Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Progress Toward Poliomyelitis Eradication — Afghanistan and Pakistan, January 2011–August 2012
In 1988, the World Health Assembly resolved to eradicate polio, which led to the establishment of the Global Polio Eradication Initiative (GPEI). In 2012, however, the transmission of indigenous wild poliovirus (WPV) continued uninterrupted in Afghanistan, Pakistan, and Nigeria (1,2), leading the World Health Assembly to declare completion of polio eradication a programmatic emergency for global public health (3). This report updates previous reports (1,4,5) and describes polio eradication activities and progress in Afghanistan and Pakistan during January 2011–August 2012, as of September 9, 2012. During 2011, 80 WPV cases were confirmed in Afghanistan, compared with 25 WPV cases in 2010; 17 WPV cases were confirmed during January–August 2012, compared with 34 WPV cases for the same period in 2011. In Pakistan, 198 WPV cases were confirmed in 2011, compared with 144 WPV cases in 2010; 30 WPV cases were confirmed during January–August 2012, compared with 88 WPV cases during the same period in 2011. During January 2011–August 2012, no WPV type 3 (WPV3) cases were confirmed in Afghanistan, and four confirmed WPV3 cases and one case with coinfection of WPV3 and WPV type 1 (WPV1) were reported in Pakistan. Violence targeting vaccinators has occurred previously in Afghanistan and recently in Pakistan. To progress further toward interruption of WPV transmission within their countries and across their shared border, the governments of Afghanistan and Pakistan might consider reviewing the implementation of their national emergency action plans (6,7) and determine how to enhance the safety of vaccination teams within conflict-affected areas of both countries.
Immunization Activities
Estimated national routine immunization coverage of infants with 3 doses of oral polio vaccine (OPV3) is 66% in Afghanistan and 75% in Pakistan, with subnational variation in both countries (8). A surrogate measure of routine OPV3 coverage based on parental recall and immunization cards of children aged 6–23 months with acute flaccid paralysis (AFP) not the result of polio (non-polio AFP)* was 61% nationally in Afghanistan; 15% in the conflict-affected South Region and Farah Province in the West Region combined; 71% in the West Region, excluding Farah Province; and 78% in the rest of the country. OPV3 coverage among children aged 6–23 months with non-polio AFP cases in Pakistan was 63% nationally, 26% in the conflict-affected Federally Administered Tribal Areas (FATA), 63% in Khyber Pakhtunkhwa (KP) Province, 52% in Sindh Province, 18% in Balochistan Province, and 77% in Punjab Province. Nationally, only 3.3% of children aged 6–23 months with non-polio AFP did not receive any oral polio vaccine (OPV) doses through routine or supplementary immunization activities (SIAs).†
During January 2011–August 2012, house-to-house SIAs generally targeted children aged ≤59 months using different OPV formulations, including bivalent types 1 and 3 and trivalent. During this period, six national immunization days and 10 subnational immunization days were conducted in Afghanistan in the East, Southeast, and South regions, and in Farah Province in the West Region. During a combined measles and OPV campaign, children aged ≤10 years were targeted. SIA planning and implementation in 2011 apparently worsened compared with previous years, as indicated by the proportion of children aged 6–23 months with non-polio AFP in high-risk districts having not received any doses of OPV vaccine, which rose from 9% in 2010 in the South Region to 21% in 2011. In Pakistan, 7 national immunization days were conducted and 8 subnational immunization days were conducted in high-risk districts in the main WPV transmission areas of FATA, KP, Sindh, Balochistan, and southern Punjab. Several smaller SIAs targeting high-risk areas and migratory, internally displaced, and underserved or marginalized groups were conducted. Most campaigns targeted children aged <5 years; however, in Khyber Agency (Bara), FATA, a short interval additional dose (SIAD) strategy§ campaign in 2012 targeted children aged <15 years because much of this area had not been reached in 3 years. A significant population exodus, from Bara Tehsil of Khyber Agency to neighboring parts of KP (mainly Peshawar and Nowshera), occurred during April and May 2012. The displaced population was targeted with multiple SIA rounds using bivalent types 1 and 3 in the hosting communities (target age group: <5 years) and in a camp for displaced persons in Jalozai Nowshera (target age group: <15 years).
