FIGURE. Cases of cryptosporidiosis at a summer camp (n = 42*), by date of onset of gastrointestinal symptoms --- North Carolina, 2009
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Cryptosporidiosis Outbreak at a Summer Camp --- North Carolina, 2009
In July 2009, local, regional, state, and federal public health officials investigated a cryptosporidiosis outbreak at a youth summer camp in North Carolina. The investigation identified 46 laboratory-confirmed and probable cryptosporidiosis cases at the camp. Analyses of data from a retrospective cohort study of staff members revealed that eating ham from a sandwich bar that included camp-grown raw produce and sharing a cabin with an ill person were significantly associated with illness. Cryptosporidium isolates from stool specimens of livestock and humans at the camp were of the identical Cryptosporidium parvum subtype, IIaA17G2R1, indicating that zoonotic transmission had occurred, and suggesting a link not implicated by traditional epidemiologic methods. This investigation underscores the importance of reducing the risk for Cryptosporidium transmission in camp settings and the value of Cryptosporidium subtyping as a tool to elucidate cryptosporidiosis epidemiology.
On June 24, owners of a North Carolina youth summer camp and health-care providers began identifying cases of diarrhea in campers and staff members and notified local public health officials. By June 30, local, regional, and state public health officials had identified four laboratory-confirmed cases of cryptosporidiosis and >30 cases of diarrhea at the camp. CDC was asked to collaborate on the investigation because no common outbreak exposure was identified and multiple potential outbreak sources were present at the camp. The investigation focused on identifying risk factors associated with acute cryptosporidiosis and implementing control measures to stop Cryptosporidium transmission at the camp.
Cryptosporidiosis is a diarrheal illness caused by the parasite Cryptosporidium. Fecal-oral transmission of Cryptosporidium oocysts can occur via ingestion of contaminated recreational water, drinking water, or food, or via contact with infected persons or animals, most notably preweaned calves (1). Potential routes of transmission at the camp included several recreational water venues (a swimming pool, lake, and river), drinking water supplied by wells, meals served by a central kitchen, and a garden that provided >50% of the produce for camp meals. Multiple animals, with which campers and staff members had contact, were kept at the camp, including cows, goats, and pigs. Ten Jersey and 12 Holstein preweaned calves arrived at the camp on May 29 and June 13, respectively.
For this investigation, a case was defined as probable if the ill person 1) had been at the camp during June 20--26, 2009, and 2) had onset of gastrointestinal symptoms (including diarrhea, defined as three or more loose or watery stools in 24 hours) after June 21, 2009. Confirmed cases were defined as meeting those conditions and having laboratory-based evidence of Cryptosporidium infection. Human and animal stool specimens were tested for Cryptosporidium, and isolates were subtyped using DNA sequence analysis (2). In response to anecdotal reports of bloody diarrhea, stool specimens also were tested for bacterial pathogens.
A total of 46 cases were identified; 12 confirmed and 34 probable. The unimodal epidemic curve peaked on June 26--27 (Figure). Cryptosporidium was detected in stool specimens from 12 patients.* C. parvum was detected in stool specimens from one (10%) of 10 Jersey calves, two (17%) of 12 Holstein calves, one goat kid (33%) of three goats, and one piglet (50%) of two pigs. C. parvum isolates from seven humans and all but one of the animals were of the identical C. parvum subtype, IIaA17G2R1. Shiga toxin--producing Escherichia coli serogroup O111 strains were detected in stool specimens of one patient† and five calves; the pulsed-field gel electrophoresis (PFGE) pattern of the human E. coli isolate did not match any of the three PFGE patterns found in the calf isolates.
A retrospective cohort study enrolled staff members only; campers, who were as young as age 5 years, were excluded because of concerns about recall accuracy and because they had minimal variation in their camp activities. The self-administered study questionnaire asked about clinical symptoms and approximately 160 camp-specific exposures and individual food items. All risk factors in bivariate analysis with p-values <0.05 were considered for inclusion in the multivariable model. Because data were sparse and many risk factors were assessed, the final multivariable model was constructed using stepwise selection, starting with the variable with the smallest p-value and adding variables one by one. The final model included only significant (p<0.05) covariates.
