Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Diabetes Death Rates Among Youths Aged ≤19 Years — United States, 1968–2009
Although diabetes mellitus most often is diagnosed in adulthood, it remains one of the most common serious chronic diseases of childhood (1). Youths with diabetes are at risk for diabetes-related mortality because of acute complications that can result from the condition (2), including diabetic ketoacidosis and hypoglycemia (3). In the United States in 2010, an estimated 215,000 persons aged ≤19 years had diagnosed diabetes (3). Medical care for diabetes has improved considerably in recent decades, leading to improved survival rates. However, recent trends in diabetes death rates among youths aged <10 years and 10–19 years in the United States have not been reported. To assess these trends, CDC analyzed data from the National Vital Statistics System for deaths in the United States with diabetes listed as the underlying cause during 1968–2009. This report highlights the results of that analysis, which found that diabetes-related mortality decreased 61%, from an annual rate of 2.69 per million for the period 1968–1969 to a rate of 1.05 per million in 2008–2009. The percentage decrease was greater among youths aged <10 years (78%) than among youths aged 10–19 years (52%). These findings demonstrate improvements in diabetes mortality among youths but also indicate a need for continued improvement in diabetes diagnosis and care.
To produce stable estimates, annual diabetes death rates among youths aged ≤19 years in the United States were calculated from National Vital Statistics System data for 2-year or 3-year periods from 1968 to 2009. Three-year periods were preferred except when the years would have included different International Classification of Diseases (ICD) codes. Diabetes-related mortality is based on information from death certificates filed in all 50 states and the District of Columbia and collected by CDC. The numbers of deaths for the study periods where diabetes was listed as the underlying cause of death were obtained from CDC Wonder.* Denominators were based on U.S. census estimates for each year.
A diabetes death was defined as a death with an underlying ICD-8 cause of death code of 250.0 or 250.9 for the years 1968–1978; ICD-9 codes of 250.0–250.9 for the years 1979–1998, and ICD-10 codes of E10–E14 for the years 1999–2009. Previous analyses of comparability between ICD-8 and ICD-9† and between ICD-9 and ICD-10§ found little difference in definitions between the coding methods (5,6). Joinpoint regression was used to analyze trends for youths aged <10 years and 10–19 years. Joinpoint regression uses permutation tests to identify points (joinpoints) where linear trends change significantly in direction or magnitude (e.g., zero joinpoints indicate a straight line).¶ The rate of change for each trend is tested to determine whether the change is significantly different from zero, and each trend in the final model is described by an annual percentage change (APC) with a 95% confidence interval (CI). If the CI does not contain zero, the APC is considered significantly different from zero.
From 1968–1969 to 2008–2009, the death rate from diabetes among youths aged ≤19 years decreased 61%, from 2.69 per million to 1.05 per million (Table). The death rate among youths aged <10 years decreased 78%, from 1.80 per million to 0.39 per million, and the death rate among youths aged 10–19 years decreased 52%, from 3.56 per million to 1.71 per million.
The trends for diabetes death rates for youths aged <10 years and youths aged 10–19 years indicate different patterns of decrease (Figure). For youths aged <10 years, a steady decrease in diabetes death rates was observed from 1968 to 1995, with an APC of -5.7 (CI = -6.6 to -4.7). However, from 1995 to 2009, the APC was -0.3 (CI = -3.5 to 4.3). For youths aged 10–19 years, a decrease in diabetes death rates occurred from 1968 to 1984, with an APC of -6.5 (CI = -7.9 to -5.1), followed by an increase in rates with an APC of 1.6 (CI = 0.8 to 2.4) from 1984 to 2009.
Reported by
Sharon Saydah, PhD, Giuseppina Imperatore, MD, Linda Geiss, MS, Edward Gregg, PhD, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Corresponding contributor: Sharon Saydah, ssaydah@cdc.gov, 301-458-4183.
