Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Effects of Switching from Whole to Low-Fat/Fat-Free Milk in Public Schools --- New York City, 2004--2009
In 2005, the New York City (NYC) Department of Education (DOE) began reviewing its public school food policies to determine whether changes could help address the increasing prevalence of childhood obesity in NYC (1). DOE determined that reducing consumption of whole milk and increasing consumption of fat-free or low-fat milk could help decrease students' fat and calorie intake while maintaining calcium consumption. However, milk industry advocates and others expressed concern that phasing out whole milk might decrease overall student demand for milk. Nevertheless, during 2005--2006, DOE removed whole milk from cafeterias in all public schools serving the city's approximately 1.1 million schoolchildren. To assess the effects of the switch on milk consumption, the NYC Department of Health and Mental Hygiene (DOHMH) analyzed system-wide school milk purchasing data. This report summarizes the results of that analysis, which indicated that DOE school milk purchases per student per year increased 1.3% in fiscal year 2009 compared with 2004 purchases. By removing whole milk and switching from low-fat to fat-free chocolate milk, NYC public school milk-drinking students were served an estimated 5,960 fewer calories and 619 fewer grams of fat in 2009 than they were in 2004. Other school systems can use these results to guide changes to their own school food policies.
Various types of milk have been available to all NYC public school students during lunch (Table 1). Milk is not available in school vending machines. The switch from whole to low-fat or fat-free milk began in the borough of the Bronx in 2004, when several elementary school principals, in response to community-based public health efforts, began limiting the availability of whole and/or sweetened, flavored (e.g., chocolate and strawberry) milk. At the same time, DOE was reevaluating its school food policies. DOE and these elementary school principals, in collaboration with the DOHMH Bronx District Public Health Office, local community organizations, and other local advocates, convened meetings to assess the feasibility and potential health impact of limiting the availability of whole milk in schools. At these meetings, milk industry advocates and others suggested that without whole and sweetened, flavored milk in cafeterias, student milk consumption would decline, thereby decreasing the amount of calcium consumed. Nevertheless, in the fall of 2005, DOE phased out whole milk products and limited sweetened milk to fat-free chocolate in all five NYC boroughs. In 2004, sweetened, flavored milk was available in low-fat varieties, and flavors other than chocolate had limited availability. After the switch, only chocolate milk was retained because of its popularity among students but was changed from low-fat to fat-free. The milk changes began in the Bronx and Manhattan in the fall of 2005, and in Queens, Brooklyn, and Staten Island in February 2006. Fiscal year 2006* was the first full school year in which whole milk was phased out in all five boroughs.
No data were available on student consumption of milk. Therefore, as a proxy, school system purchasing data provided by the DOE Office of School Food were used to approximate consumption. To calculate the annual calories and fat available from milk, the number of fat-content/flavor-specific (e.g., whole white, low-fat white, and fat-free chocolate) units purchased by DOE per year was multiplied by milk type--specific fat and calorie information (Table 1). These results were summed to yield the total number of calories and grams of fat from milk purchased by DOE. These sums were then distributed across various student types (e.g., all enrolled students or milk-drinking students) to estimate changes in annual and daily milk fat/calorie exposure (Table 2).†
From 2004 to 2006, total DOE per student school milk purchases declined 8% (Figure). However, purchases then gradually began increasing, and by 2009, DOE per student milk purchases (adjusted for school system enrollment) had increased 1.3%, from 112 per student in 2004 to nearly 114 in 2009.
Whole milk accounted for 33% of all DOE milk purchases in 2004, whereas in 2009 it accounted for less than 2% (some whole milk was still used in special education sites and for catering). Conversely, low-fat or fat-free white milk purchases in 2009 accounted for 42% of all DOE milk purchases (35% and 7%, respectively), compared with less than 7% (4% and 2%, respectively) in 2004. The proportion of sweetened, chocolate milk purchased remained stable, accounting for 61% of DOE orders in 2004 and 57% in 2009.
In 2004, approximately 18.3 billion calories and 520 million grams of fat were purchased by DOE in the form of milk. In 2009, as a result of DOE's switch to lower-fat milk, those numbers decreased to 13.7 billion calories and 98 million grams of fat, representing a 25% and 81% decline in available calories and fat from milk, respectively. Comparing 2004 with 2009, if calorie and fat savings were distributed over all enrolled students, 3,484 fewer calories and 382 fewer grams of fat were averted each school year as a result of the milk policy change. When distribution of fat and calories from milk were limited to the percentage of students who were estimated to drink milk during the school day (62% in 2004 and 63% in 2009), these savings increased to 5,960 calories and 619 fat grams per year. The analysis also determined the calorie and fat grams averted per year for students estimated to drink white milk (7,089 calories and 922 grams of fat) and to drink chocolate milk (4,900 calories and 448 grams of fat) once per school day.
