Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Measles Outbreak Associated with an Arriving Refugee — Los Angeles County, California, August–September 2011
Measles is a highly communicable, acute viral illness with potential for severe complications, including death. Although endemic measles was eliminated in the United States in 2000 as a result of widespread vaccination, sporadic measles outbreaks still occur, largely associated with international travel from measles-endemic countries and pockets of unvaccinated persons (1). On August 26, 2011, the Los Angeles County Department of Public Health (LACDPH) was notified of suspected measles in a refugee from Burma who had arrived in Los Angeles, California, on August 24, after a flight from Kuala Lumpur, Malaysia. Passengers on the flight included 31 other refugees who then traveled to seven other states, widening the measles investigation and response activities (2). In California alone, 50 staff members from LACDPH and the California Department of Public Health (CDPH) interviewed and reinterviewed 298 contacts. Measles was diagnosed in three contacts of the index patient (patient A). The three contacts with measles were two passengers on the same flight as patient A and a customs worker; no secondary cases were identified. Delayed diagnosis of measles in patient A and delayed notification of health officials precluded use of measles-mumps-rubella (MMR) vaccine as an outbreak intervention. This outbreak emphasizes the importance of maintaining a high level of vaccination coverage and continued high vigilance for measles in the United States, particularly among incoming international travelers; clinicians should immediately isolate persons with suspected measles and promptly report them to health authorities.
Case Reports
Patient A. On August 26, LACDPH was notified of a suspected measles case in an adolescent boy (patient A) at a local hospital. Patient A was a newly arrived refugee aged 15 years with no documented measles vaccination who had experienced a fever on August 21, followed by a rash on August 22 (Figure). He had not reported his symptoms to an International Organization for Migration (IOM) medical provider in Malaysia. The patient's accompanying family members (his mother and two brothers, aged 13 and 16 years) were asymptomatic. Although the patient's older brother had a febrile rash illness on August 18, he was healthy at the time of travel. The family had departed Malaysia for Los Angeles International Airport on August 24, arriving the same day; an IOM medical officer also was on the flight. On arrival, the family and other refugees were bused to a local motel.
The following morning, patient A's ongoing symptoms prompted ambulance transfer to a local emergency department (ED), where he remained, not in isolation, for approximately 8 hours. That evening he was transported by ambulance to another hospital ED, where he was isolated when measles was suspected. LACDPH was notified on August 26, and patient A's family members were instructed to isolate themselves at the motel. Although dengue fever was suspected at both EDs, on August 30 the patient was confirmed to have measles by serology and nucleic acid amplification testing (NAAT) performed by CDPH. Serologic testing of his older brother (who also had no documented measles vaccination) also indicated recent measles infection. Patient A's symptoms resolved, and he was discharged on September 1. He and his family members, who remained asymptomatic, were cleared to travel to Wisconsin the next day in accordance with their resettlement plan.
LACDPH and CDPH interviewed 97 contacts of patient A, including family members, fellow passengers on the flight and bus, ambulance staff members, motel guests, Los Angeles-based IOM staff members, and contacts at both EDs. Contacts were interviewed regarding their measles history, immunocompromised status, recent air travel, and current symptoms consistent with measles. Contacts were reinterviewed repeatedly during the 21-day incubation period following their potential measles exposure to assess for development of symptoms consistent with measles. Contacts also were asked to provide proof of measles immunity; if documentation could not be provided, health officials arranged for serologic tests to be performed. Among the 97 contacts, laboratory testing at LACDPH and CDPH identified three cases that met the National Notifiable Diseases Surveillance System measles case definition (3). Viral genotyping confirmed that all four patients were infected with viruses of genotype D9, a type commonly circulating in Malaysia (4).
Patient B. On the August 24 Kuala Lumpur–Los Angeles flight, a U.S.-born girl aged 12 months (patient B) was seated nine rows from patient A; she had boarded the plane during a stopover in Taiwan, which has low measles incidence. Patient B's first MMR vaccine dose was administered at a routine well-baby evaluation near her home in Los Angeles County on August 29, 5 days after arrival. She had a fever the next day, followed by a rash on August 31. Measles was confirmed by NAAT on September 9. Twelve contacts of patient B, including family members and pediatrician office contacts, were interviewed during the resulting contact investigation.
