Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Public Health Surveillance Using Emergency Medical Service Logs --- U.S.--Mexico Land Border, El Paso, Texas, 2009
In 2008, approximately 358 million travelers entered the United States, of whom 206 million arrived via land ports of entry (POEs) on the U.S.--Mexico border (1). Effective response to infectious diseases of public health importance among travelers requires timely identification and reporting to state and federal health authorities. Currently, notifications are made primarily by U.S. Customs and Border Protection (CBP) officers to CDC quarantine stations. However, CBP personnel have competing priorities and limited public health training (2). To evaluate the utility of monitoring emergency medical service (EMS) dispatch and response logs for ill travelers with symptoms or signs suggestive of infectious diseases, CDC screened medical records of patients transported by EMS during 2009 from the four POEs in El Paso, Texas. The screening was conducted using commercial software that monitors EMS logs and sends alerts in real time based on preestablished criteria (i.e., records containing keywords suggesting infectious diseases). Records that met the criteria were forwarded to El Paso Quarantine Station personnel and reviewed within 24 hours. If a reportable infectious disease was suspected, the final diagnosis was requested from the receiving hospital. This report summarizes the results of the evaluation, which found that, of 50,779 EMS responses in the city of El Paso, 455 (0.9%) records met alert criteria, 86 (0.2%) needed diagnostic confirmation, and nine (<0.1%) were for reportable infectious diseases. Monitoring EMS logs can enhance detection of travelers with serious infections at POEs but requires additional screening and follow-up by CDC.
CDC's Division of Global Migration and Quarantine (DGMQ) is responsible for responding to communicable diseases in arriving international travelers that might pose a public health threat. Effective and timely detection of travelers with reportable infectious diseases is necessary for disease prevention and control measures, such as outbreak and contact investigations (i.e., for infectious tuberculosis and many vaccine preventable diseases) and monitoring of POEs for mass disease events with bioterrorism potential. CDC's El Paso Quarantine Station has one medical officer and one public health advisor who are responsible for responding to these public health threats at 29 POEs spread over 1,200 miles of the U.S.--Mexico border. At POEs, CBP has agreed* to report to CDC quarantine stations any traveler who might have any of a number of clinical syndromes suggestive of an infectious disease of public health importance. However, CBP officers also must screen travelers rapidly for immigration requirements, criminal histories, terrorism intent, and illicit drug trafficking, as well as public health threats, while also permitting entry of persons engaged in commerce, tourism, or other lawful pursuits (2). Because screening and reporting of health threats might be limited by CBP's broad mandate and need for rapid processing of travelers, the Institute of Medicine has suggested that new strategies be pursued to identify travelers for signs of communicable diseases (2).
Use of EMS dispatch and response and emergency department chief complaint data is an efficient way to detect conditions of clinical and public health interest (3,4). The four urban POEs that join El Paso, Texas, and Ciudad Juarez, Chihuahua, Mexico (Bridge of the Americas, Paso Del Norte, Ysleta, and Stanton) are particularly suited to such use because of the large numbers of crossings (31.5 million per year) and because the El Paso Fire Department's computer-assisted dispatch and response system integrates both 911 call center data and EMS clinical findings into a single electronic patient record.
In this study, CDC evaluated the utility of monitoring El Paso Fire Department patient records using commercial software (FirstWatch, FirstWatch Solutions Corporation, Encinitas, California) that monitors EMS records in real time and sends an alert if the record meets the following criteria: 1) EMS response to one of the four POEs and 2) at least one keyword suggesting infection.† When EMS records matched these criteria, they were sent automatically by e-mail to the quarantine station medical officer, who reviewed the information in the alert (date, location of patient, chief complaint, and a brief summary of medical clinical) within 24 hours. If an infection reportable to the city of El Paso, Texas, or New Mexico health departments was considered possible, the El Paso Quarantine Station contacted the relevant hospital to obtain the final diagnosis. A final diagnosis was not requested for patients primarily transported for intentional or unintentional injuries, or for labor and obstetric conditions. These diagnoses were received within 24 hours for most patients. The primary diagnosis was then coded by CDC using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) (Table). To determine whether any of these patients had been reported previously to CDC by CBP, information was extracted from CDC's Quarantine and Activity Reporting System (QARS), in which all illnesses, deaths, and other port-related public health events reported to quarantine station staff members are recorded.
