FIGURE 1. Coverage with 1 dose of measles-containing vaccine among children aged 12--23 months, by district --- India, 2007--2008*
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Progress in Implementing Measles Mortality Reduction Strategies --- India, 2010--2011
In 2005, an estimated 92,000 deaths occurred in India from measles among children aged <5 years (1). Estimates from 2008 indicate that 77% of global measles mortality was attributable to measles deaths in the World Health Organization (WHO) South-East Asia Region, the majority of which occurred in India (2,3). These figures highlight the importance of India in attaining regional and global measles mortality reduction targets. In 2008, the Indian National Technical Advisory Group on Immunization (NTAGI) recommended introduction of a second dose of measles-containing vaccine (MCV2), delivered through routine vaccination in states with ≥80% coverage with the first dose of measles-containing vaccine (MCV1), or through mass vaccination campaigns in states with <80% MCV1 coverage. Based on these recommendations, the government of India initiated MCV2 introduction in late 2010. This report provides an update on MCV1 coverage, progress in implementing MCV2, and measles outbreak surveillance activities conducted in eight states during 2006--2010. India has initiated implementation of a measles mortality reduction strategy, but the pace of implementation is variable across states. Strong national and state leadership and commitment to rapid reduction of measles mortality are essential to achieve the full benefits of this strategy.
Routine MCV1 coverage
In 1985, MCV1 was introduced in the India Expanded Program on Immunization, with a recommended age for vaccination of 9--12 months. Estimated national routine MCV1 coverage was 74% among children aged 12--23 months based on the UNICEF-sponsored national Coverage Evaluation Survey (CES) of 2009 (4); state-level MCV1 coverage ranged from 48% to 96%.* District level data from the District Level Household and Facility Survey conducted during 2007--2008 (DLHS-3) indicated that MCV1 coverage was ≥90% in 26% of the evaluated districts (Figure 1).
MCV2 introduction
Based on NTAGI recommendations, 17 states† with MCV1 coverage ≥80% (according to DLHS-3 data) had introduced single antigen measles vaccine as MCV2 through routine vaccination services during May 2010--August 2011. Four states§ with MCV1 coverage ≥80% had introduced measles, mumps, and rubella vaccine as MCV2 before 2008.
Fourteen states¶ with <80% MCV1 coverage have started introducing MCV2 through mass vaccination campaigns using single antigen measles vaccine and targeting children aged 9 months--10 years (Figure 2). The target age group for campaigns was based on age distribution of cases reported through the measles outbreak surveillance system and investigation of several outbreaks in other states. An estimated 134 million children are targeted to receive MCV2 in these states in phases during 2010--2012. The first phase was conducted during September 2010--July 2011. By selecting a limited number of districts, the first phase was intended to establish best practices and document lessons learned for conducting subsequent larger phases of measles vaccination campaigns in India. The second phase will target 144 districts during September--December 2011. In 2012, a total of 172 districts are expected to be covered. In addition, campaign districts will introduce MCV2 through routine vaccination 6 months after completion of campaign activities.
Results of Phase 1 MCV2 campaigns
During the first phase of MCV2 campaigns, 12,076,836 children were vaccinated in 45 districts of 13 states (all targeted states except Uttar Pradesh). Overall reported administrative coverage** was 86% and exceeded 90% in 18 (40%) of 45 districts. Rapid convenience assessments were conducted by independent monitors during and after the campaign to validate vaccination coverage and assess campaign quality.†† In total, 10,926 areas were assessed, and the campaign vaccination status of 217,512 target-aged children was verified in 43 of 45 districts. Of the assessed areas, 3,946 (36%) had ≥90% children vaccinated, and 3,358 (31%) areas had <80% campaign targeted children vaccinated. In total, 183,965 (85%) of all the assessed children were vaccinated. The most common reasons for nonvaccination, cited by nearly half (48%) of caretakers, were lack of knowledge about 1) the campaign, 2) the location of vaccination sites, or 3) the perceived importance of the activity. No deaths related to adverse events after vaccination were reported.