Reported by
PM Alberti, PhD, SE Perlman, MPH, C Nonas, J Hadler, MD, J Choe, MPH, JF Bedell, MD, New York City Dept of Health and Mental Hygiene; H McKie, MS, New York City Dept of Education.
Editorial Note
The goal of the milk policy change for NYC public schools was to reduce a key source of dietary calories and fat without reducing the total amount of milk purchased per student, recognizing that school milk provides an important source of protein, calcium, and vitamins such as A and D. The results presented in this report show that the switch from whole milk to low-fat or fat-free milk accomplished this goal. For each milk-drinking student, 5,960 calories and 619 grams of fat were averted per school year after the policy change. Although studies have shown that schools across the nation have switched from whole to lower-fat milk options in recent years (2) and that changes to school food policies improve the kinds of food available to students and reduce overall calories and fat available (3,4), this is the first published estimate of reductions in calories and fat from a policy switch in available milk products.
The amount of sweetened, chocolate milk being consumed by students is a matter of concern. Low-fat and fat-free chocolate milk have more calories than reduced-fat white milk and contain twice the amount of sugars. Limiting chocolate milk availability would reduce further the number of calories served to students by approximately 23%.§ However, chocolate milk is popular among students and accounted for approximately 60% of milk purchases both before and after the milk policy change in NYC. A study in Connecticut showed that after eliminating sweetened, flavored milk from school cafeterias, student milk consumption declined 60% (5). Removing chocolate milk from the cafeteria line in NYC schools might result in decreased milk consumption (and therefore decreased calcium consumption). Further research should investigate the health impact of sweetened chocolate milk restrictions in NYC.
The findings in this report are subject to at least three limitations. First, although milk purchasing certainly correlates with milk consumption, data are not available to assess the magnitude of that correlation. Some of the milk taken from the cafeteria line might be thrown away, and formal "plate waste" studies have not been conducted in NYC. Second, no data were collected on total food consumption during the school day, so the effect of the milk switch on overall diet is unknown. Students might compensate for the averted calories/fat from milk by changing their consumption patterns. Finally, data were not readily available to allow stratification by grade level (e.g., elementary, middle, and high school).
Changes to the physical environment often are the most effective interventions to improve population health (6,7). The switch to lower-fat milk likely has improved the overall nutritional environment of NYC public schoolchildren. The switch also might promote changes in children's taste preferences toward lower-fat milk.
References
- Egger JR, Bartley KF, Benson L, Bellino D, Kerker B. Childhood obesity is a serious concern in New York City: higher levels of fitness associated with better academic performance. NYC Vital Signs 2009;8:1--4. Available at http://www.nyc.gov/html/doh/downloads/pdf/survey/survey-2009fitnessgram.pdf. Accessed January 21, 2010.
- US Department of Agriculture. School Nutrition Dietary Assessment study-III: vol. 1: school foodservice, school food environment, and meals offered and served. Washington, DC: US Department of Agriculture; 2007. Available at http://www.fns.usda.gov/ora/menu/published/cnp/files/sndaiii-vol1execsum.pdf. Accessed January 26, 2010.
- Cullen KW, Watson KB. The impact of the Texas public school nutrition policy on student food selection and sales in Texas. Am J Public Health 2009;99:706--12.
- Hanagriff RD, Murphy TH. 2006-2007 School year assessment of the Texas Public School Nutrition Policy: menu analysis. Austin, TX: Texas Department of Agriculture; 2007. Available at http://www.squaremeals.org/vgn/tda/files/2348/20013_Square_Meals_Menu_Analysis_2007_Report_FINAL.pdf. Accessed January 21, 2010.
- Saidel M, Patterson J. The removal of flavored milk in schools results in a decline in total milk purchases in all grades, K-12. Poster presented at American Dietetic Association 2009 Food and Nutrition Conference and Exposition; Denver, CO; October 17--20, 2009.
- World Health Organization. Road safety. In: Peden M, Scurfield R, Sleet D, et al., eds. World report on road traffic injury prevention. Geneva, Switzerland: World Health Organization; 2004. Available at http://www.who.int/violence_injury_prevention/publications/road_traffic/world_report/summary_en_rev.pdf. Accessed January 21, 2010.