During 2011–2012, as in past years, SIA teams were unable to reach thousands of children living in areas that have been inaccessible¶ to vaccination teams because of insecurity. In Afghanistan, the estimated proportion of targeted children living in inaccessible areas in the South Region was 6%–21% (72,500–273,000 children) during SIAs conducted in 2010 and 2011, and 2%–5% (28,400–65,000 children) in SIAs during January–June 2012. In Pakistan, the proportion of targeted children living in inaccessible areas of KP during SIAs decreased from <1%–2% (<30,000–100,000 children) during January–March 2010 to <0.2% (<6,000 children) during April 2010–December 2011. In FATA, however, the proportion of targeted children living in inaccessible areas was 20%–31% during 2010 and 9%–24% during 2011, leaving approximately 99,000–350,000 children unreached during each SIA conducted during 2010 and 2011. During January–July 2012, 6%–23% (64,000–257,500) of children in the target population in FATA were not accessible. Despite a gradual improvement in access to children in FATA, approximately 200,000 children were unreachable because of a ban on polio SIAs recently imposed by some local authorities in the tribal agencies of North and South Waziristan. All areas have been accessible in KP since September 2011.
WPV Surveillance
AFP surveillance. Standard indicators are used to monitor AFP surveillance performance.** In 2011, the annual national non-polio AFP rate (per 100,000 population aged <15 years) was 10.5 in Afghanistan (range among the eight regions: 6.0–12.8), and 7.2 in Pakistan (range among the seven provinces/regions: 2.3–9.7). The percentage of AFP cases for which adequate specimens were collected was 92% in Afghanistan (range: 80%–98%) and 88% in Pakistan (range: 78%–93%). Despite overall high AFP surveillance performance indicators, genomic sequencing data from WPVs obtained from confirmed polio cases and environmental surveillance samples continue to indicate surveillance gaps of WPV in certain areas of Pakistan and Afghanistan.
Environmental surveillance. In Pakistan, AFP surveillance is supplemented by environmental surveillance. During 2011–August 2012, 353 sewage samples from 21 sites in 11 cities from all major provinces of Pakistan were tested for polioviruses. The number of cities with sewage sampling increased from eight in 2011 to 11 in 2012. WPVs frequently have been isolated from sewage samples collected in all major cities in Pakistan since testing began in mid-July 2009, including several large urban areas where there was absence of confirmed WPV in reported AFP cases: Lahore in Punjab (latest confirmed case: December 2011, latest positive sewage sample: August 2012), Rawalpindi (latest confirmed case: April 2010, latest positive sewage sample: May 2012), and Sukkur (latest confirmed case: September 2010, latest positive sewage sample: July 2012). WPV continues to be isolated from the majority of environmental samples at most sampling sites, although the frequency of WPV-positive environmental samples decreased in Quetta, Balochistan, which has had no WPV-positive environmental sample since February 2012. WPV3 has not been detected in sewage samples at any site since October 2010.
WPV Epidemiology
In Afghanistan, 80 WPV1 cases were reported during 2011, compared with 25 WPV cases (17 WPV1, eight WPV3) in 2010, and 17 WPV1 cases were reported during January–August 2012, compared with 34 WPV1 cases during the same period in 2011 (Table, Figures 1 and 2) (4,5). The last WPV3 case reported in Afghanistan was in South Region in April 2010. During January 2011–August 2012, 72 (74%) WPV cases were reported among children aged <36 months. Among the 72 children, 24 (33%) received no OPV doses, 23 (32%) received 1–3 OPV doses, and 25 (35%) received ≥4 OPV doses. During this period, WPV cases were reported in 40 (12%) of 329 districts, including 13 high-risk districts†† in the southwestern provinces of Kandahar, Helmand, Urozgan, and Farah.
In Pakistan, 198 WPV cases (196 WPV1, two WPV3) were reported during 2011, compared with 144 WPV cases (120 WPV1, 24 WPV3) during 2010; 30 WPV cases (27 WPV1, two WPV3, and one case with isolation of both WPV1 and WPV3) were reported during January–August 2012, compared with 88 during the same period in 2011 (Table, Figures 1 and 2). All WPV3 cases reported in Pakistan since 2011 were from Khyber Agency, FATA; the most recent cases were reported in April 2012. During January 2011–August 2012, 192 (84%) of 228 WPV cases were among children aged <36 months. Among the 228 children aged <36 months, 68 (30%) received no OPV doses, 51 (22%) received 1–3 OPV doses, and nine (4%) received ≥4 OPV doses. WPV cases were reported in 60 (38%) of 157 districts in Pakistan during 2011, compared with 40 (30%) districts during 2010, and from 17 (11%) districts during January–August 2012. During 2010, 98 (68%) of 144 cases were from KP and FATA and 39 (27%) were from Balochistan and Sindh; during 2011, 82 (41%) of 198 cases were from KP and FATA and 105 (53%) were from Balochistan and Sindh; by comparison, 22 (73%) of 30 cases reported during January–August 2012 were from KP and FATA. Of the 13 polio cases reported from FATA in 2012, nine (69%) were from Bara Tehsil of Khyber Agency, which has not been accessible for polio SIAs since September 2009.