Editorial Note
The decline in diabetes death rates noted from 1968–1969 to 2008–2009 occurred despite indications of an increase in the last 3 decades in the incidence of type 1 diabetes among U.S. youths (4). Although national data on incidence of diabetes in youth are not yet available, among Colorado youths aged <17 years, the incidence of type 1 diabetes increased from 14.8 per 100,000 for the period 1978–1988 to 23.9 per 100,000 for the period 2002–2004 (4). The prevalence of diabetes among youths is determined by a number of factors, including the incidence of new cases and the number of deaths among youths with diabetes. The findings in this report that the overall death rate from diabetes has decreased among U.S. youths aged ≤19 years might contribute to an overall increase in prevalence of diabetes among youths.
Among youths, diabetes deaths are more likely to result from direct acute complications of diabetes such as ketoacidosis or hypoglycemia (7). In these cases, diabetes is listed as the underlying cause. These causes of diabetes deaths largely are preventable. Possible reasons for the reduction in diabetes-related deaths among persons aged <10 years since 1968–1969 and among persons aged 10–19 years from 1968–1969 to 1986–1986 include improved diabetes care and treatment, (e.g., improved technology for blood glucose monitoring and insulin administration, such as insulin pumps) and increased awareness of diabetes symptoms, possibly resulting in earlier recognition and treatment. Other possible reasons include advances in education regarding diabetes and management of diabetic ketoacidosis.
Previous analysis of diabetes death rates among youths found a steady decline from 1968 to 1985 and no change from 1986 to 1998 (8). Reasons for the increase in diabetes-related mortality among youths aged 10–19 years since 1984–1986 are unknown. One possibility is that youths who had diabetes diagnosed before age 10 years and who previously might have died before reaching age 10 years are living longer and dying at ages 10–19 years. Similar findings have been observed in other studies. For example, during 1977–2000, in a Swedish cohort of youths with type 1 diabetes, the majority of deaths occurred at approximately age 15 years (9).
The findings in this report are subject to at least three limitations. First, CDC Wonder does not distinguish between diabetes types in ICD-8 or ICD-9 mortality codes. However, type 2 diabetes rarely is diagnosed in youths aged ≤10 years, and diagnosed in only 20% of youths aged 10–19 years. Second, because of the small number of deaths, assessing whether the age group trends varied by race/ethnicity or geographic region was not possible. However, a previous report highlighted disparities in diabetes mortality by race among youths in the United States (10). Finally, these data do not permit differentiating between deaths occurring in persons with known diabetes and deaths occurring in persons with diabetes diagnosed only at the time of death.
CDC, along with the National Institute of Diabetes and Digestive and Kidney Disease at the National Institutes of Health, supports the SEARCH for Diabetes in Youth study.** This study will provide estimates of trends in the incidence and prevalence of diabetes among youths in the United States and will look at all-cause and diabetes-related mortality among youths with diabetes. Although the findings in this report demonstrate improvement in diabetes mortality among youths, particularly among those aged <10 years, deaths resulting from diabetes in youths potentially are preventable, and these findings indicate a need for improved diabetes diagnosis and care, especially among youths aged 10–19 years, whose risk for diabetes-related mortality appears to have increased in recent years.
References
- Zylke JW, DeAngelis CD. Pediatric chronic diseases—stealing childhood. JAMA 2007;297:2765–6.
- Patterson CC, Dahlquist G, Harjutsalo V, et al. Early mortality in EURODIAB population-based cohorts of type 1 diabetes diagnosed in childhood since 1989. Diabetologia 2007;50:2439–42.
- CDC. 2011 national diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States. Atlanta, GA: US Department of Health and Human Services, CDC; 2011. Available at http://www.cdc.gov/diabetes/pubs/factsheet11.htm. Accessed October 29, 2012.
- Vehik K, Hamman RF, Lezotte D, et al. Increasing incidence of type 1 diabetes in 0- to 17-year-old Colorado youth. Diabetes Care 2007;30:503–9.
