in the north-central region of Puerto Rico (Figure 2).
Discussion
The Puerto Rico Central Cancer Registry has been collecting data on cancer in Puerto Rico since 1951 and has been part of National Program of Cancer Registries since 1997. This is the first report of the USCS dataset with the Puerto Rico cancer registry data and it shows that for 2011, the latest year for which data are available for comparison, the overall cancer incidence rate in Puerto Rico was lower than in the U.S. population. Puerto Rico had a lower rate of female breast cancer compared with U.S. non-Hispanic whites and blacks and the lowest rate of lung cancer compared with all race and ethnic groups included in this analysis. However, Puerto Rico had the second highest prostate cancer incidence rates after U.S. non-Hispanic blacks and it also had the highest incidence rate of thyroid cancer. Puerto Rico had similar incidence rates to U.S. populations for colon and rectum cancer.
Differences in reported cancer incidence rates between U.S. and Puerto Rican residents might be partly explained by differences in the prevalence of risk factors such as behaviors associated with cancers or in the use of cancer screening tests. Lower rates of female breast cancer incidence might be attributable to the protective effect of young age at first live birth, which is more common in Puerto Rico than in the United States (5). Also, CDC's Behavioral Risk Factor Surveillance System data show that the prevalence of current cigarette smoking in Puerto Rico is low compared with U.S. states; only Utah is lower (6). Consistent with these data, National Health Interview Survey data show that U.S. Hispanics' current cigarette smoking rate is generally lower than the rate in the general U.S. population (7), which might explain the lower rates of lung cancer.
There are also geographic variations in cancer incidence by cancer site. As has been shown in previous investigations in Puerto Rico, the incidence rates of cancers of the kidney, pancreas, prostate, breast, colon and rectum, thyroid, and lung were higher in areas of Puerto Rico with higher socioeconomic position (8). However, prostate cancer incidence was also found to be high in the southeastern portion of the country, an area with a lower socioeconomic position. Possible explanations include higher rates of prostate-specific antigen testing in this region (9).
The findings in this report are subject to at least two limitations. First, delays in cancer reporting can result in an undercount of cancer incidence, particularly for the most recent years (10). Second, the 2011 population was estimated from the 2010 U.S. Census, which might lead to under- or over-estimations of incidence rates.
Data from population-based central cancer registries are important for monitoring trends over time and identifying opportunities to reduce cancer incidence and mortality, particularly among high-risk groups and underserved areas (3). Data from the Puerto Rico Central Cancer Registry are used to identify and select cancer control priorities, identify populations of interest for implementation of cancer control strategies††, and respond to concerns about possible cancer clusters on the island, as well as for evaluation of the impact of cancer control strategies (2).
Acknowledgment
Puerto Rico central and hospital based cancer registry personnel, Jessica B. King, MPH, Division of Cancer Prevention and Control, CDC, and Nayda Figueroa-Vallés, MD, Puerto Rico Central Cancer Registry.
1Division of Cancer Prevention and Control, National Center for Chronic Disease Prevention and Health Promotion, CDC; 2 Puerto Rico Central Cancer Registry. (Corresponding author: Mary Elizabeth O'Neil, moneil@cdc.gov, 770-488-8257)
References
- CDC. Deaths: final data for 2012 — detailed tables for the National Vital Statistics Report (NVSR). Available at http://www.cdc.gov/nchs/data/nvsr/nvsr63/nvsr63_09.pdf.
- Ortiz AP, Díaz-Toro EC, Calo WA, et al. Characteristics of smokers accessing the Puerto Rico Quitline. P R Health Sci J 2008;27:213–9.
- U.S. Cancer Statistics Working Group. United States cancer statistics: 1999–2011 incidence and mortality web-based report. Atlanta, GA: U.S. Department of Health and Human Services, CDC and National Cancer Institute; 2014. Available at http://www.cdc.gov/cancer/npcr/uscs/index.htm
- Henley SJ, Singh SD, King J, Wilson R, O'Neil ME, Ryerson AB; CDC. Invasive cancer incidence and survival - United States, 2011. MMWR Morb Mortal Wkly Rep 2015;64:237–42.
- Mathews TJ, Hamilton BE. Mean age of mother, 1970–2000. National vital statistics reports; vol 51 no 1. Hyattsville, Maryland: National Center for Health Statistics. 2002.
- CDC. State-specific prevalence of cigarette smoking and smokeless tobacco use among adults — United States, 2009. MMWR Morb Mortal Wkly Rep 2010;59:1400–6.
