* Instructions available at http://www.cdc.gov/std/gonorrhea/arg/specimen_shipping_instructions1-29-08.pdf.
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Cephalosporin Susceptibility Among Neisseria gonorrhoeae Isolates --- United States, 2000--2010
Neisseria gonorrhoeae is a major cause of pelvic inflammatory disease, ectopic pregnancy, and infertility, and it can facilitate human immunodeficiency virus (HIV) transmission (1). Emergence of gonococcal resistance to penicillin and tetracycline occurred during the 1970s and became widespread during the early 1980s. More recently, resistance to fluoroquinolones developed. Resistance was documented first in Asia, then emerged in the United States in Hawaii followed by other western states. It then became prevalent in all other regions of the United States. In Hawaii, fluoroquinolone resistance was first noted among heterosexuals; however, resistance in the United States initially became prevalent among men who have sex with men (MSM) before generalizing to heterosexuals. This emergence of resistance led CDC, in 2007, to discontinue recommending any fluoroquinolone regimens for the treatment of gonorrhea (2--3). CDC now recommends dual therapy for gonorrhea with a cephalosporin (ceftriaxone 250 mg) plus either azithromycin or doxycycline (4). This report summarizes trends in cephalosporin susceptibility among N. gonorrhoeae isolates in the United States during 2000--2010 using data from the Gonococcal Isolate Surveillance Project (GISP). During that period, the percentage of isolates with elevated minimum inhibitory concentrations (MICs) to cephalosporins (≥0.25 µg/mL for cefixime and ≥0.125 µg/mL for ceftriaxone) increased from 0.2% in 2000 to 1.4% in 2010 for cefixime and from 0.1% in 2000 to 0.3% in 2010 for ceftriaxone. Although cephalosporins remain an effective treatment for gonococcal infections, health-care providers should be vigilant for treatment failure and are requested to report its occurrence to state and local health departments. State and local public health departments should promote maintenance of laboratory capability to culture N. gonorrhoeae to allow testing of isolates for cephalosporin resistance. They also should develop enhanced surveillance and response protocols for gonorrhea treatment failures and report gonococcal treatment failures to CDC.
GISP is a CDC-sponsored, sentinel surveillance system that monitors antimicrobial susceptibilities in N. gonorrhoeae through ongoing testing of approximately 5,900 male urethral gonococcal isolates obtained annually from consecutive symptomatic men at 25--30 sexually transmitted disease (STD) clinics in the United States; approximately 4% of all reported gonorrhea cases among men are included annually (5). Antibiotic susceptibility is measured by MIC, the lowest concentration of an antibiotic that inhibits visible growth of the bacteria. MICs to cephalosporins (cefixime and ceftriaxone) among gonococcal isolates collected during 2000--2010 were analyzed. Cefixime susceptibilities were not determined during 2007--2008 because cefixime was unavailable in the United States during that period. Decreased antibiotic susceptibility for cefixime or ceftriaxone is defined by the Clinical and Laboratory Standards Institute (CLSI) as MICs ≥0.5 µg/mL; criteria for cefixime and ceftriaxone resistance in N. gonorrhoeae have not been defined (6). Because few isolates exhibited decreased susceptibility and increases in MICs can precede the emergence of resistance, the percentage of isolates with elevated MICs (≥0.25 µg/mL for cefixime and ≥0.125 µg/mL for ceftriaxone) was assessed to determine if MICs to cephalosporins were increasing with time. These breakpoints were used in GISP for surveillance purposes. The analyses were stratified by U.S. census region and sex of sex partner. The South and Northeast regions were combined because fewer samples are collected in the eastern half of the country compared with the western half (Figure 1). Sex of sex partner was categorized as MSM or men who have sex exclusively with women (MSW). Resistance to penicillin (MIC ≥2.0 µg/mL), tetracycline (MIC ≥2.0 µg/mL), and ciprofloxacin (MIC ≥1.0 µg/mL), a fluoroquinolone, were assessed. Cochran-Armitage trend tests were performed to assess statistical significance (p<0.05).