- National Center for Health Statistics, CDC. Estimates of selected comparability ratios based on dual coding of 1976 death certificates by the eighth and ninth revisions of the international classification of diseases. Monthly Vital Statistics Report 1980;28(11).
- Anderson RN, Minino AM, Hoyert DL, Rosenberg HM. Comparability of cause of death between ICD-9 and ICD-10: preliminary estimates. Natl Vital Stat Rep 2001;49(2).
- Edge JA, Ford-Adams ME, Dunger DB. Causes of death in children with insulin dependent diabetes 1990–96. Arch Dis Child 1999;81:318–23.
- DiLiberti JH, Lorenz RA. Long term trends in childhood diabetes mortality: 1968–1998. Diabetes Care 2001;24:1348–52.
- Dahlquist G, Kallen B. Mortality in childhood-onset type 1 diabetes: a population-based study. Diabetes Care 2005;28:2384–7.
- CDC. Racial disparities in diabetes mortality among persons aged 1–19 years—United States, 1979–2004. MMWR 2007;56:1184–7.
* Available at http://wonder.cdc.gov.
† Comparability ratio of ICD-8 to ICD-9 for diabetes deaths was 0.9991.
§ Comparability ratio of ICD-9 to ICD-10 for diabetes deaths was 1.0082.
¶ Additional information available at http://srab.cancer.gov/joinpoint.
** Additional information available at http://www.cdc.gov/diabetes/pubs/pdf/search.pdf.
What is already known on this topic?
Diabetes in youths is a serious chronic disease. Youths with diabetes are at a risk for mortality caused by acute complications of the disease.
What is added by this report?
In 2008–2009, the rate of diabetes deaths was 1.05 per million persons aged ≤19 years, a decline of 61% from 1968–1969. Diabetes mortality decreased among youths aged <10 years and youths aged 10–19 years by 78% and 52%, respectively. However, for youths aged 10–19 years an annual percentage increase of 1.6 occurred from 1984 to 2009.
What are the implications for public health practice?
Deaths from diabetes in young persons are potentially preventable. The recent increase in diabetes-related mortality among youths aged 10–19 years shows a need for improved diabetes diagnosis and care in this age group and research to better understand these deaths.
FIGURE. Annual death rates from diabetes* per 1 million youths aged <10 years and 10–19 years — United States, 1968–2009
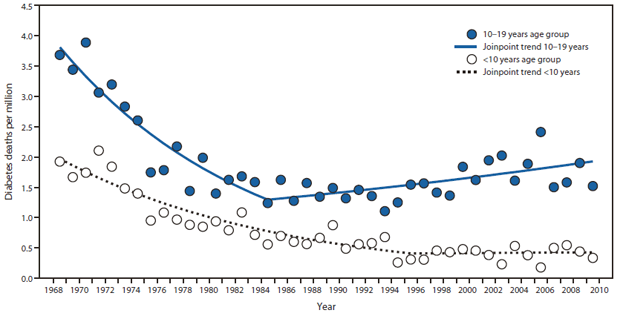
* Based on diabetes as underlying cause of death, using International Classification of Diseases (ICD) codes as follows: for years 1968–1978, ICD-8 codes 250.0 or 250.9; for years 1979–1998, ICD-9 codes 250.0–250.9; and for years 1999–2009, ICD-10 codes E10–E14.
Alternate Text: The figure above shows annual death rates from diabetes per 1 million youths aged <10 years and 10-19 years in the United States during 1968-2009. For youths aged <10 years, a steady decrease in diabetes death rates was observed from 1968 to 1995, with an annual percentage change (APC) of -5.7. However, from 1995 to 2009, the APC was -0.3. For youths aged 10-19 years, a decrease in diabetes death rates occurred from 1968 to 1984, with an APC of -6.5, followed by an increase in rates with an APC of 1.6 from 1984 to 2009.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
