Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Suicides in National Parks --- United States, 2003--2009
In 2007, the year for which the most recent national data on fatalities are available, 34,598 suicides occurred in the United States (rate: 11.3 per 100,000 population); 79% were among males (1). In 2009, an estimated 374,486 visits to hospital emergency departments occurred for self-inflicted injury, of which approximately 262,000 (70%) could be attributed to suicidal behavior (1,2). The majority (58%) were among females. Most suicides (77%) occur in the home (3), but many occur in public places, including national parks. In addition to the loss of life, suicides consume park resources and staff time and can traumatize witnesses. To describe the characteristics of and trends in suicides in national parks, CDC and the National Park Service (NPS) analyzed reports of suicide events (suicides and attempted suicides) occurring in the parks during 2003--2009. During this 7-year span, 84 national parks reported 286 suicide events, an average of 41 events per year. Of the 286 events, 68% were fatal. The two most commonly used methods were firearms and falls. Consistent with national patterns, 83% of suicides were among males. A comprehensive, multicomponent approach is recommended to prevent suicide events, including enhanced training for park employees, site-specific barriers, and collaboration with communities.
The national park system comprises 393 parks, including historic sites, monuments, preserves, lakeshores, seashores, reserves, rivers, riverways, scenic trails, military parks, battlefields, memorials, recreations areas, and parkways, in 49 states (all but Delaware), the District of Columbia, American Samoa, Guam, Puerto Rico, Saipan, and the U.S. Virgin Islands. NPS routinely collects reports on serious incidents that occur within the park system, including suicide events. Suicide events in national parks are reported through the NPS serious incident notification system. NPS reporting criteria are based on an incident management system that classifies events by type, based on size, location, threat to life and property, political sensitivity, organizational complexity, jurisdictional boundaries, values to be protected, topography, agency policy, and other factors (4). For each incident, a park ranger enters a brief description into the notification system, typically a simple, chronologic narrative. Although many suicide events reported by NPS might appear in other reporting systems (e.g., information from death certificates appears in vital statistics records), the notification system provides information about events that occur specifically in national parks, a unique environment in which the federal government has responsibility and oversight.
For this report, deaths during 2003--2009 that occurred in national parks were identified as suicides if a ranger and/or law enforcement personnel determined that the deceased person took his or her own life. Cases were listed as attempted suicide if rangers or law enforcement determined that the person had tried to take his or her own life (e.g., jumped from a bridge, but survived) or when it appeared likely that the person was attempting suicide (e.g., intent stated, but action not taken). A suicide event was defined as either a suicide or an attempted suicide.
Cases were identified from 2003--2009 NPS reports based on text string searches (e.g., suicide; attempted suicide; end or take own life). Each matching report was reviewed, and specific data elements were abstracted (e.g., victim age and sex, date of incident, and suicide or attempted suicide method). For 10 of the 194 deaths coded as suicide, a cause of death was not determined, but sufficient evidence was found to believe a suicide had occurred (e.g., a suicide note was found in an abandoned car in a remote area of a park). The method used in the suicide event was converted to standard International Classification of Diseases, 10th Revision coding terms (e.g., jump = fall, hanging = suffocation, automobile crash = transportation, and knife wound = cut/pierce). Poisoning cases include drug overdoses. Because reporting is done via narrative and not defined data elements, information was missing from some reports (e.g., age was missing in 35% of the cases, method was not specified in 13% of cases, and sex was missing in 2% of the cases).
During 2003--2009, 286 suicide events were reported from a total of 84 parks; 194 (68%) were suicides, and 92 (32%) were attempted suicide. The number of suicides in specific parks ranged from zero to 15 (Table 1). Six (7%) of 84 parks had 10 or more events (suicide and attempted suicide). Blue Ridge Parkway and Grand Canyon National Park had the most events (21 each) during 2003--2009. Approximately 19% of the events involved a fall (typically a jump from a cliff or bridge), and 6% were transportation related (e.g., driving over a cliff). In contrast, 2% of all suicides nationally were fall related, and <1% were transportation related (1).