Of 129 staff members, 123 (95%) completed the retrospective cohort study questionnaire (Table). In multivariable analysis, only two factors were significantly associated with illness: ham from the sandwich bar on June 21 (adjusted prevalence ratio [aPR] = 3.5; 95% confidence interval [CI] = 1.6--7.4) and sharing a cabin with an ill person (aPR = 2.8; CI = 1.3--6.2).
A simultaneous environmental health investigation included inspection of the camp and collection of samples from all camp water sources, including the pool, lake, creeks, river, wells, produce preparation sink, and ice-maker filter, and composite soil samples from the gardens for Cryptosporidium testing. The investigation revealed that persons were encouraged to spray a diluted bleach solution on their hands before and after interacting with the calves,§ but a hand-washing sink was not available in the barn area. Cryptosporidium spp. were detected in multiple composite soil samples from the gardens; however, components of the soil inhibited DNA amplification and precluded typing of Cryptosporidium isolates. Cryptosporidium was not detected in any of the water samples. After the outbreak began, the camp implemented control measures, including installing a hand-washing sink in the barn area.
Reported by
Sarah A. Collier, MPH, IHRC, Atlanta, GA. Steven Smith, MPA, Anita Lowe, Patricia Hawkins, Pam McFarland, Transylvania County Health Dept, Brevard; Martha Salyers, MD, Phyllis Rocco, MPH, Ginger Bumby, North Carolina Public Health Regional Surveillance Team 6, Asheville; Jean-Marie Maillard, MD, Carl Williams, DVM, North Carolina Div of Public Health, North Carolina Dept of Health and Human Svcs. Aaron Fleischauer, PhD, Career Epidemiology Field Officer Program, Office for Public Health Preparedness and Emergency Response; Vincent Radke, MPH, Div of Emergency and Environmental Health Svcs, National Center for Environmental Health; Jacquelin M. Roberts, MS, Allen W. Hightower, MS, Henry S. Bishop, Blaine A. Mathison, Alexandre J. da Silva, PhD, Div of Parasitic Diseases and Malaria, Center for Global Health; Joe Carpenter, Althea S. Hayden, MD, Div of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases; Michele C. Hlavsa, MPH, Lihua Xiao, DVM, PhD, Virginia A. Roberts, MSPH, Joan Brunkard, PhD, Michael J. Beach, PhD, Vincent Hill, PhD, Jonathan Yoder, MPH, MSW, Elizabeth L. Dunbar, MPH, Theresa Dearen, Cheryl Bopp, MS, Michael S. Humphrys, MS, Div of Foodborne, Waterborne, and Environmental Diseases, National Center for Zoonotic, Vector-Borne, and Enteric Diseases; Ghasi Phillips, ScD, Loretta Chang, MD, Elissa M. Meites, MD, EIS officers, CDC. Corresponding contributor: Michele C. Hlavsa, healthywater@cdc.gov.
Editorial Note
The incidence of reported cryptosporidiosis in the United States increased from 1.0 cases per 100,000 population in 1999 to >3.0 cases in 2008 (3). The cause of this increase is unknown; however, recreational water plays an important role in Cryptosporidium transmission. In immunocompetent persons, cryptosporidiosis can range from asymptomatic infection to diarrhea that typically lasts 1--2 weeks. Immunocompromised persons might experience chronic, severe diarrhea, which can lead to malnutrition and substantial weight loss, potentially causing death. The principal Cryptosporidium species that infect humans are C. parvum, which can be transmitted zoonotically or anthroponotically, and Cryptosporidium hominis (formerly known as C. parvum genotype I), which primarily is transmitted anthroponotically. Molecular techniques are needed to distinguish the morphologically indistinguishable oocysts of the two species.
Traditional epidemiologic methods used in this outbreak investigation revealed a unimodal epidemic curve suggestive of a point-source exposure and that food was significantly associated with illness. Contact with calves or other livestock were not significantly associated with illness in bivariate analysis. However, molecular epidemiologic methods demonstrate that the C. parvum subtype IIaA17G2R1 transmitted at the camp likely came from livestock on the farm. Ham from the June 21 sandwich bar might be a marker for contaminated produce. Lettuce grown at the camp and commercially purchased tomatoes and onions were available as sandwich toppings. The lettuce was grown adjacent to the calves' area. One patient who was only at the camp June 22--23 did not participate in the June 21 lunch, but reported eating quesadillas with lettuce and tomatoes on June 22. The association between eating lettuce at the June 22 dinner and illness was significant in bivariate analysis, but not in multivariable analysis.