An average of 5,865 isolates (range: 5,367--6,552) were tested annually during 2000--2010. Overall, the percentage of isolates with cefixime MICs ≥0.25 µg/mL increased from 0.2% to 1.4% during 2000--2010 (p<0.001). The percentage of isolates with ceftriaxone MICs ≥0.125 µg/mL increased from 0.1% to 0.3% during 2000--2010 (p = 0.047). From 2000 to 2010, in the western region, the percentage of isolates with cefixime MICs ≥0.25 µg/mL increased from 0% to 3.3% (p<0.001), and the percentage of isolates with ceftriaxone MICs ≥0.125 µg/mL increased from 0% to 0.5% (p<0.001) (Table). In the western region, the most prominent increases in cefixime MICs were observed in Honolulu, Hawaii (0% in 2000 and 7.7% in 2010 [p<0.001]), and in California (0% in 2000 and 4.5% in 2010 [p<0.001]). An increase in ceftriaxone MICs also was observed in California (0% in 2000 and 0.6% in 2010 [p = 0.001]).
Among MSM, the percentage of isolates with cefixime MICs ≥0.25 µg/mL increased from 0% in 2000 to 4.0% during 2010 (p<0.001), and the percentage of isolates with ceftriaxone MICs ≥0.125 µg/mL increased from 0% to 0.9% (p<0.001). Overall, no statistically significant increases occurred in cefixime or ceftriaxone MICs among MSW (Figure 2). Regionally, increases in the percentage of isolates with cefixime MICs ≥0.25 µg/mL among MSM were observed in all regions during 2000--2010 (West: 0% in 2000 and 5.0% in 2010 [p<0.001]; Midwest: 0% in 2000 and 3.4% in 2010 [p = 0.001]; Northeast and South: 0% in 2000 and 0.9% in 2010 [p = 0.035]). A significant increase among MSW was identified in the West (0% in 2000 and 1.3% in 2010 [p<0.001]); however, no change occurred in the Midwest (0.3% in 2000 and 0.1% in 2010), and a significant decrease occurred in the Northeast and South (0.4% in 2000 and 0% in 2010 [p<0.001]). For isolates with ceftriaxone MICs ≥0.125 µg/mL, significant regional increases were observed among MSM in the West (0% in 2000 and 0.8% in 2010 [p<0.001]) and Midwest (0% in 2000 and 2.0% in 2010 [p = 0.046]) and among MSW in the West (0% in 2000 and 0.2% in 2010 [p = 0.008]); no significant increases were observed among MSM or MSW in other regions.
During 2009--2010, 13 (0.11%) of 11,323 isolates had decreased susceptibility to cefixime (MICs = 0.5 µg/mL), compared with seven (0.02%) of 41,462 isolates during 2000--2006 (p<0.001) (isolates were not tested for cefixime susceptibility during 2007--2008). All 2009--2010 isolates with decreased susceptibility to cefixime were resistant to tetracycline and ciprofloxacin, all but one were resistant to penicillin, and none exhibited decreased susceptibility to azithromycin (≥2 µg/mL). Twelve of the men from whom the isolates were obtained were MSM; 10 men resided in the West, and three in the Midwest. No isolates had decreased susceptibility to ceftriaxone during 2000--2010.
Reported by
Carlos del Rio, MD, Rollins School of Public Health, Emory Univ, Atlanta, Georgia. Geraldine Hall, PhD, Dept of Clinical Pathology, Cleveland Clinic, Cleveland, Ohio. Edward W. Hook, Div of Infectious Disease, MD, Univ of Alabama at Birmingham. William L.H. Whittington, Dept of Medicine, Univ of Washington. Robert D. Kirkcaldy, MD, John R. Papp, PhD, Hillard Weinstock, MD, Div of STD Prevention, National Center for HIV, Hepatitis, STD, and TB Prevention; Erin L. Murray, PhD, EIS Officer, CDC. Corresponding contributor: Robert D. Kirkcaldy, rkirkcaldy@cdc.gov, 404-639-8659.