During 2009, El Paso EMS made 50,779 calls, of which 898 (1.8%) were to the four border crossings. Of these 898 calls, 455 (50.7%%) met the alert criteria. Review of the alerts led to final diagnoses being requested for 86 (9.6%) patients. Reportable infectious diseases were identified in nine (10.5%) of the 86 patients, including pandemic influenza A (H1N1) (five cases), coccidiodomycosis, Legionnaires disease, and invasive Streptococcus pneumoniae; nonreportable infectious diseases (e.g., urinary tract infection, bronchitis, osteomyelitis) were identified in 31 (36.0%); and a noninfectious condition in 46 (53.5%) (Table). Reportable infectious diseases were clustered in the fall, coinciding with the H1N1 epidemic (Figure).
During the same period, 295 notifications in QARS involved the jurisdiction of the El Paso Quarantine Station. Of these, 27 (9.1%) were from CPB officers at the four POEs covered by El Paso EMS. Among those 27 patients, two (7.4%) had reportable infectious diseases (tuberculosis, Hansen disease), 15 (55.6%) had nonreportable infectious diseases, and 10 (37.0%) had noninfectious conditions. Only two (2.3%) of the 86 travelers for whom a final diagnosis was requested and none of the nine patients with reportable infectious diseases were reported to the El Paso Quarantine Station by CBP.
Reported by
D Fishbein, MD, M Sandoval, MPH, C Wright, MPH, S Herrera, MPH, S Reese, MPH, T Wilson, MS, M Escobedo, MD, S Waterman, MD, S Modi, MD, J Keir, MPH, H Lipman, PhD, Div of Global Migration and Quarantine, National Center for Emerging and Zoonotic Infectious Diseases; D Sugerman, MD, EIS Officer, CDC.
Editorial Note
The large volume of travelers crossing at international POEs makes identification and reporting of infectious diseases difficult. The results of this analysis indicate that use of EMS dispatch and response logs more than doubled the number of reports of probable infectious diseases identified and reported from the El Paso POEs, and increased by more than fivefold (from two to 11) the number of reportable diseases identified and reported. By identifying these patients at the time they were transported, the El Paso Quarantine Station was able to contact the receiving hospital and identify suspected cases while the patients were enroute to the hospital. Reportable diseases were identified shortly after the diagnosis was made and before they were reported to other health authorities by the hospitals.
In addition to increasing the level of detection, automated monitoring of EMS response logs has the advantage of fostering interagency collaboration without relying on additional human resources. Neither EMS nor CBP personnel needed to add to their workloads to report these cases because case information was entered automatically into a computerized database and analyzed in real time, and cases of possible infectious disease were reported by e-mail to the El Paso Quarantine Station for evaluation.
Although the use of EMS data in the early detection of reportable infectious diseases has not been studied previously, EMS data have been found to be a useful means for real-time syndromic surveillance for early detection of outbreaks and specific health conditions (3,4). In a study in Denmark, increased frequency of ambulance transport served to identify an influenza outbreak before it was recognized by other surveillance systems (3). In New York City, EMS diagnoses of difficulty breathing were 86.4% sensitive and 86.6% specific for cardiac disease, and 71.4% sensitive and 93.6% specific for pulmonary disease (3,4). However, implementation of syndromic surveillance systems should be weighed carefully against their potential public health utility (5) and cost to public health agencies.
In spite of the rapid identification of a number of reportable infectious diseases through surveillance of EMS logs, the number of cases identified was small and most did not require an immediate public health response. CBP did not report the majority of cases transported by EMS. This might be expected, given the relatively brief period available to CBP for detection of ill travelers as they transit through ports of entry. Although CBP officers are trained to identify and report travelers who appear ill with syndromic conditions such as those included in this study, most of the clinical information was not collected until the patients were evaluated by EMS. Unless the illness is plainly visible and unambiguous, or travelers indicate that they are ill, in most cases CBP cannot detect illnesses of public health significance at the border. For travelers with medical emergencies, the focus is always on prompt transport of patients who require immediate medical care.
