Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Trends in Tuberculosis — United States, 2011
Please note: An erratum has been published for this article. To view the erratum, please click here.
In 2011, a total of 10,521 new tuberculosis (TB) cases were reported in the United States, an incidence of 3.4 cases per 100,000 population, which is 6.4% lower than the rate in 2010. This is the lowest rate recorded since national reporting began in 1953 (1). The percentage decline is greater than the average 3.8% decline per year observed from 2000 to 2008 but not as large as the record decline of 11.4% from 2008 to 2009 (2). This report summarizes 2011 TB surveillance data reported to CDC's National Tuberculosis Surveillance System. Although TB cases and rates decreased among foreign-born and U.S.-born persons, foreign-born persons and racial/ethnic minorities continue to be affected disproportionately. The rate of incident TB cases (representing new infection and reactivation of latent infection) among foreign-born persons in the United States was 12 times greater than among U.S.-born persons. For the first time since the current reporting system began in 1993, non-Hispanic Asians surpassed persons of Hispanic ethnicity as the largest racial/ethnic group among TB patients in 2011. Compared with non-Hispanic whites, the TB rate among non-Hispanic Asians was 25 times greater, and rates among non-Hispanic blacks and Hispanics were eight and seven times greater, respectively. Among U.S.-born racial and ethnic groups, the greatest racial disparity in TB rates occurred among non-Hispanic blacks, whose rate was six times the rate for non-Hispanic whites. The need for continued awareness and surveillance of TB persists despite the continued decline in U.S. TB cases and rates. Initiatives to improve awareness, testing, and treatment of latent infection and TB disease in minorities and foreign-born populations might facilitate progress toward the elimination of TB in the United States.
Health departments in the 50 states and the District of Columbia electronically report to CDC verified TB cases that meet the CDC and Council of State and Territorial Epidemiologists surveillance case definition.* Reports include the patient's self-identified race, ethnicity (i.e., Hispanic or non-Hispanic), human immunodeficiency virus (HIV) status, treatment information, and drug-susceptibility test results. CDC calculates national and state TB rates overall and by racial/ethnic group, using U.S. Census Bureau population estimates (3). As of March 22, 2012, race/ethnicity intercensal population estimates were unavailable for 2011; therefore, 2010 population estimates were used as denominators to calculate 2011 case rates. The Current Population Survey provides the population denominators used to calculate TB rates and percentage changes according to national origin.† Because 2011 Current Population Survey data were available, 2011 population estimates were used for U.S.-born and foreign-born TB rates. For TB surveillance, a U.S.-born person is defined as someone born in the United States or its associated jurisdictions, or someone born in a foreign country but having at least one U.S.-citizen parent. In 2011, 0.4% of patients had unknown country of birth, and 0.7% had unknown race or ethnicity. For this report, persons of Hispanic ethnicity might be of any race; non-Hispanic persons are categorized as black, Asian, white, American Indian or Alaska Native, Native Hawaiian or other Pacific Islander, or of multiple races.
Compared with the national TB case rate of 3.4 cases per 100,000 population, TB rates in reporting areas ranged widely, from 0.7 in Maine to 9.3 in Alaska (median: 2.4) (Figure 1). Thirty-four states had lower rates in 2011 than in 2010; 16 states and the District of Columbia had higher rates. As in 2010, four states (California, Florida, New York, and Texas) continued to report more than 500 cases each in 2011. Combined, these four states accounted for 5,299 TB cases or approximately half (50.4%) of all TB cases reported in 2011.
Among U.S.-born persons, the number and rate of TB cases declined in 2011. The 3,929 TB cases in U.S.-born persons (37.5% of all cases in persons with known national origin) represented a 9.9% decrease compared with 2010 and a 77.5% decrease compared with 1993 (Figure 2). The rate of 1.5 TB cases per 100,000 population among U.S.-born persons represented a 10.3% decrease since 2010 and an 80.1% decrease since 1993.