The mechanism leading to food contamination could not be identified. However, C. parvum transmission from animals to humans occurred, sharing a cabin with an ill person was significantly associated with illness, and the barn area lacked a hand-washing sink, suggesting that hand hygiene at the camp could be improved. This is particularly important because campers and staff members participated in livestock care and produce harvesting. The timing of both sets of calves' arrival at the North Carolina camp and the onset of the outbreak suggests that the parasite might have been introduced to the camp by the Holstein calves. Findings from previously reported cryptosporidiosis outbreaks at camps with calves present have indicated that visible manure on hands was associated with illness; conversely, habitual hand washing with soap after calf contact was protective (4). Along with hand washing, additional measures to protect against transmission of Cryptosporidium in camp settings are needed (Box).
The findings in this report are subject to at least four limitations. First, the study questionnaire did not ask respondents about raw produce added to their sandwiches on June 21. Second, only 26 cases were included in the cohort study, limiting statistical power. Third, persons with preexisting Cryptosporidium antibodies might be less likely to develop illness upon reinfection (5), introducing possible misclassification of illness status and biasing estimates of association between exposure and illness toward the null. Finally, this investigation might have failed to identify all ill food handlers, a source of previously reported foodborne cryptosporidiosis outbreaks (6). Two food handlers (onset of illness June 27 and 28) were removed from kitchen duties when they reported their illness to camp owners. Neither reported any camp-specific risk factors for illness other than communal meals.
This investigation demonstrates the need for extensive use of effective measures to prevent Cryptosporidium transmission at camps where animals are kept (7). Hand-washing facilities with running water, soap, and disposable towels or air dryers should be accessible in animal areas. Hands should be washed after touching animals or their waste; before, during, and after food preparation; and after using the toilet, caring for ill persons, or cleaning soiled bedding. Cryptosporidium is chlorine-tolerant, and alcohol-based hand sanitizers are not effective against it.
C. parvum subtype IIaA17G2R1 previously was identified as the etiologic agent of an Ohio outbreak associated with ozonated apple cider (8). C. parvum infection is common in preweaned calves. Although C. parvum subtype IIaA17G2R1 infection in calves has been documented (2,9), the significance of isolating this C. parvum subtype is unknown. Cryptosporidium isolates are not systematically subtyped in the United States. Subtyping has generally been limited to use as an outbreak investigation tool at the national level, despite its epidemiologic utility. In this outbreak investigation, subtyping verified an epidemiologic link that was not implicated by traditional epidemiologic methods; in other investigations, subtyping differentiated individual clusters (8,10). Systematically subtyping Cryptosporidium isolates via a national molecular surveillance program could elucidate transmission patterns and help direct prevention efforts needed to address increasing incidence of cryptosporidiosis (3).
References
- Santin M, Trout JM, Xiao L, Zhou L, Greiner E, Fayer R. Prevalence and age-related variation of Cryptosporidium species and genotypes in dairy calves. Vet Parasitol 2004;122:103--17.
- Xiao L, Hlavsa MC, Yoder J, et al. Subtype analysis of Cryptosporidium specimens from sporadic cases in Colorado, Idaho, New Mexico, and Iowa in 2007: widespread occurrence of one Cryptosporidium hominis subtype and case history of an infection with the Cryptosporidium horse genotype. J Clin Microbiol 2009;47:3017--20.
- Yoder JS, Beach MJ. Cryptosporidium surveillance and risk factors in the United States. Exp Parasitol 2010;124:31--9.
- Smith KE, Stenzel SA, Bender JB, et al. Outbreaks of enteric infections caused by multiple pathogens associated with calves at farm day camp. Pediatr Infect Dis 2004;23:1098--104.
- Moss DM, Chappell CL, Okhuysen PC, et al. The antibody response to 27-, 17-, and 15-kDa Cryptosporidium antigens following experimental infection in humans. J Infect Dis 1998;178:827--33.
- Smith HV, Caccio SM, Cook N, Nichols RAB, Tait A. Cryptosporidium and Giardia as foodborne zoonoses. Vet Parasitol 2007;149:29--40.
- CDC. Compendium of measures to prevent disease associated with animals in public settings, 2011. MMWR 2011;60(No. RR-4).