Editorial Note
The epidemiologic pattern of cephalosporin susceptibility in the West and among MSM during 2009--2010 is similar to that previously observed during the emergence of fluoroquinolone-resistant N. gonorrhoeae in the United States (2--3,7). Although the history of fluoroquinolone-resistant N. gonorrhoeae might not predict the patterns of decreasing cephalosporin susceptibility, the observed trends are concerning. During 2001--2010, decreased gonococcal susceptibility to cephalosporins and reported treatment failures have been documented in Asia (8). Recently, two cases of gonococcal treatment failure were reported from Norway among heterosexual men with gonococcal urethritis treated with cefixime (9), and a pharyngeal isolate with a ceftriaxone MIC = 2.0 µg/mL was identified from a female commercial sex worker in Japan (10).
The potential emergence of gonococcal cephalosporin resistance is of particular concern because the U.S. gonorrhea control strategy relies upon effective antibiotic therapy. Previously, the emergence and spread of gonococcal antibiotic resistance in the United States was addressed by changing the recommended antibiotics for treatment. No other well-studied and effective antibiotic treatment options or combinations currently are available. The emergence of gonococcal cephalosporin resistance would substantially limit available treatment options.
In light of the diminished resources available to STD control programs and the past inability to prevent emergence of resistance, the eventual emergence of cephalosporin resistance appears likely. Actions undertaken now could delay the spread of cephalosporin-resistant strains and mitigate the public health consequences. Effective treatment of gonorrhea is essential and now requires two antibiotics. The findings in this report suggest that gonococcal resistance to cefixime might emerge in the United States before resistance to ceftriaxone. Ceftriaxone is the most effective cephalosporin for treatment of gonorrhea and should be used for treatment of gonorrhea in combination with azithromycin or doxycycline (4). Azithromycin is preferred over doxycycline for dual therapy with ceftriaxone; of the 2009--2010 isolates with decreased susceptibility to cefixime, none exhibited decreased susceptibility to azithromycin, and all of them exhibited tetracycline resistance. Based on the findings in this report, CDC currently is recommending ceftriaxone 250 mg intramuscularly and azithromycin 1 g orally as the most effective treatment for uncomplicated gonorrhea.
In addition to effective treatment, prompt recognition of cephalosporin-resistant gonorrhea is critical. Although GISP has been successful in identifying important shifts in gonococcal epidemiology and antimicrobial susceptibility, its effectiveness should be complemented through partnerships with local health departments and health-care providers. Clinicians should remain vigilant for treatment failures (evidenced by persistent symptoms or a positive follow-up test despite treatment) among patients treated for gonorrhea with CDC-recommended antibiotics and obtain specimens for gonococcal culture from patients with possible treatment failure. Clinicians caring for patients with gonorrhea, particularly MSM in the western United States, might consider having patients return 1 week after treatment for test-of-cure with culture, preferably, or with nucleic acid amplification tests (NAATs).
If a patient experiences cefixime treatment failure, clinicians should re-treat the patient with 250 mg ceftriaxone intramuscularly and 2 g azithromycin orally (4). If a patient experiences a ceftriaxone treatment failure, clinicians should consult with an infectious disease expert and CDC regarding re-treatment. These patients should return for tests-of-cure within 1 week, preferably with culture, or, if culture is not available, with NAAT. If the follow-up NAAT result is positive, a specimen for culture should be obtained. Clinicians also should ensure that the patient's sex partners from the preceding 2 months are tested for gonorrhea (preferably with culture) and empirically treated with ceftriaxone 250 mg intramuscularly and azithromycin 2 g orally. Finally, these treatment failures should be reported to the local or state health department within 24 hours. Laboratorians are requested to report gonococcal isolates with decreased cefixime or ceftriaxone susceptibility (≥0.5 µg/mL) to their local or state health departments within 24 hours of identification. Local and state health departments are requested to report these cases immediately to CDC (gispinfo@cdc.gov or 404-639-8659). Isolates can be submitted to CDC's Neisseria Reference Laboratory for confirmation susceptibility testing.*
Local and state health departments also should promote maintenance of local gonococcal culture capacity, despite the widespread use of NAATs. Gonococcal antibiotic susceptibility testing (AST), necessary for identification of resistant isolates, only can be performed with culture specimens. Health departments should establish options for local availability of gonococcal cultures and AST, and consider enhancing surveillance for cephalosporin-resistant gonorrhea. Options for local culture and AST availability might involve building or enhancing local gonorrhea reference laboratory testing capacity, partnering with regional clinical laboratories or academic institutions, or sending isolates to CDC for susceptibility testing. Enhanced surveillance might include monitoring of multiple cases from the same patient reported within 30--60 days, often discarded as presumed duplicates. Finally, effective alternative antibiotics or antibiotic combinations for the treatment of gonorrhea are needed urgently; thus, the development of novel antibiotics and clinical trials to study combinations of existing antibiotics is necessary.
