Key points
- Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a serious and often long-lasting illness that keeps people from doing their usual activities.
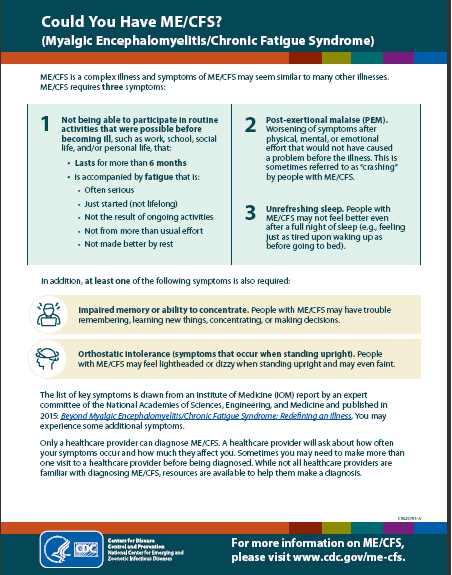
- It makes physical and mental exertion difficult.
- Symptoms include trouble thinking, severe tiredness and other symptoms.
- There is no known cause or cure. Care usually means treating the symptoms that most affect a person's life.

Overview
ME/CFS is a biological illness that affects many body parts. It causes severe fatigue not improved by rest, problems thinking and sleeping, dizziness, pain, and many other symptoms.
People with ME/CFS may not look sick but can't do their normal activities. ME/CFS may get worse after they do any activity -- physical or mental. This symptom is called post-exertional malaise (PEM). After they exert themselves, they may need to stay in bed for an extended time. About 1 in 4 people with ME/CFS are confined to bed at some point in their illness.
It is difficult to diagnose because there is no specific test for ME/CFS. One reason that people with ME/CFS have not been diagnosed may be limited access to healthcare. Another reason may be a lack of healthcare providers who know about ME/CFS and how to recognize it.
Anyone can get ME/CFS. It doesn't matter what age, gender or ethnicity they are. However, some groups are more affected than others.
Signs and symptoms
People with ME/CFS are not able to function the same way they did before they became ill. They may not always be able to do daily tasks like showering or cooking a meal.
ME/CFS often makes it hard to keep a job, go to school, and take part in family and social life. ME/CFS can last for years and sometimes leads to serious disability.
ME/CFS is most common in people in middle age but also affects kids, teens and elderly people. Among adults, women are affected more often than men. Among children, teens are more affected than younger kids.
People who are white are diagnosed more often than other races and ethnicities. But many people with ME/CFS have not been diagnosed, especially among people from racial and ethnic minority groups.
Diagnosis
Symptoms of ME/CFS may appear similar to many other illnesses. There is no test to confirm ME/CFS. This makes it difficult to diagnose. The illness can also be unpredictable. Symptoms may come and go, or there may be changes in how severe symptoms are over time.
A doctor should be able to distinguish ME/CFS from other illnesses by doing a thorough medical exam. This includes asking many questions about the patient's health history and current illness. They should also ask about how often symptoms occur, how bad they are, and how long they have lasted. It is also important for doctors to talk with patients about how the symptoms affect their lives.
Treatment and recovery
There is no cure or approved treatment for ME/CFS. But some symptoms can be treated or managed. Treating these symptoms might provide relief for some people with ME/CFS but not others. Other strategies, like learning new ways to manage activity, can also help.
People with ME/CFS, their families, and healthcare providers need to work together to decide which symptom causes the most problems. This should be treated first after discussing possible benefits and harms of any treatment plans, including medicines and other therapies.
Healthcare providers need to support their patients' families as they come to understand how to live with this illness. Providers and families should remember that this process is likely to be hard on people with ME/CFS.