Reported by
World Health Organization (WHO) Country Office Kabul, Afghanistan. WHO Country Office Islamabad, Pakistan. WHO Eastern Mediterranean Regional Office, Cairo, Egypt. Regional Reference Laboratory for Poliovirus, Islamabad, Pakistan. Global Polio Laboratory Network. Polio Eradication Dept, WHO, Geneva, Switzerland. Div of Viral Diseases, National Center for Immunization and Respiratory Diseases; Global Immunization Div, Center for Global Health, CDC. Corresponding contributor: Jenna Webeck, Global Immunization Div, Center for Global Health, CDC, hwk5@cdc.gov, 404-553-7617.
Editorial Note
In Afghanistan, more than three times as many WPV cases occurred in 2011 as in 2010; in Pakistan, WPV cases increased by 37% in 2011 compared with 2010. In 2012, WPV1 transmission continues in the known endemic areas of southwestern Afghanistan. WPV1 transmission is widespread in high-risk districts in Pakistan; however, the number of reported WPV cases in Pakistan in 2012 has decreased 66% compared with the same period in 2011. Only five WPV3-associated cases have been reported since January 2011, all from a limited area in Pakistan.
In the southwestern endemic zone of Afghanistan, SIA planning and implementation in 2011 worsened compared with previous years, even though access to children in high-risk areas continued to improve. The 2012 Afghanistan National Polio Eradication Emergency Action Plan defined major challenges and key activities to address these challenges (6). New strategic approaches include a major surge in human resources, particularly at district and provincial administrative levels, management training, and use of locally recruited permanent polio teams in high-risk districts for continuous house-to-house vaccination. Even with the new strategies to partly address the security concerns, the national emergency action plan highlights other key obstacles to interrupting transmission, such as low quality program management and lack of accountability (6).
In Pakistan, 73% of WPV cases reported in 2012 were in insecure areas of FATA and KP. One third of these cases were reported from one tribal agency, Khyber, the only known remaining focus of WPV3 transmission in Asia. Recent bans on polio vaccination by some local authorities in North Waziristan and South Waziristan in FATA, and deadly attacks on polio workers in Gaddap, a high-risk area of Karachi in Sindh Province, have further increased the difficulties in reaching underimmunized children. To achieve polio eradication, both Pakistan and Afghanistan might consider how to enhance the safety of vaccination teams within conflict-affected areas.
Implementation of the Pakistan Polio Eradication National Emergency Action Plan, launched in early 2011, augmented in early 2012, and monitored at the highest political level, has made district commissioners and union council medical officers responsible for program implementation. Staffing also has increased substantially, particularly at the union council level (7). SIA preparations are being monitored systematically; if preparations in union councils or districts are not meeting quality benchmarks, SIAs are deferred.
Although WPV transmission within Afghanistan and Pakistan still occurs separately, genetic sequencing of polioviruses detected during AFP surveillance and environmental sewage sampling indicate that population movement (cross-border and internal) contributes substantially to the spread of poliovirus in Afghanistan and Pakistan. The number of transit teams in Pakistan providing OPV to children passing through border crossings and bus stops has increased, and regular cross-border planning and coordination of SIAs and surveillance activities with Afghanistan is taking place.
GPEI's 2012–2013 Global Emergency Action Plan (9), together with the national emergency action plans, seeks to accelerate activities to put the remaining countries with WPV transmission back on track toward interruption of WPV transmission (1,6,7). Although GPEI activities in Afghanistan and Pakistan have been accelerated, ongoing WPV transmission in both countries remains a threat to achieving the GPEI goal (10).
References
- CDC. Progress toward interruption of wild poliovirus transmission—worldwide, January 2011–March 2012. MMWR 2012;61:353–7.
- CDC. Progress toward poliomyelitis eradication—Africa, 2011. MMWR 2012;61:190–4.
- World Health Assembly. Poliomyelitis: intensification of the global eradication initiative. Agenda item A65/20. Geneva, Switzerland: World Health Organization; 2012. Available at http://apps.who.int/gb/ebwha/pdf_files/wha65/A65_20-en.pdf . Accessed September 14, 2012.
- CDC. Progress toward poliomyelitis eradication—Afghanistan and Pakistan, 2009. MMWR 2010;59:268–72.