- CDC. Ten great public health achievements---United States, 1900--1999. MMWR 1999;48:241--3.
* All years refer to fiscal years which span from July 1 of the previous year through June 30 of the year indicated.
† The amount of milk served to students in schools was assumed to be equal to the amount of milk purchased by DOE, with no wastage. Reductions in annual milk calories and fat per student were calculated as the differences between 2004 calories/fat served per student and 2009 calories/fat served per student. Calorie and fat calculations were based on school system--wide DOE milk purchases (whole white, 1% white, fat-free white, 1% chocolate, and fat-free chocolate) in each of these years and on nutritional information for each of these milk types. In 2004, a total of 18.3 billion calories and 519 million grams of fat in the form of milk were served by DOE, and in 2009, a total of 13.7 billion calories and 98 million grams of fat were served. To arrive at per student figures, these calorie and fat amounts were divided by the total number of New York City public school students in 2004 (1,086,886) and 2009 (1,029,459).
Annual calories and fat served per milk-drinking student were calculated by first determining the percentage of students who drink milk in school. Actual DOE milk purchases (121,854,769 units in 2004 and 117,000,859 units in 2009) were divided by the 181 days in the school year to determine units purchased by DOE per school day (67,323 units in 2004 and 64,641 units in 2009). These units purchased were then divided by the total number of public school students to estimate the percent of students drinking milk once per day (62% in 2004 and 63% in 2009). Total calories and fat served (from the annual number divided by 181 school days) were then divided by these new denominators (673,869 students in 2004 and 648,559 in 2009), and differences in estimated consumption between 2004 and 2009 were calculated.
The proportion of milk purchased by DOE that was white (39% of all milk in 2004 and 43% of all milk in 2009) was assumed to equal the proportion of students who drank white milk. The number of calories and fat from DOE white milk purchases in 2004 (6.7 billion and 335 million, respectively) and 2009 (5.1 billion, and 98 million, respectively) were divided by the estimated number of white milk drinkers (262,809 in 2004 and 278,880 in 2009), and differences in consumption between 2004 and 2009 were calculated.
Calculations were identical to the calculations described previously using chocolate milk calories/fat served (11.6 billion and 184 million in 2004, respectively, and 8.6 billion and 1,750 in 2009, respectively) and number of estimated chocolate milk drinkers (411,060 in 2004 and 369,679 in 2009).
§ Calculation based on converting 2009 fat-free chocolate milk purchases to fat-free white milk purchases. Total calories would decrease from 13.7 billion to 10.6 billion.
|
What is already known on this topic? The prevalence of childhood obesity is increasing, and switching from whole milk to low-fat or fat-free milk has been suggested as one way to reduce children's intake of excess fat and calories. What is added by this report? Milk policy changes in New York City public schools decreased the amount of fat and calories apparently consumed by students without decreasing overall school milk purchases, thereby maintaining student consumption of calcium and important vitamins. What are the implications for public health practice? These results suggest that substitution of low-fat and fat-free milk for whole milk in schools can substantively reduce student consumption of calories and fat. |
FIGURE. Annual half-pint milk purchases per student (adjusted for enrollment), by fat content/flavor --- New York City public schools, fiscal years 2004--2009*
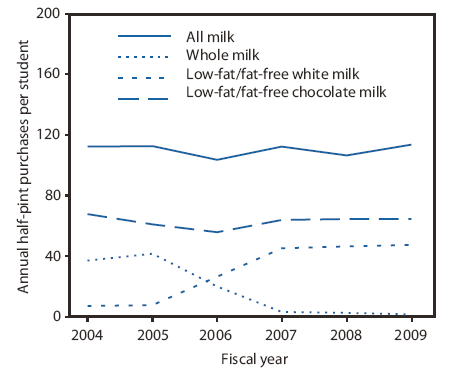
* Because no data were available on student consumption of milk, as a proxy, school system purchasing data provided by the New York City Department of Education Office of School Food were used to approximate consumption.
Alternate Text: The figure above shows the annual half-pint milk purchases per student (adjusted for enrollment), by fat content and flavor in New York City public schools for fiscal years 2004-2009. From 2004 to 2006, total per student school milk purchases declined 8%. However, purchases then gradually began increasing, and by 2009, per student milk purchases (adjusted for school system enrollment) had increased 1.3%, from 112 per student in 2004 to nearly 114 in 2009.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
