FIGURE 1. Average annual antibiotic prescribing rates for physician office--related visits per 1,000 population aged ≤14 years --- National Ambulatory Medical Care Survey, United States, 1993--1994 to 2007--2008
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Office-Related Antibiotic Prescribing for Persons Aged ≤14 Years --- United States, 1993--1994 to 2007--2008
In 2003, the Institute of Medicine identified antibiotic resistance as a key microbial threat to health in the United States and recommended promoting appropriate antibiotic use as an important strategy to address this threat (1). Antibiotic use contributes to development of antibiotic resistance on both the individual and country level (2). To examine trends in pediatric antibiotic prescribing in physician offices, CDC analyzed data from the National Ambulatory Medical Care Survey (NAMCS) for the period 1993--1994 to 2007--2008. This report summarizes the results of that analysis, which found that antibiotic prescribing rates for persons aged ≤14 years who had visited physician offices decreased 24% from 300 antibiotic courses per 1,000 office visits in 1993--1994 to 229 antibiotic courses per 1,000 office visits in 2007--2008. Among the five acute respiratory infections (ARIs) examined, antibiotic prescribing rates decreased 26% for pharyngitis and 19% for nonspecific upper respiratory infection (common cold); prescribing rates for otitis media, bronchitis, and sinusitis did not change significantly. Although the overall antibiotic prescribing rate for persons aged ≤14 years has decreased, the rate remains inappropriately high. Further efforts are needed to decrease inappropriate antibiotic prescribing for persons aged ≤14 years.
NAMCS is a national probability sample survey of visits to nonfederal, office-based physicians conducted annually by CDC. NAMCS samples visits during randomly assigned 1-week reporting periods throughout the year and collects patient demographic information, diagnostic codes for up to three diagnoses, and prescription information from the medical record. Diagnoses of the five ARIs, most episodes of which do not require antibiotic treatment, were identified using the following International Classification of Diseases, Ninth Revision, Clinical Modification codes for the primary diagnosis: 381.0, 381.4, 382.0, 382.4, 382.9 (otitis media); 466.0, 490 (bronchitis); 462, 463 (pharyngitis); 461, 473 (sinusitis); and 460, 465 (nonspecific upper respiratory infection [common cold]). Details of NAMCS methodology have been described previously.* To quantify and assess antibiotic prescribing practices, the first five drug prescriptions recorded for each visit were examined, and the number of antibiotic prescriptions counted. Data were weighted to produce national estimates, and combined in 2-year periods to improve the reliability of estimates.
The population-based antibiotic prescription rate was defined as the average annual number of antibiotic prescriptions recorded for persons aged ≤14 years during the 2-year period, divided by the population aged ≤14 years during the same period. Population denominators were the average of the Census Bureau's postcensal estimates of the civilian, noninstitutionalized population of the United States for each July during the 2-year period (3). The visit-based antibiotic prescription rate was defined as the average annual number of antibiotic prescriptions recorded for persons aged ≤14 years during the 2-year period, divided by the average annual number of physician office visits by persons in that age group during the same period. In addition, an average annual office visit rate, regardless of antibiotic prescribing, was calculated for patients aged ≤14 years. Significance of trends (at p<0.05) was tested by assuming a linear trend in weighted least-squares regression analysis. The two-tailed t-test was used to compare proportions (p<0.05 level of significance).
The number of participating physicians and average annual response rates for each 2-year period of the study ranged from 2,500 to 3,500 and from 62% to 72%, respectively. The number of completed patient record forms for patients aged ≤14 years ranged from 6,500 to 9,400, and the number of these forms showing an antibiotic prescribed ranged from 1,300 to 2,500 for each 2-year period.
From 1993--1994 to 2007--2008, the overall average annual office visit rate, regardless of antibiotic prescribing, increased significantly (p<0.05), from 2,180 (95% confidence interval [CI] = 1,974--2,386) per 1,000 persons aged ≤14 years to 2,581 (CI = 2,291--2,871), an increase of 18%. However, the visit rate for the five ARIs examined decreased during the same period by 14%, from 654 (CI = 574--734) per 1,000 persons aged ≤14 years to 560 (CI = 471--648).