- CDC. Progress toward poliomyelitis eradication—Afghanistan and Pakistan, January 2010–September 2011. MMWR 2011;60:1523–7.
- Global Polio Eradication Initiative. Afghanistan Emergency Action Plan for Polio Eradication 2012–2013. Geneva, Switzerland: World Health Organization; 2012. Available at http://www.polioeradication.org/portals/0/document/aboutus/governance/imb/6imbmeeting/3.4_6imb.pdf. Accessed September 14, 2012.
- Government of Islamic Republic of Pakistan. Augmenting the National Emergency Action Plan for Polio Eradication in 2012. January 2012. Islamabad, Pakistan: Government of Islamic Republic of Pakistan; 2012. Available at http://www.polioeradication.org/portals/0/document/aboutus/governance/imb/6imbmeeting/8.5_6imb.pdf. Accessed September 12, 2012.
- World Health Organization. WHO vaccine-preventable diseases monitoring system: 2011 global summary. Geneva, Switzerland: World Health Organization; 2011. Available at http://www.who.int/vaccines/globalsummary/immunization/countryprofileselect.cfm. and http://apps.who.int/immunization_monitoring/en/globalsummary/countryprofileselect.cfm. Accessed August 15, 2012.
- Global Polio Eradication Initiative. Global Polio Eradication Initiative Emergency Action Plan 2012–2013. Geneva, Switzerland: World Health Organization; 2012. Available at http://www.polioeradication.org/resourcelibrary/strategyandwork/emergencyactionplan.aspx. Accessed October 1, 2012.
- Independent Monitoring Board of the Polio Eradication Initiative. Every missed child: report of the Independent Monitoring Board of the Global Polio Eradication Initiative. Geneva, Switzerland: World Health Organization; 2012. Available at http://www.polioeradication.org/portals/0/document/aboutus/governance/imb/6imbmeeting/imb6_report.pdf. Accessed August 15, 2012.
* Vaccination histories of children aged 6–23 months with AFP who do not test WPV-positive are used to estimate OPV coverage of the overall target population and to corroborate national reported routine immunization coverage estimates.
† Mass campaigns conducted for a brief period (days to weeks) in which 1 dose of OPV is administered to all children aged <5 years, regardless of vaccination history. Campaigns can be conducted nationally or in sections of the country.
§ SIADs are used during negotiated periods of nonviolence in otherwise inaccessible areas to vaccinate children with a monovalent OPV or bivalent OPV dose, which is administered within 1–2 weeks of the prior dose.
¶ Areas considered too dangerous by the World Health Organization (WHO) and the local government to conduct an SIA.
** The quality of AFP surveillance is monitored by performance indicators that include 1) detection rate of non-polio AFP cases and 2) the proportion of AFP cases with adequate stool specimens. WHO operational targets for countries with endemic polio transmission are a non-polio AFP detection rate of at least two cases per 100,000 population aged <15 years and adequate stool specimen collection from >80% of AFP cases, in which two specimens are collected at least 24 hours apart, both within 14 days of paralysis onset, and shipped on ice or frozen packs to a WHO-accredited laboratory, arriving in good condition.
†† High-risk districts include those persistently affected by WPV transmission and those in proximity to the persistently affected districts.
What is already known on this topic?
Afghanistan and Pakistan are two of the three remaining countries (including Nigeria) in which indigenous wild poliovirus (WPV) transmission has never been interrupted. Conflict in both countries has made some areas inaccessible for polio eradication activities.
What is added by this report?
WPV type 1 (WPV1) transmission occurred in conflict-affected areas in the South Region of Afghanistan, and in three groups of districts in Pakistan in 1) districts bordering Afghanistan in the Federally Administered Tribal Areas and Khyber Pakhtunkhwa, 2) southern Sindh Province, and 3) the northwest border area in Balochistan. In addition to transmission within each country, genetic sequencing data confirms cross-border transmission between Pakistan and Afghanistan resulting from substantial population movements within and between countries. Positive sewage samples in Pakistan, in areas with no recent confirmed cases, highlight unrecognized continued polio transmission.
What are the implications for public health practice?
Ongoing WPV1 transmission in parts of Afghanistan and Pakistan remains a substantial threat to the Global Polio Eradication Initiative goal of a polio-free world. To achieve polio eradication, both Afghanistan and Pakistan might consider reviewing how their national emergency action plans address commitment, management, and oversight by provincial and district authorities, as well as cross-border transmission of WPV and the safety of vaccination teams in insecure areas.