Among 194 suicides in the parks, 83% were among males. Nationally, in 2007, 79% of all suicides were among males (1). The mean age of persons who committed or attempted suicide in the parks was 43 years (range: 16--84 years). The highest number of suicides occurred in June (22), August (21), and January (21). The highest number of attempted suicides occurred in July (17), followed by May (11). The six most commonly reported suicide methods overall were firearm (33%), fall (19%), suffocation (9%), poisoning (7%), cut/pierce (6%), and transportation (6%). The three most commonly reported methods for males were firearm (36%), fall (19%), and suffocation (10%), and for females they were firearm (21%), fall (19%), and poisoning (16%) (Table 2). More than one method was noted for 8% of suicide events. During 2003--2009, the NPS averaged 28 suicides (range: 22--37) and 13 attempted suicides (range: 7--21) annually, with no evident temporal trend (Figure), although the number of suicides and attempted suicides both increased from 2007 to 2009.
Reported by
S Newman, DrPH, National Park Svc, Washington, DC. E Akre, MA, Suffolk Univ, Boston, Massachusetts. R Bossarte, PhD, Univ of Rochester, New York. K Mack, PhD, A Crosby, MD, National Center for Injury Prevention and Control, CDC.
Editorial Note
A previous report examined deaths in U.S. national parks during 2003--2004 (5), but this is the first report to focus on the characteristics of suicide events in U.S. national parks. Although the total number of deaths attributed to suicide that occurred in national parks during 2003--2009 is small, each death represents a preventable event in a public place. Suicides also can represent a major cost burden for the parks, in one case reaching nearly $200,000 because of the resources and time required to conduct a search for a missing person (NPS, unpublished data 2010).
Park rangers have intervened to prevent suicides; however, their ability to dissuade suicidal visitors is limited. Training programs for park rangers should consider factors such as awareness of and ability to connect to local community prevention programs for information and guidance, and the typically short duration that park rangers interact with visitors. In addition, park rangers cover considerable territory, and the ratio of park visitors per park ranger is high. Enhanced training that focuses on the ability to recognize the signs and symptoms of suicidal behavior, provides strategies for reaching out to persons with problems, and improves the understanding of available treatment might prove useful.
The most successful suicide prevention programs are multifaceted and comprehensive (6). The three general strategies for preventing suicidal behavior include 1) universal approaches (strategies that target the general population including environmental strategies that decrease the availability of harmful means); 2) selected approaches (strategies for specific at-risk groups); and 3) indicated approaches (strategies for at-risk persons who show signs of suicidal potential) (7). Successful suicide prevention programs often include aspects of universal prevention that focus on 1) encouraging and enabling persons to seek help for health and social problems, 2) improving collaboration among community prevention organizations, 3) training professionals and volunteers within the community to identify persons at risk and make referrals when necessary, and 4) enhancing social support for at-risk persons.
Various factors could limit the use of site-specific suicidal behavior interventions in park settings, including characteristics of the location (e.g., public access and engineering complexity of the site), but physical barriers have been used successfully on bridges and some tall structures (8). In Bern, Switzerland, for example, installation of a safety net below a site from which persons had jumped eliminated suicide attempts at that location (8). Given that 19% of the suicide events in parks were fall related, NPS should consider engineering modifications, where practical and consistent with the NPS responsibility to protect natural, cultural, and historic resources, as one component of a suicide prevention strategy. This might include additional pedestrian barriers on bridges or other means to block access to the most common locations. This approach might require an environmental evaluation of possible deterrents, balanced with the NPS mission to retain site access and beauty. Other potential interventions include placing suicide hotline information (e.g., the National Suicide Prevention Lifeline, 1-800-273-TALK [8255]) in kiosks and waysides near high-risk locations and video monitoring at high-risk locations for rapid response. Parks also can seek support and resources from community services to identify appropriate intervention strategies.
The findings in this report are subject to at least three limitations. First, the remote nature of some parks means that some victims were difficult to find, and some deaths might have been handled entirely by local law enforcement personnel who did not then inform park rangers. Therefore, these results likely are an underestimate of the actual number of suicide events. Second, the NPS notification system does not require reporting of standardized data elements, such as age, sex, or method. In addition, no standard environmental investigation was possible for each event. As a result, some useful data were missing. Finally, reported suicide death data from NPS have not been validated against vital statistics. Therefore, some deaths might have been misclassified. Further evaluation of NPS surveillance would be useful.