- Blackburn BG, Mazurek JM, Hlavsa M, et al. Cryptosporidiosis associated with ozonated apple cider. Emerg Infect Dis 2006;12:684--6.
- Xiao L, Zhou L, Santin M, Yang W, Fayer R. Distribution of Cryptosporidium parvum subtypes in calves in eastern United States. Parasitol Res 2007;100:701--6.
- Valderrama AL, Hlavsa MC, Cronquist A, et al. Multiple risk factors associated with a large statewide increase in cryptosporidiosis. Epidemiol Infect 2009;137:1781--8.
* Commercial laboratories detected Cryptosporidium spp. in stool specimens of five patients. These five stool specimens had been discarded, and isolates were not available for confirmatory testing and Cryptosporidium subtyping unlike the remaining seven.
† Stool specimens from only four of the seven patients with laboratory-confirmed C. parvum infection were tested for bacterial pathogens.
§ Although dilute bleach solution might effectively disinfect chlorine-susceptible pathogens such as E. coli, it would not be an effective disinfectant for Cryptosporidium, which is extremely chlorine-tolerant.
What is already known on this topic?
Cryptosporidium is an extremely chlorine-tolerant parasite that causes cryptosporidiosis, a common cause of diarrhea in the United States. Fecal-oral transmission of Cryptosporidium can occur via ingestion of contaminated recreational water, drinking water, food, or via contact with infected persons or animals, most notably preweaned calves.
What is added by this report?
Traditional epidemiologic methods indicated food and person-to-person contact were significantly associated with illness. However, Cryptosporidium subtyping results indicated the source of the outbreak was likely to be preweaned calves, a source that was not implicated by traditional epidemiologic methods.
What are the implications for public health practice?
Camps where animals are kept need to enforce effective hygiene and sanitation practices to prevent Cryptosporidium transmission. A national program that systematically subtypes Cryptosporidium isolates could elucidate the epidemiology of cryptosporidiosis in the United States.
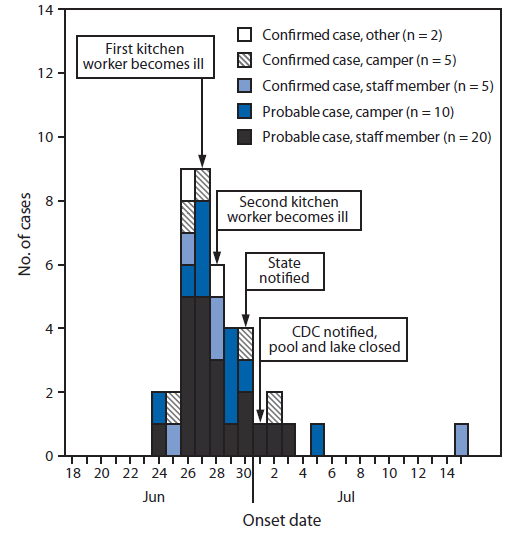
* An additional four probable cases involving two staff members, one camper, and one other person had unknown symptom onset dates but reported onset of gastrointestinal symptoms after June 21, 2009.
Alternate Text: The figure above shows cases of cryptosporidiosis at a summer camp in North Carolina during June and July 2009 (n = 42), by date of onset of gastrointestinal symptoms among staff members, campers, and others. A total of 46 cases were identified; 12 confirmed and 34 probable. The unimodal epidemic curve peaked on June 26-27.
|
BOX. Key recommendations for camp owners and managers to help prevent and control transmission of Cryptosporidium* |
|
Hand washing Provide appropriate and accessible hand hygiene stations with running water, soap, and disposable towels or air dryers. Alcohol-based hand sanitizers are not effective against Cryptosporidium. Hands should be washed
Steps on how to properly wash hands are described at http://www.cdc.gov/handwashing. Animals Consider limiting contact with preweaned calves. Review and implement recommendations in the Compendium of Measures to Prevent Disease Associated with Animals in Public Settings, 2011, available at http://www.cdc.gov/mmwr/pdf/rr/rr6004.pdf. Food Maintain food services to the standards set by local or state laws. Exclude persons from food and beverage preparation if they are ill with diarrhea or other gastrointestinal symptoms. * Additional recommendations for camp facilities to prevent Cryptosporidium transmission are available at http://www.cdc.gov/parasites/crypto/camps.html. |
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