FIGURE 1. Number of cases of wild poliovirus types 1 (WPV1) and 3 (WPV3), by month — Afghanistan and Pakistan, January 2009–August 2012*
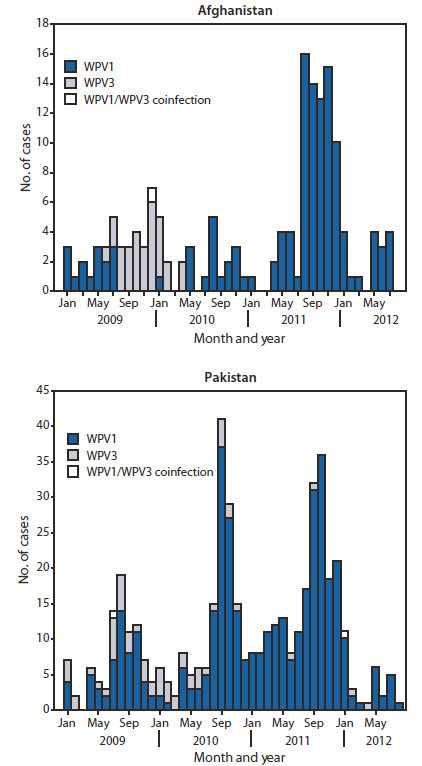
* Data as of September 9, 2012.
Alternate Text: The figure above shows the number of cases of wild poliovirus types 1 (WPV1) and 3 (WPV3), by month, in Afghanistan and Pakistan during January 2009- August 2012. In Afghanistan, 80 WPV1 cases were reported during 2011, compared with 25 WPV cases (17 WPV1, eight WPV3) in 2010; 17 WPV1 cases were reported during January- August 2012, compared with 34 WPV1 cases during the same period in 2011. In Pakistan, 198 WPV cases (196 WPV1, two WPV3) were reported during 2011, compared with 144 WPV cases (120 WPV1, 24 WPV3) during 2010; 30 WPV cases (27 WPV1, two WPV3, and one case with isolation of both WPV1 and WPV3) were reported during January-August 2012, compared with 88 during the same period in 2011.
FIGURE 2. Cases of wild poliovirus types 1 (WPV1) and 3 (WPV3) — Afghanistan and Pakistan, January 2011–August 2012
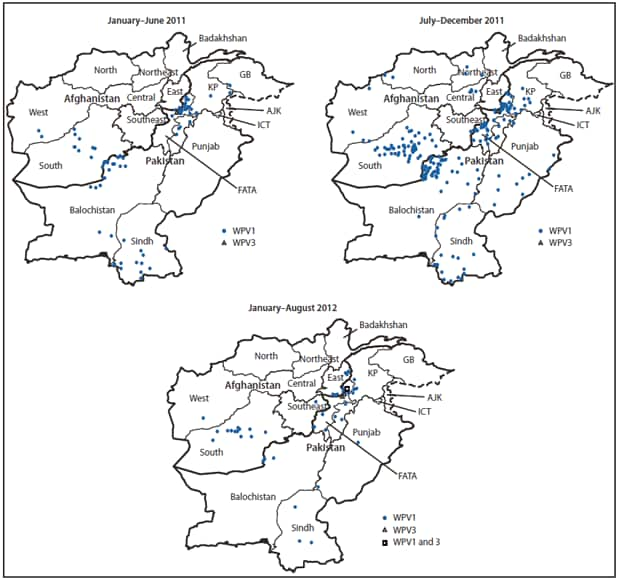
Abbreviations: AJK = Azad Jammu and Kashmir; FATA = Federally Administered Tribal Areas; GB = Gilgit-Baltistan; ICT = Islamabad Capital Territory; KP = Khyber Pakhtunkhwa (formerly Northwest Frontier Province).
Alternate Text: The figure above shows cases of wild poliovirus types 1 (WPV1) and 3 (WPV3) in Afghanistan and Pakistan during January 2011-August 2012. In Afghanistan, 80 WPV1 cases were reported during 2011, compared with 25 WPV cases (17 WPV1, eight WPV3) in 2010; 17 WPV1 cases were reported during January-August 2012, compared with 34 WPV1 cases during the same period in 2011. In Pakistan, 198 WPV cases (196 WPV1, two WPV3) were reported during 2011, compared with 144 WPV cases (120 WPV1, 24 WPV3) during 2010; 30 WPV cases (27 WPV1, two WPV3, and one case with isolation of both WPV1 and WPV3) were reported during January-August 2012, compared with 88 during the same period in 2011.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