This study also highlights the difficulty of detecting infectious diseases at the time infected travelers enter the United States (6--9). The large expanse of U.S. national borders, large number of crossings, limited federal resources, and need to allow the rapid movement of people and cargo make binational surveillance systems essential. Since 1997, CDC, the Mexican Secretariat of Health, and border health officials have implemented a variety of surveillance systems for infectious diseases as part of the Border Infectious Disease Surveillance (BIDS) project (8). One such sentinel influenza surveillance site in Imperial County, California, near the U.S.--Mexico border, was responsible for detecting one of the first two cases of 2009 influenza A (H1N1) (10).
The findings in this report are subject to at least three limitations. First, the reported number of patients detected with an infectious disease likely greatly underestimates the true number of imported infections, because generally only those illnesses that pose immediate threats to life required transport by EMS. Second, when such patients are transported, EMS personnel do not measure body temperatures routinely to screen for fever, a crucial first step in nearly every infectious disease syndromic algorithm, and confirmation of most reportable diseases requires diagnostic tests not usually available on ambulances. Finally, surveillance systems based on symptoms and signs of illness cannot detect asymptomatic infections, nor most infectious diseases with protean symptoms.
The results of this study suggest that automated surveillance of EMS logs can enhance detection of reportable infections at POEs and supplement existing public health surveillance. To determine the ultimate value of this system, longer periods of study and refinement of the keyword search strategy based on performance characteristics are needed to determine whether travelers with conditions of greater importance to public health can be detected by this system. Surveillance based on EMS logs is only one component of a system that must include binational cooperation, data sharing, notification, reporting, continuity of care, and preparedness. Systems to detect infectious disease in immigrants and refugees before international travel begins or after it is completed also are an essential part of surveillance. This is especially important given the modest value of interventions at POEs and the limitations of detecting ill travelers en route.
Acknowledgments
This report is based, in part, on contributions by J Walker, D Sharp, and C Celaya, El Paso Fire/Emergency Medical Services Dept; L Escobedo, MD, Texas Dept of State Health Svcs Region 9/10; F Averhoff, MD, N Cohen, MD, and J Rueda, Div of Global Migration and Quarantine, National Center for Zoonotic and Emerging Infectious Diseases, CDC.
References
- Research and Innovation Technology Administration. U.S. border crossings [Database].Washington, DC: US Department of Transportation, Research and Innovation Technology Administration; 2010. Available at http://www.transtats.bts.gov/bordercrossing.aspx. Accessed April 1, 2010.
- Institute of Medicine. Quarantine stations at ports of entry: protecting the public's health. Washington, DC: National Academy Press; 2005.
- Bork KH, Klein BM, Molbak K, Trautner S, Pedersen UB, Heegaard E. Surveillance of ambulance dispatch data as a tool for early warning. Euro Surveill 2006;11:229--33.
- Ackerman R, Waldron RL. Difficulty breathing: agreement of paramedic and emergency physician diagnoses. Prehosp Emerg Care 2006;10:77--80.
- Reingold A. If syndromic surveillance is the answer, what is the question? Biosecur Bioterror 2003;1:77--81.
- Government Accountability Office. Public health and border security: HHS and DHS should further strengthen their ability to respond to tuberculosis incidents. Washington, DC: Government Accountability Office; 2008. Available at http://www.gao.gov/new.items/d0958.pdf. Accessed April 11, 2010.
- Waterman SH, Escobedo M, Wilson T, et al. A new paradigm for quarantine and public health activities at land borders: opportunities and challenges. Public Health Rep 2009; 124:203--11.
- Weinberg M, Waterman S, Lucas CA, et al. The U.S.--Mexico Border Infectious Disease Surveillance project: establishing bi-national border surveillance. Emerg Infect Dis 2003;9:97--102.
- Cain KP, Benoit SR, Winston CA, MacKenzie WR. Tuberculosis among foreign-born persons in the United States. JAMA 2008;300:405--12.
- CDC. Swine influenza A (H1N1) infection in two children---southern California, March--April 2009. MMWR 2009;58:400--2.