From 1993--1994 to 2007--2008, the overall average annual population-based rate of antibiotic prescriptions decreased 10%, from 655 (CI = 570--739) per 1,000 persons aged ≤14 years to 592 (CI = 492--691) (Figure 1). However, this decline was not constant; the rate decreased from 1995--1996 to 1999--2000 and was stable thereafter. For the five ARI diagnoses examined, the average annual population-based prescribing rate decreased 24%, from 448 (CI = 387--510) antibiotic prescriptions per 1,000 persons aged ≤14 years in 1993--1994 to 342 (CI = 277--406) in 2007--2008.
Physician office visit--based antibiotic prescribing rates decreased 24% during the study period, from 300 (CI = 276--324) antibiotic prescriptions per 1,000 visits by persons aged ≤14 years to 229 (CI = 206--253) (Figure 2). The average annual decrease was 6.7%. The antibiotic prescription rate per 1,000 office visits decreased 11% for the ARI diagnoses, including 19% for nonspecific upper respiratory infection and 26% for pharyngitis. Prescribing rates for the other three ARIs did not change significantly. Despite the decrease, in 2007--2008, ARIs still accounted for 58% of office visits where an antibiotic was prescribed for a person aged ≤14 years (Figure 3). However, this proportion was smaller than the 69% of office visits calculated for 1993--1994 (Figure 3).
Reported by
Linda F. McCaig, MPH, Ambulatory and Hospital Care Statistics Br, National Center for Health Statistics; Lauri A. Hicks, DO, Rebecca M. Roberts, MS, Div of Bacterial Diseases, National Center for Immunization and Respiratory Diseases; Tarayn A. Fairlie, MD, EIS Officer, CDC. Corresponding contributor: Tarayn A. Fairlie, tfairlie@cdc.gov, 404-639-4849.
Editorial Note
The findings in this report show an overall decrease in both population-based and visit-based antibiotic prescribing rates for persons aged ≤14 years in the United States from 1993--1994 to 2007--2008. Changes in the population-based prescribing rates likely reflect a combination of factors, including a decreased need for antibiotics because of introduction of pneumococcal conjugate vaccine and decreased office visits for ARI (4). The 24% decrease overall and 11% decrease in ARI-related visit-based antibiotic prescribing rates also suggest that physician prescribing behavior has changed.
Although these changes in physician behavior are encouraging, several areas require further intervention. First, 58% of the antibiotics prescribed in the office setting in 2007--2008 were for five ARIs, most episodes of which do not require antibiotic treatment but are common outpatient diagnoses for which patient expectations, as well as physician behavior, contribute to inappropriate antibiotic use (5). Second, prescribing antibiotics for otitis media has not decreased significantly, despite the American Academy of Pediatrics 2004 release of guidelines recommending watchful waiting for otherwise healthy children aged ≥2 years without severe symptoms of otitis media or with an uncertain diagnosis (6). The results for otitis media contrast with those for pharyngitis, where a significant decrease in antibiotic prescribing was observed from 1993--1994 to 2007--2008, perhaps because rapid diagnostic testing for group A streptococcus improved prescription decision-making. With expanding resistance profiles among common pathogens, treatment options are dwindling, and reducing inappropriate use of antibiotics is increasingly important.
Similar issues are being addressed in Europe, where young children also are the main recipients of antibiotics and most antibiotics are given for upper respiratory infections (7). Studies in Germany, where the volume of antibiotic use is in the bottom third among countries in the European Union (8), have shown that more than one third of the population had taken antibiotics in the previous year (9). Far higher rates of antibiotic use have been observed in southern and eastern Europe (9). The European Union has made reducing antibiotic use among children a priority with creation in October 2009 of the Antibiotic Resistance and Prescribing in European Children network (10).
The findings in this report are subject to at least two limitations. First, only the primary diagnosis was examined, and antibiotic prescriptions were attributed to that diagnosis. Antibiotics also might have been prescribed for the second or third diagnoses, which might have resulted in misclassification. Second, only antibiotic prescribing related to office visits was considered; prescribing related to telephone or e-mail encounters was excluded, thus potentially underrepresenting the frequency of antibiotic prescribing for children.