The difference between the proportion of U.S.-born and foreign-born persons with TB continued to increase, although the number and rate of TB cases among foreign-born persons in the United States declined in 2011. A total of 6,546 TB cases were reported among foreign-born persons (62.5% of all cases in persons with known national origin), a 3.0% decrease from 2010. The 17.3 per 100,000 population TB rate among foreign-born persons was a 4.8% decrease since 2010 and a 49.0% decrease since 1993. In 2011, 54.1% of foreign-born persons with TB originated from five countries: Mexico (n = 1,392 [21.3%]), the Philippines (n = 750 [11.5%]), Vietnam (n = 537 [8.2%]), India (n = 498 [7.6%]), and China (n = 365 [5.6%]).
During the past 12 years, the proportion of TB cases occurring in Asians has increased steadily, from 20.5% in 2000 to 29.9% in 2011. More TB cases were reported among Asians than any other racial/ethnic group in the United States in 2011 (Table). From 2010 to 2011, TB rates decreased most for blacks, then Hispanics, whites, and Asians. Among persons with TB, 95.4% of Asians, 73.9% of Hispanics, 36.4% of blacks, and 20.9% of whites were foreign-born. Among U.S.-born persons, blacks were the racial/ethnic group with the greatest percentage of TB cases (38.6%) and the largest disparity compared with U.S.-born whites.
HIV test result reporting improved in 2011, with 81% of cases reported having a known HIV status. Among persons with TB who had a known HIV test result, 7.9% were coinfected with HIV. Vermont data were not available.§
A total of 109 cases of multidrug-resistant TB (MDR TB)¶ were reported in 2010, the most recent year for which complete drug-susceptibility data were available. Drug-susceptibility test results for isoniazid and rifampin were reported for 97.5% and 97.1% of culture-confirmed TB cases in 2009 and 2010, respectively. Among these cases, the percentage of MDR TB for 2010 (1.3% [109 of 8,422]) was unchanged from the percentage for 2009 (1.3%). The percentage of MDR TB cases among persons without a previous history of TB has remained stable at approximately 1.0% since 1997. For persons with a previous history of TB, the percentage with MDR TB in 2010 was approximately four times greater than among persons not previously treated for TB. In 2010, foreign-born persons accounted for 90 (82.6%) of the 109 MDR TB cases. Four cases of extensively drug-resistant TB** (all occurring in foreign-born persons) have been reported for 2011.
Reported by
Roque Miramontes, MPH, Robert Pratt, Sandy F. Price, Carla Jeffries, MPH, Thomas R. Navin, MD, Div of TB Elimination, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention; Gloria E. Oramasionwu, MD, EIS Officer, CDC. Corresponding contributor: Gloria E. Oramasionwu, iyo8@cdc.gov, 404-718-8633.
Editorial Note
Despite the continued decline in U.S. TB cases and rates since 1993, the 6.4% decline from 2010 to 2011 to a rate of 3.4 per 100,000 falls short of the 2010 goal of TB elimination (less than one case per 1,000,000) set in 1989 (4). If current efforts are not improved or expanded, TB elimination is unlikely before the year 2100 (5).
In 2011, Asians became the largest single racial/ethnic group represented among TB cases, with a case rate 25 times that of non-Hispanic whites. Although the case rate among Asians declined in 2011 compared with 2010, this 0.6% decline was smaller than among any other racial/ethnic group. This finding underscores the need for increased TB awareness and prevention programs in Asian communities. A decrease in TB rates was associated with one such program, implemented in predominantly black and Hispanic neighborhoods in Texas, which raised TB awareness in the community while also treating anyone found to have latent TB infection (LTBI) (6). Moreover, because 95% of Asians with TB in 2011 were foreign-born, further support of global TB control will be important for reducing TB rates.