* Memorandum of understanding between the Department of Health and Human Services and the Department of Homeland Security; October 19, 2005.Additional information on relevant regulations is available at http://www.cdc.gov/quarantine/specificlawsregulations.html.
† Keywords were as follows: Gastrointestinal group: abdominal pain, stomach pain/ache, cramping, nausea, vomiting, diarrhea, bloody diarrhea, loose stools, decreased appetite, jaundice, botulism, cholera, Clostridium, cryptosporidiosis, salmonellosis, shigellosis, hepatitis A, norovirus, typhoid fever, weight loss; Respiratory group: influenza, tuberculosis, cough, cough with blood, sore throat, congestion, shortness of breath, breathing problems, difficulty breathing, influenza (flu), Legionnaires disease, melioidosis, pertussis, whooping cough, SARS, tularemia, anthrax; Dermatologic group: varicella, chickenpox, rash, redness of skin, swelling, sores, inflammation, discolorations, bumps, blisters, skin disorder, cutaneous anthrax, ulcers, hand foot mouth disease, measles, mumps, rubella, smallpox, shingles, MRSA, methicillin-resistant Staphylococcus aureus, Staphylococcus; Systemic group: fever, febrile, elevated temperature, warm/hot, flushed, chills, clammy, sweating, infection, yellow fever, lymphadenopathy, brucellosis; muscle ache, diphtheria, malaria; plague, psittacosis, Q-fever, muscle ache, weakness; Central nervous group: polio, stiff neck, headache, meningitis, meningococcal disease, rabies, encephalitides; Hemorrhagic group: hemorrhage, nose bleed, bleeding, bruising, mucosal bleeding, headache, red eyes, dengue.
What is already known on this topic?
U.S. Customs and Border Protection (CBP) officers, whose primary task is law enforcement, also watch for and report illnesses of public health importance among approximately 206 million travelers who enter the United States across U.S.--Mexico land border each year.
What is added by this report?
The El Paso Quarantine Station used a real-time commercial software system that monitors emergency medical service (EMS) logs to identify possible infectious diseases reportable to local and state health authorities. Nine patients crossing the border with reportable diseases were detected; none had been reported to the El Paso Quarantine Station by CBP officers.
What are the implications for public health practice?
Although automated monitoring of EMS logs can enhance detection of reportable infectious diseases in travelers, the yield is low and substantial additional screening and follow-up is needed by CDC.
FIGURE. Number of emergency medical service calls prompting alert and follow-up for possible infectious disease, by month and final diagnosis --- U.S.--Mexico land border crossings, El Paso, Texas, 2009
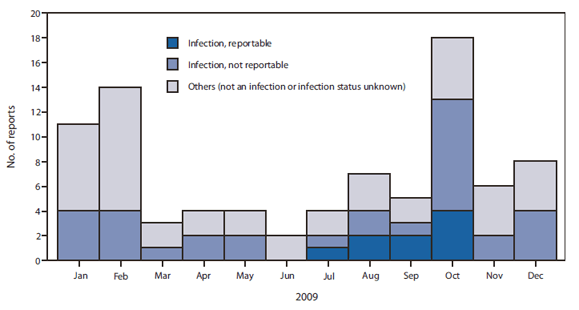
Alternate Text: The figure above shows the number of emergency medical service calls prompting alert and follow up for possible infectious disease, by month and final diagnosis, from the four U.S.-Mexico land border crossings in El Paso, Texas, in 2009. During 2009, El Paso emergency medical services made 50,779 calls, of which 898 (1.8%) were to the four border crossings. Of these 898 calls, 455 (50.7%) met the alert criteria. Review of the alerts led to final diagnoses being requested for 86 (9.6%) patients. Reportable infectious diseases were identified in nine (10.5%) of the 86 patients, including pandemic influenza A (H1N1) (five cases), coccidiodomycosis, Legionnaires disease, and invasive Streptococcus pneumoniae; nonreportable infectious diseases (e.g., urinary tract infection, bronchitis, osteomyelitis) were identified in 31 (36.0%); and a noninfectious condition in 46 (53.5%). Reportable infectious diseases were clustered in the fall, coinciding with the H1N1 epidemic.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