- Agaku IT, King BA, Dube SR. Current cigarette smoking among adults - United States, 2005-2012. MMWR Morb Mortal Wkly Rep 2014;63:29–34.
- Torres-Cintrón M, Ortiz AP, Ortiz-Ortiz KJ, et al. Using a socioeconomic position index to assess disparities in cancer incidence and mortality, Puerto Rico, 1995-2004. Prev Chronic Dis 2012;9:E15.
- Serrano-Rodríguez R, Amill-Rosario A. Prevalence of cancer screening, Puerto Rico 2012. Puerto Rico Behavioral Risk Factor Surveillance System, Puerto Rico Department of Health, Centers for Disease Control and Prevention. 2013.
- Clegg LX, Feuer EJ, Midthune DN, Fay MP, Hankey BF. Impact of reporting delay and reporting error on cancer incidence rates and trends. J Natl Cancer Inst 2002;94:1537–45.
* Invasive cancers are all cancers excluding basal and squamous cell skin cancers except when these occur on the skin of the genital organs, and in situ cancers except in the urinary bladder.
† Cancer registries demonstrated that cancer incidence data were of high quality by meeting the six USCS publication criteria: 1) case ascertainment is ≥ 90% complete, 2) ≤ 5% of cases are ascertained solely on the basis of a death certificate, 3) ≤ 3% of cases are missing information on sex, 4) ≤ 3% of cases are missing information on age, 5) ≤ 5% of cases are missing information on race, and 6) ≥ 97% of the registry's records passed a set of single-field and inter-field computerized edits that test the validity and logic of data components. Additional information is available at http://www.cdc.gov/cancer/npcr/uscs/index.htm.
§ Additional information available at: http://www.cdc.gov/cancer/npcr/uscs/technical_notes/criteria.htm
¶ The 2007–2009 Puerto Rico population estimates were abstracted from the file "2000–2010 Puerto Rico Characteristics Intercensal Population Estimates," source: U.S. Census Bureau, Population Division; release date: October 2012. The 2010–2011 Puerto Rico population estimates were abstracted from the file "Annual Estimates of the Resident Population by Single Year of Age and Sex for the United States, States, and Puerto Rico Commonwealth: April 1, 2010 to July 1, 2012." U.S. Census Bureau, Population Division, release date June 2013.
** Annual estimates of the resident population by sex for Puerto Rico municipalities were provided by the U.S. Census Bureau, Population Division using the Vintage 2013 and 2000–2010 intercensal estimates series.
†† Additional information available at: http://ftp.cdc.gov/pub/Publications/Cancer/ccc/puerto_rico_ccc_plan_2008_2012.pdf.
What is already known on this topic?
As of 2012, cancer is a leading cause of illness and death in Puerto Rico. Many cancers are preventable.
What is added by this report?
Data on cancer incidence in Puerto Rico are now included in U.S. Cancer Statistics and show that during 2007–2011, the overall, age-adjusted, annual cancer incidence rate was 330 cases per 100,000 persons and varies by municipality. Cancer sites with the highest incidence included prostate (152), female breast (84), and colon and rectum (43). In 2011, overall, age-adjusted, annual cancer incidence in Puerto Rico was 339 cases per 100,000 persons compared with 451 in the United States, and incidence rates in Puerto Rico were lower for lung and bronchus cancer but higher for prostate and thyroid cancers.
What are the implications for public health practice?
Differing rates of cancer by municipality indicate a need to assess geographic variations in risk factor prevalence and cancer screening practices. The cancer rates for 2007–2011 will be critical for assessing the effectiveness of cancer prevention programs.