Measles outbreak surveillance
Laboratory-supported measles outbreak surveillance was initiated in 2006 and, by 2010, was operational in eight states (Andhra Pradesh, Gujarat, Karnataka, Kerala, Madhya Pradesh, Rajasthan, Tamil Nadu, and West Bengal). An outbreak is considered confirmed if measles immunoglobulin M (IgM) is detected in serum from at least two suspected cases. Sera are tested by a network of eight laboratories accredited by the World Health Organization. All samples testing negative for measles IgM are tested for rubella IgM.
During 2010, a total of 242 suspected outbreaks were investigated, and 198 (82%) were laboratory-confirmed as measles (Figure 3). Among 8,984 measles patients from laboratory-confirmed outbreaks, 7% were aged <1 year, 41% were aged 1--4 years, 37% were aged 5--9 years, and 15% were aged ≥10 years.
Reported by
India Ministry of Health and Family Welfare; Stephen Sosler, PhD, Anindya Sekhar Bose, MD, Hamid Jafari, MD, National Polio Surveillance Project, World Health Organization, New Delhi, India. Abhijeet Anand, MBBS, MPH, Eric Wiesen, MA, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Corresponding contributor: Abhijeet Anand, aanand@cdc.gov, 404-639-1970.
Editorial Note
Overall, 77% of global measles mortality in 2008 was attributable to measles deaths in the WHO South-East Asia Region, the majority of which occurred in India. Therefore, MCV2 introduction in India as part of a comprehensive measles mortality reduction strategy is an important step towards achieving the global target of a 95% reduction in global measles deaths in 2015 from the 733,000 measles deaths estimated in 2000. The government of India is demonstrating strong commitment to this effort and is providing full financial support for the purchase of all vaccines and all logistic and operational costs of MCV2 introduction activities.
Routine vaccination is a critical strategy for achieving high coverage with MCV1 and MCV2. The government of India is implementing measures to strengthen routine vaccination, especially in districts with low coverage. Nevertheless, substantial challenges exist, including the need for 1) increasing the number of trained staff at all levels, 2) increasing public demand for and confidence in vaccines, 3) improving vaccine stock and cold chain management, and 4) developing a strong reporting and management system for adverse events after vaccination. In addition, administration of MCV2 through routine vaccination services targets children aged 16--24 months, the same age that a diphtheria, tetanus, and pertussis (DTP) booster is recommended by the national immunization program. National DTP booster coverage (according to CES 2009) was 41%, indicating the need to rapidly increase coverage of vaccines scheduled beyond the first year of life (4). The first phase of the measles vaccination campaigns highlighted important challenges in planning and implementation, including obtaining strong state-level leadership and coordination, timely determination of campaign dates, reaching populations with the campaign messages, and reaching children in urban areas. Success in overcoming these challenges in the subsequent phases will be critical to reducing measles mortality in India.
Past experience with MCV2 introduction through mass campaigns in other countries has demonstrated that a substantial proportion of the susceptible population needs to be vaccinated during a short period to achieve maximum reduction of measles virus transmission (5). Phased subnational campaigns over a longer period might leave pockets of susceptible children, especially among highly mobile populations. In a country as large and mobile as India, the benefits of conducting large-scale campaigns during a short period need to be balanced with the need to ensure safety and high coverage with injectable vaccines. Therefore, a well-considered approach is needed that covers large areas as quickly as possible without jeopardizing quality or safety. The age distribution and vaccination status of measles patients in the eight states currently implementing measles outbreak surveillance demonstrates gaps in immunity, especially among children aged <10 years. Expanding surveillance to obtain information on measles epidemiology in all Indian states will be important. Such information will allow India to quickly identify and respond to outbreaks and will help guide measles control in India. In particular, it will reveal any possible need for campaigns in states with reported routine MCV1 coverage ≥80%.
References
- Kumar R, Awasthi S, Bassani DG, et al. Causes of neonatal and child mortality in India: a nationally representative mortality survey. Lancet 2010;376:1853--60.
- World Health Organization. Global reductions in measles mortality 2000--2008 and the risk of measles resurgence. Wkly Epidemiol Rec 2009;84:509--16.
- CDC. Global measles mortality, 2000--2008. MMWR 2009;58:1321--6.
- United Nations Children's Fund. 2009 Coverage Evaluation Survey. New Delhi, India: United Nations Children's Fund; 2009.