The findings in this report are subject to at least two limitations. First, data available in GISP only include results from urethral gonococcal isolates from males attending publicly funded STD clinics. Second, the clinical significance of shifts in MICs below CLSI criteria for decreased susceptibility is unclear, and transient increases and decreases in cephalosporin MICs have been observed previously in GISP. However, in light of similar trends in other regions of the world, the patterns observed in GISP with higher MICs in isolates from the west and MSM, and the ability of N. gonorrhoeae to develop resistance, the increasing MICs to cephalosporins in the United States are concerning. Vigilance of clinicians and enhanced surveillance by local and state health departments will be critical for early detection of treatment failures.
Acknowledgments
Collaborating state and local health departments. Participating STD clinic and regional laboratory staff members. Alesia Harvey, Michael Grabenstein, Kevin Pettus, Samera Bowers, Gail Bolan, MD, Kimberly Workowski, MD, Div of STD Prevention, National Center for HIV, Hepatitis, STD, and TB Prevention, CDC.
References
- Fleming D, Wasserheit J. From epidemiological synergy to public health policy and practice: the contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Trans Infect 1999;75:3--17.
- CDC. Fluoroquinolone-resistance in Neisseria gonorrhoeae, Hawaii, 1999, and decreased susceptibility to azithromycin in N. gonorrhoeae, Missouri, 1999. MMWR 2000;49:833--7.
- CDC. Update to CDC's sexually transmitted diseases treatment guidelines, 2006: fluoroquinolones no longer recommended for treatment of gonococcal infections. MMWR 2007;56:332--6.
- CDC. Sexually transmitted diseases treatment guidelines, 2010. MMWR 2010;59(No. RR-12).
- CDC. Sexually transmitted disease surveillance supplement 2007, Gonococcal isolate surveillance project annual report 2007. Atlanta, GA: US Department of Health and Human Services, CDC; 2009. Available at http://www.cdc.gov/std/gisp2007/gispsurvsupp2007short.pdf. Accessed June 28, 2011.
- National Committee for Clinical Laboratory Standards. Approved standard M100-38 performance standards for antimicrobial susceptibility testing. Wayne, PA: National Committee for Clinical Laboratory Standards;1998.
- Wang S, Harvey A, Conner S, et al. Antimicrobial resistance for Neisseria gonorrhoeae in the United States, 1988 to 2003: the spread of fluoroquinolone resistance. Ann Intern Med 2007;147:81--8.
- Tapsall J. Neisseria gonorrhoeae and emerging resistance to extended spectrum cephalosporins. Curr Opin Infect Dis 2009;22:87--91.
- Unemo M, Golparian D, Syversen G, et al. Two cases of verified clinical failures using internationally recommended first-line cefixime for gonorrhoeae treatment, Norway, 2010. Eurosurveillance 2010;15:19721--3.
- Ohnishi M, Saika T, Hoshina S, et al. Ceftriaxone-resistant Neisseria gonorrhoeae, Japan. Emerg Infect Dis 2011;17:148--9.
What is already known on this topic?
Cephalosporins are a critical component of CDC-recommended gonorrhea treatment; however, declining cephalosporin susceptibility and cephalosporin treatment failures have been reported in Asia and Europe.
What is added by this report?