FIGURE 1. Age-adjusted rates* of invasive cancer† incidence by selected primary cancer site, geographic location, race and ethnicity — National Program of Cancer Registries and the Surveillance, Epidemiology, and End Results program§, Puerto Rico and United States, 2011
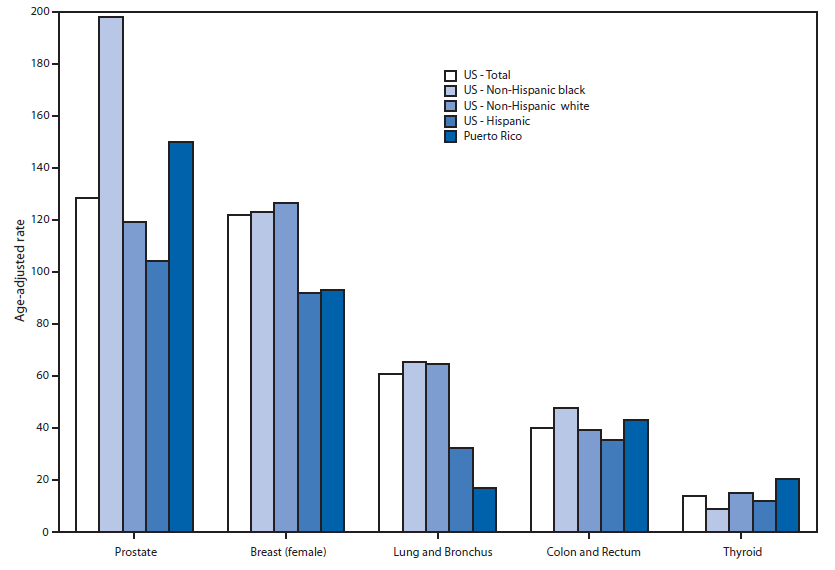
* Incidence rates are per 100,000 persons and are age-adjusted to the 2000 U.S. standard population.
† Excludes basal and squamous cell carcinomas of the skin except when these occur on the skin of the genital organs, and in situ cancers except urinary bladder.
§ Compiled from cancer registries that meet the data-quality criteria for all invasive cancer sites combined (representing 99% of the U.S. population).
Alternate Text: The figure above is a bar chart showing age-adjusted rates of invasive cancer incidence by selected primary cancer site, geographic location, race, and ethnicity in Puerto Rico and the United States during 2011.
FIGURE 2. Age-adjusted incidence rates* of invasive cancer† by selected primary cancer sites and municipality – National Program of Cancer Registries, Puerto Rico, 2007–2011
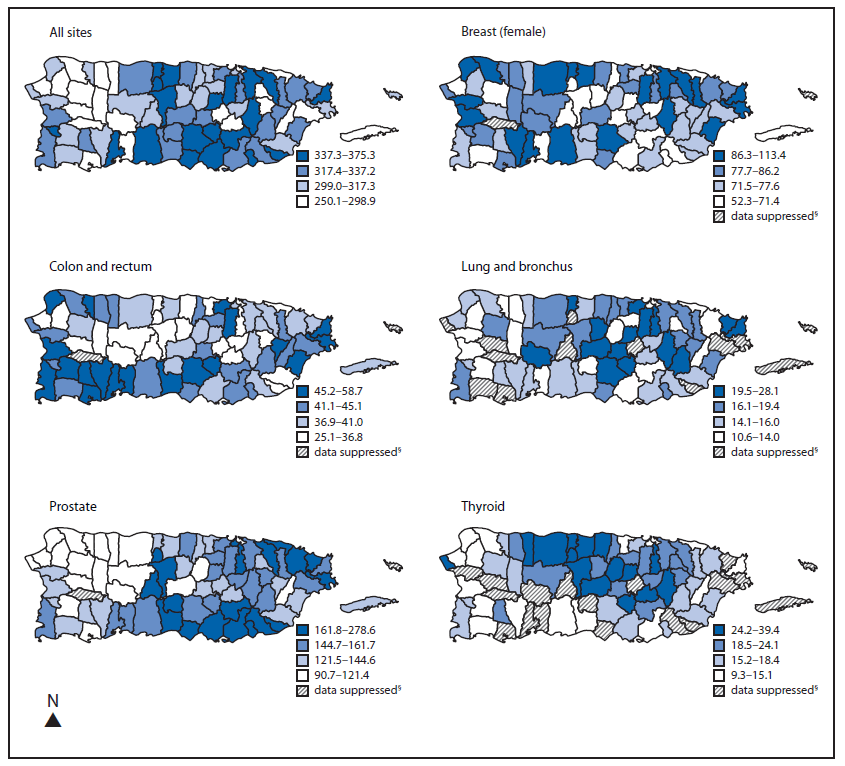
* Incidence rates are per 100,000 persons and are age-adjusted to the 2000 U.S. standard population.
† Excludes basal and squamous cell carcinomas of the skin except when these occur on the skin of the genital organs, and in situ cancers except urinary bladder.
§ Data not given because <16 cases were reported.
Alternate Text: The figure above consists of six maps of Puerto Rico showing age-adjusted incidence rates of invasive cancer by selected primary cancer sites and municipality in Puerto Rico during 2007-2011.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