Patient C. Also seated nine rows from patient A on the August 24 Kuala Lumpur–Los Angeles flight was an unvaccinated, Indonesia-born girl aged 19 months (patient C) who was visiting family members in Los Angeles County. On August 30, patient C's family was instructed to remain under home quarantine, given the girl's known measles exposure. Patient C then had a fever on September 1, but her family did not report this symptom to LACDPH during an interview that day, nor was it disclosed that on the same day, patient C and her parents were traveling by chartered bus to Las Vegas, Nevada. Patient C and her family stayed at two Las Vegas hotels before returning to Los Angeles by rental car on September 3 (the same day patient C developed a rash) and attending church the next day. On September 6, a family member reported patient C's symptoms and the recent Las Vegas trip to LACDPH officials. Despite repeated LACDPH instructions to remain at home, patient C and her family visited a pediatrician on September 7. Measles was confirmed on September 9 by NAAT. Patient C could have been exposed to measles in Indonesia, where genotype D9 also circulates (4), but her exposure to a known case and timing of illness made transmission from patient A more likely. LACDPH investigated 79 contacts of patient C, including family members, chartered bus passengers, church attendees, and pediatrician office contacts. A separate investigation of Las Vegas contacts was conducted by Nevada health officials; details from that investigation are not included in this report.
Patient D. Processing patient A on his arrival at the airport on August 24 was a U.S. Customs and Border Protection officer (patient D) aged 25 years, who developed a fever on September 3 and a rash on September 6. He visited a local ED, where measles was suspected. Measles was confirmed on September 9 by NAAT. Patient D had no documented history of MMR vaccination. Serology was positive for measles immunoglobulin G and immunoglobulin M on September 13, although rubella immunoglobulin G was negative, indicating either no previous MMR vaccination or an inadequate immunologic response. Although infectious and experiencing a fever, patient D reported to work during September 2–4. A total of 110 contacts of patient D were interviewed, including family members, friends, employees at a restaurant where patient D dined while ill, hospital contacts, and airport employees. A national alert was posted on CDC's for travelers processed by patient D while he was infectious. Five other customs officers reported measles-like prodromal illness, which was not confirmed as measles but required LACDPH investigation and resulted in time off from work.
Reported by
Dulmini Kodagoda, MPH, Alvin Nelson El Amin, MD, Vi Nguyen, MPH, Immunization Program, Los Angeles County Dept of Public Health. John Holguin, MPH, Long Beach Dept of Health and Human Svcs. Jennifer Zipprich, PhD, Kathleen Harriman, PhD, Kathleen Winter, MPH, John Talarico, DO, Debra Wadford, PhD, Chris Preas, California Dept of Public Health. Christina Mikosz, MD, EIS Officer, CDC. Corresponding contributor: Christina Mikosz, cmikosz@cdc.gov, 213-240-7941.
Editorial Note
Measles, which is spread via the respiratory route, including airborne transmission, is a highly infectious disease. Two doses of MMR vaccine, a highly effective regimen (>95%) in preventing measles, are recommended routinely for children and for certain adults who lack evidence of measles immunity and who are at greater risk for exposure, including health-care personnel, international travelers, and students at post–high school educational institutions (5). In the United States, a first dose of MMR vaccine routinely is recommended for children at age 12–15 months, with a booster dose at age 4–6 years. However, because of the increased risk for exposure, a first dose is recommended at age 6–11 months for infants who will be traveling internationally, followed by a second dose at 12–15 months and the booster at age 4–6 years (6).
A gap in refugee vaccination policy was identified during this investigation. Recent measles outbreaks have been associated with international travel by unvaccinated, infectious travelers (7–10), who can include refugees. Los Angeles International Airport is a major U.S. port of entry for international travelers, processing approximately 5 million arriving international passengers during 2010,* including refugees. Existing regulations do not require refugees to receive any vaccine before U.S. arrival, but the outbreak described in this report might have been prevented if patient A and his family members had received measles vaccination before emigration. In response to this outbreak, MMR vaccine now is being provided for refugees traveling from Malaysia to the United States (2).
This outbreak also identified potential gaps in immunization requirements of workers who interact with arriving refugees. Documentation of employee measles immunity is not uniformly required for employment as a federal airport officer. Having an employee vaccination policy in place with implementation oversight could be beneficial in increasing immunization coverage and reducing transmission of vaccine-preventable diseases among workers who routinely are exposed to incoming international travelers. In 2007, a Detroit airport officer contracted measles from an ill international traveler and possibly transmitted it to another airport worker (8), underscoring that disease transmission can occur at any international airport.
Delays in reporting of patient A to LACDPH contributed to this outbreak. CDC requires that certain illnesses noted during travel, including fever and rash, be reported by airline staff members to the quarantine station with jurisdiction; federal airport staff members also are requested to report this information. The index patient had onset of fever on August 21 and onset of rash on August 22. However, the CDC Los Angeles Quarantine Station was not notified of an ill passenger on the August 24 flight from Malaysia. LACDPH was not informed of the suspected measles case until 2 full days after patient A had arrived in the United States and spent time in a major airport, motel, and hospital ED while infectious. Dengue fever had been considered as a diagnosis before measles. Earlier suspicion and reporting of measles to health officials might have limited the extent of community exposure to measles, enabled provision of MMR vaccination to contacts without evidence of measles immunity, and allowed health officials to enhance surveillance sooner. Measles should be considered in the differential diagnosis for any patient with a febrile rash illness with recent international travel; patients with suspected measles should be reported immediately to local public health authorities and isolated until measles is ruled out.