In 1995, CDC launched the Campaign for Appropriate Antibiotic Use in the Community, which in 2003 was renamed Get Smart: Know When Antibiotics Work. The purpose of the program is to educate parents and health-care providers about the importance of appropriate antibiotic use. In November 2009, recognizing the need for increased global cooperation in combating antibiotic resistance, the United States and European Union created the Trans-Atlantic Task Force on Antimicrobial Resistance.† In November 2010, CDC's third annual Get Smart About Antibiotics Week was held in the United States at the same time Antibiotic Awareness Day was held in the European Union. CDC also launched a companion program focused on in-patient settings called Get Smart for Healthcare.
These observances stress that inappropriate antibiotic use anywhere leads to antibiotic resistance everywhere, and that reducing inappropriate antibiotic use is a global responsibility. CDC's Get Smart program encourages local and state health departments, individual practitioners, and public and private organizations to partner with them to reduce inappropriate antibiotic use by participating in Get Smart Week 2011, which will be held November 14--20, 2011. Additional information is available at http://www.cdc.gov/getsmart or via e-mail (getsmart@cdc.gov).
References
- Harrison PF, Lederberg J. Antimicrobial resistance: issues and options. Workshop report. Washington DC: National Academy Press; 1998.
- Bronzwaer S, Cars O, Buchholz U, et al. A European study on the relationship between antimicrobial use and antimicrobial resistance. Emerg Infect Dis 2002;8:278--82.
- US Census Bureau. National population estimates by age, sex, race, and Hispanic origin: 1980--1999. Washington, DC: US Census Bureau; 2000. Available at http://www.census.gov/popest/national/asrh/natasrh.html. Accessed August 24, 2011.
- Grijalva CG, Griffin MR. Population-based impact of routine infant immunization with pneumococcal conjugate vaccine in the USA. Expert Rev Vaccines 2008;7:83--95.
- Barden LS, Dowell SF, Schwartz B, Lackey C. Current attitudes regarding use of antimicrobial agents: results from physicians' and parents' focus group discussions. Clin Ped 1998;37:665--71.
- American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics 2004;113:1451--65.
- Moro ML, Marchi M, Gagliotti C, Di Mario S, Resi D. Why do paediatricians prescribe antibiotics? Results of an Italian regional project. BMC Pediatr 2009;9:69.
- Goossens H, Ferech M, Coenen S, Stephens P. Comparison of outpatient systemic antibacterial use in 2004 in the United States and 27 European countries. Clin Infect Dis 2007;44:1091--5.
- European Commission. Special Eurobarometer 338: antimicrobial resistance. Brussels, Belgium: European Commission; 2010. Available at http://ec.europa.eu/health/antimicrobial_resistance/docs/ebs_338_en.pdf. Accessed August 24, 2011.
- Henderson KL, Muller-Pebody B, Johnson AP, Goossens H, Sharland M. First set-up meeting for Antibiotic Resistance and Prescribing in European Children (ARPEC). Euro Surveill 2009;14(45).
* Available at http://www.cdc.gov/nchs/ahcd/ahcd_scope.htm#namcs_scope.
† Additional information available at http://www.whitehouse.gov/the-press-office/us-eu-joint-declaration-and-annexes.
What is already known on this topic?
Inappropriate antibiotic use contributes to antimicrobial resistance, a major health threat in the United States. Children frequently are prescribed antibiotics in U.S. physician offices and most typically for acute respiratory infections (ARIs), even though most ARI episodes do not require antibiotic treatment.
What is added by this report?
The antibiotic prescribing rate for persons aged ≤14 years in U.S. physician offices decreased 24%, from 300 antibiotic courses per 1,000 office visits in 1993--1994 to 229 antibiotic courses per 1,000 office visits in 2007--2008. However, in 2007--2008 ARIs still accounted for 58% of all office-based antibiotic prescribing, and prescribing rates for otitis media, sinusitis, and bronchitis had not changed significantly.
What are the implications for public health practice?