Addressing the increasing difference between TB rates in foreign-born and U.S.-born persons is critical for TB elimination. Most foreign-born persons with TB (78.8%) had their TB diagnosed after being in the United States for more than 2 years,†† consistent with reactivation of LTBI acquired abroad. Therefore, treating LTBI will be critical for accelerating the TB decline among foreign-born persons (5). In 2007, CDC published technical instructions for TB screening in prospective immigrants to the United States (7). As more high-TB burden countries adopt these technical instructions, screening and treating immigrants should improve. Persons screened overseas and found to have LTBI should receive preventive TB treatment upon arrival in the United States. A new, shorter regimen for LTBI requiring just 12 once-weekly drug administrations has been recommended by CDC and might result in better adherence to LTBI treatment in foreign-born and U.S.-born populations (8,9).
Approximately 81% of TB cases in 2011 had known HIV status at TB diagnosis. This increase (66.3% in 2010) is attributed to increased reporting from selected regions. The American Thoracic Society and the Infectious Disease Society of America recommend that all TB patients be counseled and tested for HIV (10).
This analysis is limited to reporting provisional TB cases and case rates for 2011. Case rates are based on estimates of population denominators from either 2010 or 2011. CDC's annual TB surveillance report will provide final TB case rates based on updated denominators later this year.
Progress toward TB elimination in the United States will require ongoing surveillance and improved TB control and prevention activities. Sustained focus on domestic TB control activities and further support of global TB control initiatives is important to address persistent disparities between non-Hispanic whites and racial/ethnic minorities and between U.S.-born and foreign-born persons.
Acknowledgments
State and local TB control officials.
References
- CDC. Reported tuberculosis in the United States, 2010. Atlanta, GA: US Department of Health and Human Services, CDC; 2011. Available at http://www.cdc.gov/tb/statistics/reports/2010/default.htm. Accessed February 21, 2012.
- CDC. Decrease in reported tuberculosis cases—United States, 2009. MMWR 2010;59:289–94.
- US Census Bureau. Current estimates data. Available at http://www.census.gov/popest/data/national/totals/2011/index.html. Accessed February 2, 2012.
- CDC. A strategic plan for the elimination of tuberculosis in the United States. MMWR 1989;38(No. S-3).
- Hill AN, Becerra JE, Castro KG. Modelling tuberculosis trends in the USA. Epidemiol Infect 2012:1–11.
- Cegielski JP, Griffith DE, McGaha PK, et al. Eliminating tuberculosis, one neighborhood at a time. Am J Public Health 2012 (In press).
- CDC. CDC immigration requirements: technical instructions for tuberculosis screening and treatment. Using cultures and directly observed therapy. US Department of Health and Human Services, CDC; 2009. Available at http://www.cdc.gov/immigrantrefugeehealth/pdf/tuberculosis-ti-2009.pdf. Accessed February 16, 2012.
- Sterling TR, Villarino ME, Borisov AS, et al. Three months of rifapentine and isoniazid for latent tuberculosis infection. N Engl J Med 2011;365:2155–66.
- CDC. Recommendations for use of an isoniazid-rifapentine regimen with direct observation to treat latent Mycobacterium tuberculosis infection. MMWR 2011;60:1650–3.
- CDC. Treatment of tuberculosis. American Thoracic Society, CDC, and Infectious Diseases Society of America. MMWR 2003;52(No. RR-11).
* Available at http://www.cdc.gov/osels/ph_surveillance/nndss/casedef/tuberculosis_current.htm.
† Additional information available at http://dataferrett.census.gov.
§ Vermont no longer reports HIV status of TB patients to CDC.
¶ Defined by the World Health Organization as a case of TB in a person with a Mycobacterium tuberculosis isolate resistant to at least isoniazid and rifampin. Additional information available at http://whqlibdoc.who.int/publications/2010/9789241599191_eng.pdf.