Acknowledgments
Michelle T. Parra, PhD, Immunization Program, Laurene Mascola, MD, David Dassey, MD, Acute Communicable Disease Control Program, Los Angeles County Dept of Public Health; Regina Chase, Giorgio Cosentino, Barryett Enge, MS, Alex Espinosa, MS, Ashraf Fadol, Carlos Gonzalez, Oliver Oyler, Larry Penning, Pat Stoll, MD, Viral and Rickettsial Disease Laboratory, California Dept of Public Health. Div of Global Migration and Quarantine; Diana Bensyl, PhD, Scientific Education and Professional Development Program Office, Office of Surveillance, Epidemiology, and Laboratory Svcs, CDC.
References
- Parker Fiebelkorn A, Redd SB, Gallagher K, et al. Measles in the United States during the postelimination era. J Infect Dis 2010;202:1520–8.
- CDC. Notes from the field: measles among U.S.-bound refugees from Malaysia—California, Maryland, North Carolina, and Wisconsin, August–September 2011. MMWR 2011;60:1281–2.
- CDC. National Notifiable Diseases Surveillance System: measles 2010 case definition. Atlanta, GA: US Department of Health and Human Services, CDC; 2010. Available at http://www.cdc.gov/osels/ph_surveillance/nndss/casedef/measles_2010.htm. Accessed May 25, 2012.
- Rota P, Brown K, Mankertz A, et al. Global distribution of measles genotypes and measles molecular epidemiology. J Infect Dis 2011;204(Suppl 1):S514–23.
- CDC. Measles, mumps, and rubella—vaccine use and strategies for elimination of measles, rubella, and congenital rubella syndrome and control of mumps: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 1998;47(No. RR-8).
- CDC. Measles imported by returning U.S. travelers aged 6–23 months, 2001–2011. MMWR 2011;60:397–400.
- CDC. Notes from the field: measles outbreak—Indiana, June–July 2011. MMWR 2011;60:1169.
- Chen T-H, Kutty P, Lowe L, et al. Measles outbreak associated with an international youth sporting event in the United States, 2007. Pediatr Infect Dis J 2010;29:794–800.
- CDC. Notes from the field: multiple cases of measles after exposure during air travel—Australia and New Zealand, January 2011. MMWR 2011;60:851.
- CDC. Notes from the field: measles outbreak—Hennepin County, Minnesota, February–March 2011. MMWR 2011;60:421.
* Additional information at http://www.lawa.org.
What is already known on this topic?
Widespread use of measles-mumps-rubella (MMR) vaccine has resulted in elimination of indigenous measles circulation in the United States. However, sporadic outbreaks of measles continue to occur in the United States, typically linked to imported cases from countries where measles remains endemic.
What is added by this report?
An ill passenger arriving in Los Angeles from Malaysia was linked to cases of measles in two passengers on the same flight and a U.S. Customs and Border Protection officer. The index patient had never been vaccinated against measles and was emigrating to the United States. Fifty health officials interviewed 298 contacts in the resulting investigation. Delayed diagnosis and notification of health officials precluded the use of MMR vaccination for outbreak containment.
What are the implications for public health practice?
Measles should be considered in the differential diagnosis of any febrile rash illness in a patient with recent international travel; in suspected cases, health authorities should be notified immediately and the patient isolated. Widespread MMR vaccination is a highly effective way to limit illness and complications from measles.
FIGURE. Timeline for onset of fever and rash and laboratory confirmation of measles in patient A and three contact patients (B, C, and D) — Los Angeles County, California, August–September 2011
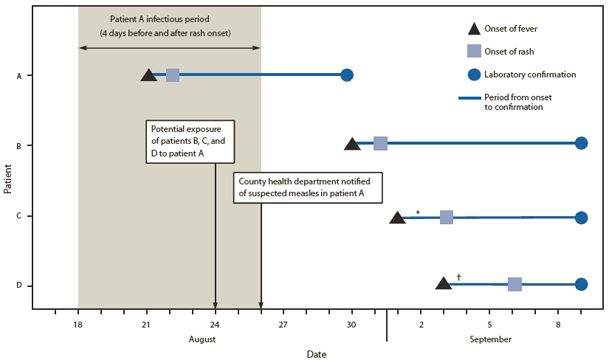
* Patient C traveled out of state during September 1–3, while infectious.
† Patient D reported to work during September 2–4, while infectious.
Alternate text: The figure above shows the timeline for onset of fever and rash and laboratory confirmation of measles in patient A and contact patients B, C, and D, after a flight from Kuala Lumpur to Los Angeles International Airport in August 2011. Patient A arrived at the airport August 24, 3 days after onset of fever and two days after onset of rash. His measles was confirmed on August 30. Measles was confirmed in the three contacts on September 9.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