- Ma C, An Z, Hao L, et al. Progress toward measles elimination in the People's Republic of China, 2000--2009. J Infect Dis 2011;204(Suppl 1):S447--54.
* India is comprised of 29 states and six Union Territories.
† Andaman and Nicobar Islands, Andhra Pradesh, Chandigarh, Dadra and Nagar Haveli, Daman and Diu, Himachal Pradesh, Jammu and Kashmir, Karnataka, Kerala, Lakshadweep, Maharashtra, Mizoram, Orissa, Punjab, Tamil Nadu, Uttarakhand, and West Bengal.
§ Delhi, Goa, Sikkim, and the Union Territory of Pondicherry.
¶ Arunachal Pradesh, Assam, Bihar, Chhattisgarh, Gujarat, Haryana, Jharkhand, Madhya Pradesh, Manipur, Meghalaya, Nagaland, Rajasthan, Tripura, and Uttar Pradesh.
** Administrative coverage is calculated by dividing the number of doses administered by the number of persons in the target population.
†† Rapid convenience assessments target identified high-risk populations and areas. In selected areas, 20 households with target-aged children are visited, the campaign vaccination status of children is verified, and reasons for nonvaccination are elicited for unvaccinated children. Unvaccinated children are referred to the nearest vaccination sites. If two or more unvaccinated children are reported from a given area, supervisors are informed, and remedial action is taken.
What is already known on this topic?
An estimated 77% of global measles mortality in 2008 was attributable to measles deaths in the World Health Organization South-East Asia Region, the majority of which occurred in India. Progress in reducing measles mortality in India is critical in achieving the global goal of 95% reduction in measles mortality by 2015 from the estimated 733,000 measles deaths in 2000. Providing 2 doses of measles-containing vaccine to all children is an important step in reducing measles deaths; until recently, India was the only country not to have implemented this measles mortality reduction strategy.
What is added by this report?
In 2010, the government of India initiated introduction of a second dose of measles-containing vaccine (MCV2) delivered through routine vaccination or mass vaccination campaigns. The first phase of the campaign, initiated in September 2010, vaccinated approximately 12 million children of the 134 million in 14 states targeted to receive measles vaccine from campaigns by 2012. MCV2 is now being provided through routine vaccination to all remaining 21 states. The government of India is demonstrating strong commitment to accelerated measles mortality reduction activities.
What are the implications for public health practice?
Introduction of MCV2 in India is an important step in reducing global measles mortality. The first phase of measles campaigns in India have demonstrated substantial challenges in planning and implementing campaigns, such as obtaining strong state-level leadership, having trained staff at all levels, and increasing public demand and confidence in vaccines.
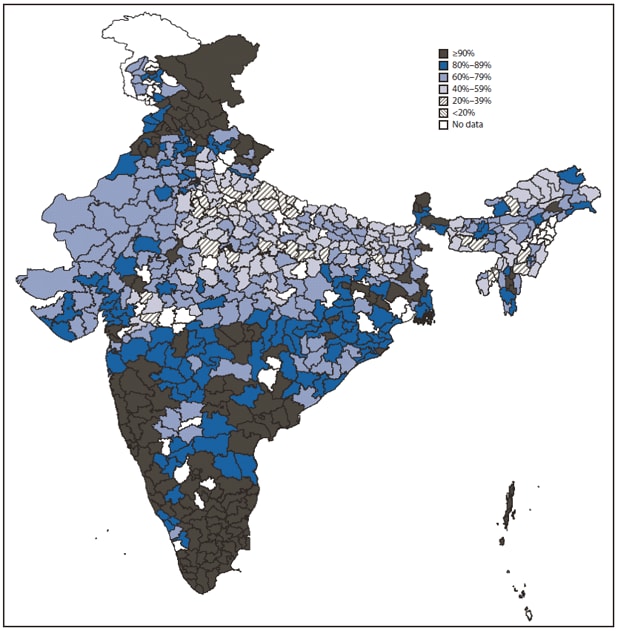
* Data are from the District Level Household and Facility Survey 2007--2008.
