Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Injuries from Ingestion of Wire Bristles from Grill-Cleaning Brushes — Providence, Rhode Island, March 2011–June 2012
On July 3, 2012, this report was posted as an MMWR Early Release on the MMWR website (http://www.cdc.gov/mmwr).
Foreign object ingestion is a common reason for visiting an emergency department (ED), particularly for children (1–3). In recent years, internal injuries have been reported following unintentional ingestions of wire grill-cleaning brush bristles by both children and adults (4–6). A series of six cases from a single hospital system with two EDs during July 2009–November 2010 was reported previously (4). This report describes a series of six more cases identified at the same hospital system during March 2011–June 2012. The six patients ranged in age from 31 to 64 years; five were men. Like the patients in the previous series (4), all six reported outdoor residential food grilling and use of commercially available wire grill-cleaning brushes. The severity of injury ranged from puncture of the soft tissues of the neck, causing severe pain on swallowing, to perforation of the gastrointestinal tract requiring emergent surgery. Awareness of this potential injury among health-care professionals is critical to facilitate timely diagnosis and treatment. Additionally, awareness among the public, manufacturers who make wire grill-cleaning brushes, and retailers who sell these products can reduce exposures and decrease the likelihood of further occurrences. Before cooking, persons should examine the grill surface carefully for the presence of bristles that might have dislodged from the grill brush and could embed in cooked food. Alternative residential grill-cleaning methods or products might be considered.
The first of the six most recent cases was identified on March 14, 2011, and the latest on June 3, 2012. Medical staff members continue to conduct surveillance for additional cases of injury from ingested wire grill-cleaning brush bristles treated in the hospital system.
Case Reports
A man aged 50 years arrived at the ED with abdominal pain that had begun after eating steak at a backyard barbeque. Computed tomography (CT) scan of the abdomen and pelvis revealed a linear object extending through the wall of a loop of small intestine into the omentum (Figure). Laparotomy was performed to remove the foreign body, which appeared to be a wire bristle from a grill-cleaning brush. The patient fully recovered and was discharged the next day.
Five more patients visited the ED during August 2011–June 2012 after inadvertent ingestion of a wire bristle that had become dislodged from a grill-cleaning brush and embedded in food. In all of the cases, the bristles were initially identified by radiographs of the neck or CT scans of the abdomen and pelvis, and their origin was confirmed after removal (Table). Patient interviews revealed a common history of recent ingestion of grilled meat. After definitive treatment, all six patients recovered fully.
Severe pain on swallowing was the chief symptom in three of the six patients. In all three of these patients, a wire bristle from a grill-cleaning brush was found in the neck. The three included a woman aged 46 years and two men aged 50 and 64 years (Table). The three initially were evaluated with plain radiography, which identified the foreign object in each patient. One who was initially evaluated with plain radiography then underwent CT for precise localization. All three were treated successfully with laryngoscopic removal of the wire bristle.
Severe abdominal pain was the chief symptom of the other patients, who were three men aged 31, 35, and 50 years (Table). These patients were evaluated primarily with intravenous contrast-enhanced CT of the abdomen and pelvis. In two patients, the wire bristle was noted lodged within the omentum adjacent to a loop of small intestine. In one patient, the wire bristle was located within the sigmoid colon, indenting the bladder. Two patients underwent emergency abdominal surgery to retrieve the foreign object and repair the intestine. In one patient, the wire had not perforated the intestine and was removed via colonoscopy.
Reported by
David J. Grand, MD, Thomas K. Egglin, MD, William W. Mayo-Smith, MD, and John J. Cronan, MD, Dept of Diagnostic Imaging, Warren Alpert School of Medicine, Brown Univ, Providence, Rhode Island. Corresponding contributor: David J. Grand, dgrand@lifespan.org, 401-444-6421.
Editorial Note
Foreign object ingestion resulted in approximately 80,000 ED visits in 2010 (1); the vast majority occurred in children (1,2). Serious morbidity from foreign object ingestion occurs in <1% of ED cases (3). Prior to 2012, two case reports described perforation of the upper gastrointestinal tract secondary to ingestion of a wire bristle from a grill-cleaning brush. In both patients, perforation resulted in abscess formation, one in a sublingual and one in a paraesophageal location (5,6). This report, like an earlier report from the same hospital system (4), suggests that such incidents might be more common than previously suspected. The continued occurrence of injuries from ingested wire bristles warrants further investigation and action.
Actions to prevent these injuries include increasing awareness among consumers, manufacturers, retailers, and medical professionals to promote prevention, timely diagnosis, and appropriate treatment. Additionally, the Consumer Product Safety Commission (CPSC) currently is reviewing available grill-cleaning brush–related injury data to determine if an identifiable pattern of product defect could pose an unreasonable risk for injury or death, necessitating a consumer warning, product recall, or other regulatory action.