Antibiotic prescribing for persons aged ≤14 years in the United States remains inappropriately high. Further intervention is needed to decrease inappropriate antibiotic prescribing for this population.
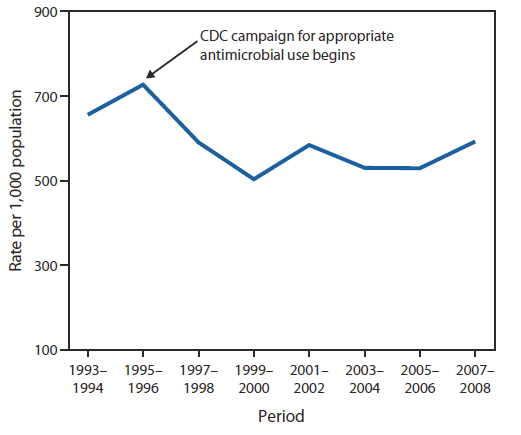
Alternate Text: The figure above shows the average annual antibiotic prescribing rates for physician office-related visits per 1,000 population of persons aged <14 years, in the United States from 1993-1994 to 2007-2008. From 1993-1994 to 2007-2008, the overall average annual population-based rate of antibiotic prescriptions decreased 10% from 655 per 1,000 persons aged ≤14 years to 592.
FIGURE 2. Average annual antibiotic prescribing rates for persons aged ≤14 years per 1,000 physician office visits --- National Ambulatory Medical Care Survey, United States, 1993--1994 to 2007--2008
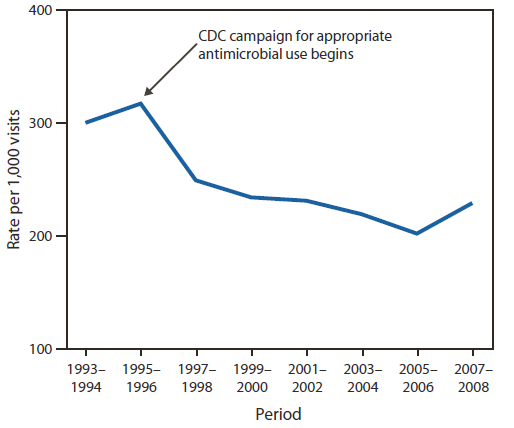
Alternate Text: The figure above shows the average annual antibiotic prescribing rates for persons aged <14 years per 1,000 physician office visits, in the United States from 1993-1994 to 2007-2008. Physician office visit-based antibiotic prescribing rates decreased 24% during the study period, from 300 antibiotic prescriptions per 1,000 visits by persons aged ≤14 years to 229.
FIGURE 3. Average annual percentage of physician office visits by persons aged ≤14 years where an antibiotic was prescribed, by primary diagnosis --- National Ambulatory Medical Care Survey, United States, 1993--1994 and 2007--2008
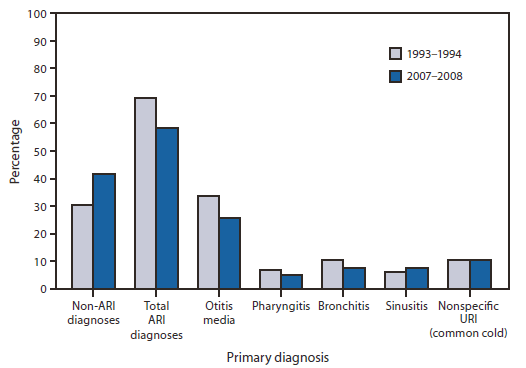
Abbreviations: ARI = acute respiratory infection; URI = upper respiratory infection.
Alternate Text: The figure above shows the average annual percentage of physician office visits by persons aged <14 years where an antibiotic was prescribed, by primary diagnosis, in the United States from 1993-1994 and 2007-2008. The antibiotic prescription rate per 1,000 office visits decreased 11% for five acute respiratory infection (ARI) diagnoses, including 19% for nonspecific upper respiratory infection and 26% for pharyngitis. Despite the decrease, in 2007-2008, ARIs still accounted for 58% of office visits where an antibiotic was prescribed for a person aged ≤14 years.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