In light of strategies proven effective for suicide prevention and the results of this report, two general approaches are warranted. First, comprehensive strategies in which each park collaborates with community prevention programs to gain increased access to resources, guidance, and training and second, site-specific suicidal behavior interventions such as access barriers and restriction (e.g., physical barriers on bridges) should be considered. Although community-based programs potentially could be effective in reducing the number of at-risk persons who engage in suicidal behavior at national parks, the degree to which such programs can be integrated into NPS prevention efforts requires further study. Several studies have shown that restricting access to a common, lethal, and easily accessible method decreases both the rate of suicides by that method and the overall suicide rate (8,9), indicating that persons do not immediately seek an alternative suicide method. Finally, the approaches used for suicide prevention in national parks need to be assessed to determine their effectiveness in this unique setting.
References
- CDC. WISQARS (Web-based Injury Statistics Query and Reporting System). Atlanta, GA: US Department of Health and Human Services, CDC; 2009. Available at http://www.cdc.gov/injury/wisqars. Accessed June 17, 2009.
- CDC. Nonfatal self-inflicted injuries treated in hospital emergency departments---United States, 2000. MMWR 2002;51:436--8.
- CDC. Surveillance for violent deaths---National Violent Death Reporting System, 16 states, 2007. MMWR 2010;59(No. SS-4).
- National Park Service. Reference manual 55: incident management program. Washington, DC: National Park Service; 2007. Available at http://www.nps.gov/policy/rm55manual.pdf. Accessed November 24, 2010.
- Heggie TW, Heggie TM, Kliewer C. Recreational travel fatalities in US national parks. J Travel Med 2008:15:404--11.
- Knox KL, Conwell Y, Caine ED. If suicide prevention is a public health problem, what are we doing to prevent it? Am J Public Health 2004;94:37--45.
- Goldsmith SK, Pellmar TC, Kleinman AM, Bunney WE, eds. Reducing suicide: a national imperative. Washington, DC: National Academy Press; 2002.
- National Institute for Mental Health in England. Guidance on action to be taken at suicide hotspots. Leeds, UK: National Institute for Mental Health in England; 2006. Available at http://www.nmhdu.org.uk/silo/files/guidance-on-action-to-be-taken-at-suicide-hotspots.pdf. Accessed June 4, 2010.
- Daigle MS. Suicide prevention through means restriction: assessing the risk of substitution. A critical review and synthesis. Accid Anal Prev 2005;37:625--32.
What is already known on this topic?
Suicide is a public health problem that most often occurs in private residences; little is known about suicides and attempted suicides that occur in public settings such as national parks.
What is added by this report?
During 2003--2009, a combined average of 41 suicides and attempted suicides occurred in national parks per year, and they most often involved firearms (33%) or falls (19%), which differed from the methods most commonly used in suicide events in other settings.
What are the implications for public health practice?
Based on findings in this report and strategies proven effective for suicide prevention, two main approaches are recommended to help prevent suicides in national parks: 1) strategies in which parks collaborate with community prevention programs to gain increased access to resources, guidance, and training and 2) feasible and appropriate site-specific suicidal behavior interventions, such as barriers or restrictions to access.
FIGURE. Number of suicides and attempted suicides in national parks, per year --- National Park Service, United States, 2003--2009
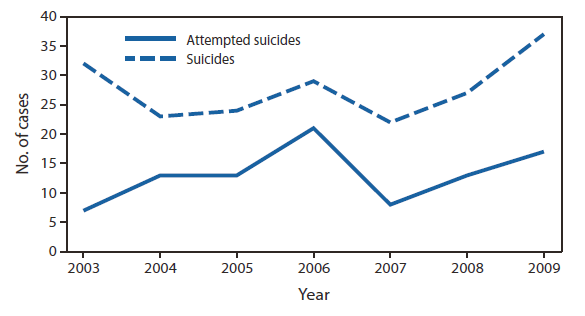
Alternate Text: The figure above shows suicides and attempted suicides in national parks, per year in the United States from 2003-2009. During 2003-2009, the National Park Service averaged 28 suicides (range: 22-37) and 13 attempted suicides (range: 7-21) annually, with no evident temporal trend.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