** Defined by the World Health Organization as a case of TB in a person with an M. tuberculosis isolate with resistance to at least isoniazid and rifampin among first-line anti-TB drugs, resistance to any fluoroquinolone (e.g., ciprofloaxacin or ofloxacin), and resistance to at least one second-line injectable drug (e.g., amikacin, capreomycin, or kanamycin). Additional information available at http://whqlibdoc.who.int/publications/2010/9789241599191_eng.pdf.
†† The percentage of foreign-born persons with TB residing in the United States for more than 2 years was based on provisional 2011 National Tuberculosis Surveillance System data accessed on February 22, 2012.
What is already known on this topic?
Although tuberculosis (TB) has been on the decline in the United States since 1993, an increasing proportion of cases has been observed among the foreign-born. Racial and ethnic minorities have represented a higher proportion of cases among the U.S.-born.
What is added by this report?
Provisional 2011 surveillance data indicate a TB case rate of 3.4 cases per 100,000 persons, which is the lowest rate since 1993. For the first time since current reporting began in 1993, Asians have become the most widely represented racial/ethnic group among TB cases, even though case rates also have declined in this group. Reporting of human immunodeficiency (HIV) status at diagnosis has improved in the most recent reporting year, and HIV infection among TB cases is at an all-time low.
What are the implications for public health practice?
Continued awareness and surveillance of TB is needed despite the decline. Initiatives to improve awareness, testing, and treatment of latent infection and TB disease in minorities and foreign-born populations should facilitate progress toward the elimination of TB in the United States.
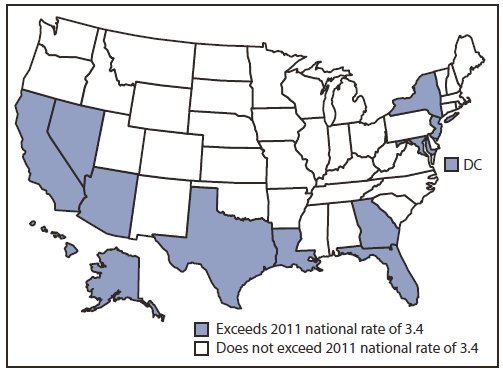
* Per 100,000 population.
† Data are provisional.
Alternate Text: The figure above shows the rate of tuberculosis (TB) cases in the United States, during 2011. Compared with the national TB case rate of 3.4 cases per 100,000 population, TB rates in reporting areas ranged widely, from 0.7 in Maine to 9.3 in Alaska (median: 2.4).
FIGURE 2. Number and rate of tuberculosis (TB) cases among U.S.-born and foreign-born persons, by year reported — United States, 1993–2011*
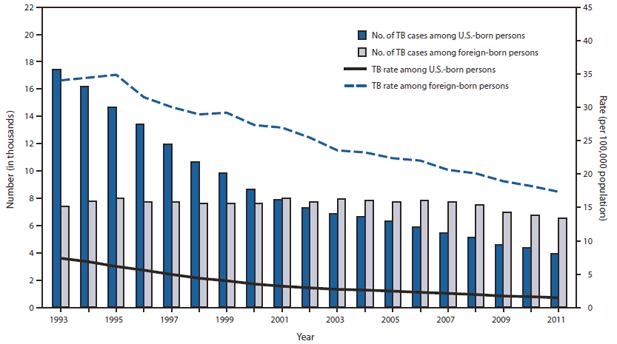
Source: National Tuberculosis Surveillance System.
* Data are updated as of February 22, 2012. Data for 2011 are provisional.
Alternate Text: The figure above shows the number and rate of tuberculosis (TB) cases among U.S.-born and foreign-born persons, by year, reported in the United States during 1993-2011. Among U.S.-born persons, the number and rate of TB cases declined in 2011. The 3,929 TB cases in U.S.-born persons (37.5% of all cases in persons with known national origin) were a 9.9% decrease compared with 2010 and a 77.5% decrease compared with 1993.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