Alternate Text: The figure above shows coverage with 1 dose of measles-containing vaccine (MCV1) among children aged 12–23 months, by district, in India during 2007–2008. In 1985, MCV1 was introduced in the India Expanded Program on Immunization, with a recommended age for vaccination of 9–12 months. Estimated national routine MCV1 coverage was 74% among children aged 12–23 months based on the UNICEF-sponsored national Coverage Evaluation Survey of 2009; state-level MCV1 coverage ranged from 48% to 96%. District level data from the District Level Household and Facility Survey conducted during 2007–2008 indicated that MCV1 coverage was ≥90% in 26% of the evaluated districts.
FIGURE 2. Coverage with 1 dose of measles-containing vaccine among children aged 12--23 months, by state --- India, 2007--2008*
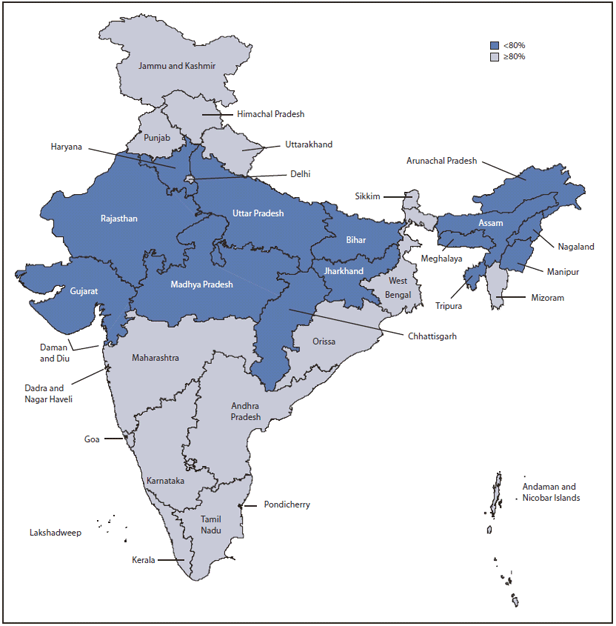
* Data are from the District Level Household and Facility Survey 2007--2008 for all states except Nagaland, for which data are from the UNICEF 2006 Coverage Evaluation Survey.
Alternate Text: The figure above shows coverage with 1 dose of measles-containing vaccine (MCV1) among children aged 12–23 months, by state, in India during 2007–2008. Fourteen states with <80% MCV1 coverage have started introducing MCV2 through mass vaccination campaigns using single antigen measles vaccine and targeting children aged 9 months–10 years.
FIGURE 3. Laboratory-confirmed measles and rubella outbreaks in states conducting measles outbreak surveillance --- India, 2010*
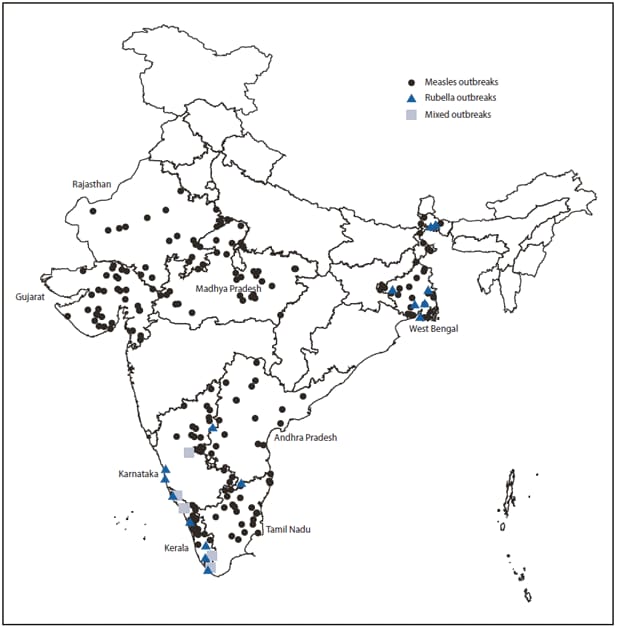
* Data are from the National Polio Surveillance Project measles surveillance database, 2010.
Alternate Text: The figure above shows laboratory-confirmed measles and rubella outbreaks in states conducting measles outbreak surveillance in India during 2010. During 2010, a total of 242 suspected outbreaks were investigated, and 198 (82%) were laboratory-confirmed as measles.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