This report describes current trends in cephalosporin susceptibility among Neisseria gonorrhoeae isolates in the United States: minimum inhibitory concentrations (MICs) to cephalosporins are increasing, suggesting that susceptibility to cephalosporins might be declining. The prevalence of isolates with elevated MICs remains low overall.
What are the implications for public health practice?
Health-care providers should use ceftriaxone and azithromycin for treatment of gonorrhea, remain vigilant for gonorrhea cephalosporin treatment failures, and report treatment failures to their local or state health departments. Local and state health departments should promote the maintenance of local gonococcal culture capacity, establish options for local gonococcal antibiotic susceptibility testing, consider enhancing surveillance for cephalosporin-resistant gonorrhea, and report gonorrhea cases with cephalosporin treatment failure to CDC.
FIGURE 1. Sentinel sites participating in the Gonococcal Isolate Surveillance Project --- United States, 2000--2010*
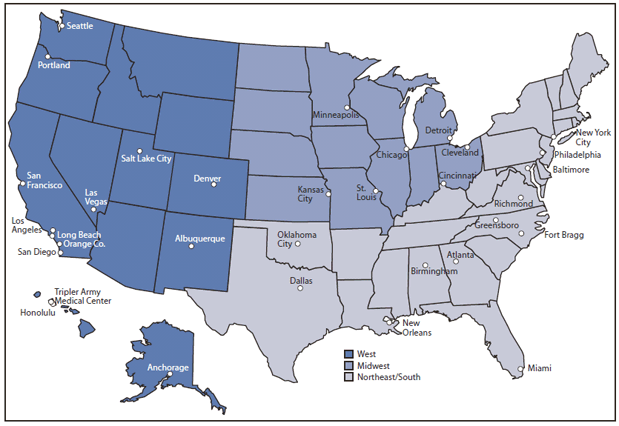
* Sites had continuous participation during 2000--2010 with the following exceptions (and years of participation): Anchorage (2000--2003); Detroit (2003--2010); Fort Bragg (2000--2002); Greensboro (2002--2010); Kansas City (2000--2001 and 2007--2010); Los Angeles (2003--2010); Las Vegas (2002--2010); Long Beach (2000--2007); New York City (2006--2010); Oklahoma City (2003--2010); Richmond (2007--2010); Salt Lake City (2003); St. Louis (2000--2004); and Tripler Army Medical Center (2001--2006 and 2009--2010).
Alternate Text: The figure above shows sentinel sites participating in the Gonococcal Isolate Surveillance Project in the United States during 2000-2010. The South and Northeast regions were combined because fewer samples are collected in the eastern half of the country compared with the western half.
FIGURE 2. Percentage of gonorrhea isolates with cefixime MICs ≥0.25 µg/mL and ceftriaxone MICs ≥0.125 µg/mL, by sex of sex partner --- Gonococcal Isolate Surveillance Project, United States, 2000--2010
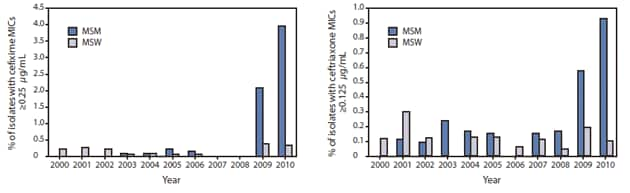
Abbreviations: MICs = minimum inhibitory concentrations; MSM = men who have sex with men; MSW = men who have sex exclusively with women.
Alternate Text: The figures above show the percentage of gonorrhea isolates with cefixime minimum inhibitory concentrations (MICs) ≥0.25 μg/mL and ceftriaxone MICs ≥0.125 μg/mL, by sex of sex partner in the United States, according to the Gonococcal Isolate Surveillance Project during 2000-2010. Among men who have sex with men, the percentage of isolates with cefixime MICs ≥0.25 μg/mL increased from 0% in 2000 to 4.0% during 2010 (p<0.001), and the percentage of isolates with ceftriaxone MICs ≥0.125 μg/mL increased from 0% to 0.9% (p<0.001). Overall, no statistically significant increases occurred in cefixime or ceftriaxone MICs among men who have sex exclusively with women.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