With the summer grilling season under way, broad awareness of the risk will help ED physicians, internists, and radiologists to quickly and appropriately diagnose this injury. These bristles are small, and can be quite difficult to visualize on plain radiographs and CT. If necessary, CT scans of the abdomen and pelvis should be performed without oral contrast, which can obscure the wire bristle. Clinical history is critical so that radiologic evaluation can be tailored to pinpoint the location of the wire (and potential complications) for the appropriate intervention. Additionally, public awareness might result in careful examination of any grill surface before use or use of alternative grill-cleaning methods or products. Awareness by manufacturers and retailers might encourage alteration of current products or development of safer ones for consumer use. Finally, those in the food services industry should examine whether their patrons are at risk for this injury.
Detailed information on the types and brands of grill-cleaning brushes was not available; therefore, recommendations regarding which brands might be safer overall or less likely to lose their bristles could not be made. Questions remain regarding whether different brands or designs of grill-cleaning brushes, different grill types (e.g., uncoated cast iron versus porcelain-coated cast iron), different types of food (e.g., whole cuts of meat versus patties), or different health conditions (e.g., dentures or other oral conditions) make a difference in the risk for ingestion of wire bristles.
Physician awareness of this potential injury is critical to facilitate timely diagnosis and treatment. Awareness of this potential injury by the general population, manufacturers, and retailers can reduce exposures and decrease the likelihood of occurrence. Careful examination of the grill surface before grilling or use of alternative grill-cleaning methods or products are advisable. To improve monitoring of this injury mechanism, medical professionals or consumers should report these injuries to CPSC at http://www.saferproducts.gov.
Acknowledgment
Julie Gilchrist, MD, Div of Unintentional Injury Prevention, National Center for Injury Prevention and Control, CDC.
References
- Consumer Product Safety Commission. National Electronic Injury Surveillance System). Washington, DC: Consumer Product Safety Commission; 2012. Available at http://www.cpsc.gov/library/neiss.html.
- Chen MK, Beierle EA. Gastrointestinal foreign bodies. Pediatr Ann 2001;30:736–42.
- Dahshan A. Management of ingested foreign bodies in children. J Okla State Med Assoc 2001;94:183–6.
- Grand DJ, Cloutier DR, Beland MD, Mayo-Smith WW. Inadvertent ingestion of wire bristles from a grill cleaning brush: radiologic detection of unsuspected foreign bodies. AJR Am J Roentgenol 2012;198:836–9.
- Boon M, Pribitkin E, Spiegel J, Nazarian L, Herbison GJ. Lingual abscess from a grill cleaning brush bristle. Laryngoscope 2009;199:79–81.
- Campisi P, Setwart C, Forte V. Penetrating esophageal injury by ingestion of a wire bristle. J Pediatr Surg 2005;40:e15–6.
What is already known on this topic?
Case reports and one case series have been published describing the risk from unintentional ingestion of wire bristles from grill-cleaning brushes.
What is added by this report?
This case series presents an additional six cases during a 17-month period from a single hospital system. The two case series together document that this risk continues and suggest that this injury mechanism might be more common than suspected previously.
What are the implications for public health practice?
Persons who grill should be aware of the risk for ingestion of wire bristles from grill-cleaning brushes. They should examine their grills or consider alternative methods or products for grill cleaning to reduce exposure and potential injury. Medical professionals need to be aware of this injury to facilitate appropriate diagnosis and treatment.
FIGURE. Axial and coronal images (A, B) from intravenous contrast-enhanced computed tomography show a wire grill-cleaning brush bristle in the omentum (arrows), surrounded by soft tissue stranding (inflammation); a specimen radiograph (C) from omental resection confirms complete foreign object retrieval (arrow).
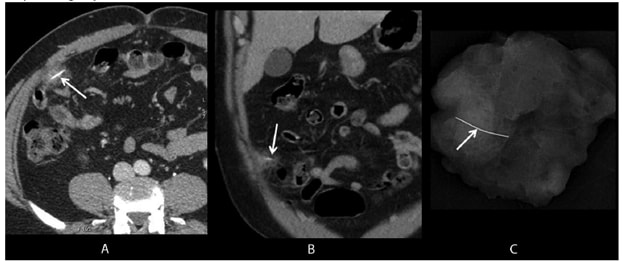
Alternate Text: The figure above consists of three images. The first two are axial and coronal images from intravenous contrast-enhanced computed tomography showing a wire grill-cleaning brush bristle in the omentum, surrounded by soft tissue stranding (inflammation). The third image is a specimen radiograph from omental resection that confirms complete foreign object removal.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
