Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Recommended Adult Immunization Schedule — United States, 2012
Each year, the Advisory Committee on Immunization Practices (ACIP) reviews the recommended adult immunization schedule to ensure that the schedule reflects current recommendations for licensed vaccines. In October 2011, ACIP approved the adult immunization schedule for 2012, which includes several changes from 2011. A footnote directing readers to links for the full ACIP vaccine recommendations and where to find additional information on specific vaccine recommendations for travelers is now included. In addition, a Table summarizing precautions and contraindications was added. This table is based on the corresponding table in the 12th edition of Epidemiology and Prevention of Vaccine-Preventable Diseases and is included to provide ready access to key safety information for adult vaccine providers (1).
Changes to the footnote for tetanus, diphtheria, and acellular pertussis (Tdap) and tetanus, diphtheria (Td) vaccines were made to update recommendations. Tdap vaccine is recommended specifically for persons who are close contacts of infants younger than 12 months of age (e.g., parents, grandparents, and child-care providers) and who have not received Tdap previously. Before 2011, vaccination postpartum was preferred for women who had not had a previous adult Tdap dose. However, in 2011, ACIP recommended pregnant women preferentially receive Tdap vaccination during later pregnancy (>20 weeks gestation). Other adults who are close contacts of children younger than 12 months of age continue to be recommended to receive a one-time dose of Tdap vaccine.
Updates to the footnotes and figures also were made for human papillomavirus (HPV) and hepatitis B vaccines based on recommendations made at the October 2011 ACIP meeting. The HPV vaccine recommendation has been updated to include routine vaccination of males 11–12 years of age, with catch-up vaccination recommended for males 13–21 years of age. HPV vaccine also is recommended for previously unvaccinated males 22–26 years of age who are immunocompromised, or who test positive for human immunodeficiency virus (HIV) infection, or who have sex with men.
ACIP also voted in October 2011 to recommend hepatitis B vaccine for adults <60 years of age who have diabetes, as soon as possible after diabetes is diagnosed. In addition, hepatitis B vaccination is recommended at the discretion of the treating clinician for adults with diabetes who are 60 years or older based on a patient's likely need for assisted blood glucose monitoring, likelihood of acquiring hepatitis B, and likelihood of immune response to vaccination.
A notation was included for zoster vaccine to acknowledge that the vaccine was recently approved by the Food and Drug Administration (FDA) for administration to persons 50 years of age and older; however, ACIP continues to recommend that vaccination begin at age 60 years. The influenza vaccine footnote was revised to specify age indications for the different licensed formulations of trivalent inactivated influenza vaccine (TIV). The footnote for the measles, mumps, rubella (MMR) vaccine was simplified to focus only on routine use of this vaccine in adults; information on use of the vaccine for outbreak control was removed. Readers are referred to the ACIP MMR recommendations and to the ACIP recommendations for the immunization of health-care personnel regarding the use of MMR vaccine in outbreak settings. Additional information on the use of quadrivalent meningococcal conjugate vaccine (MCV4) and meningococcal polysaccharide vaccine (MPSV4) for specific age and risk groups was added. Minor clarifications also were made to the footnotes for HPV vaccine, varicella vaccine, and pneumococcal polysaccharide vaccine (PPSV).
Additional information is available as follows: 1) immunization schedule (in English and Spanish) at http://www.cdc.gov/vaccines/recs/schedules/adult-schedule.htm; 2) information regarding adult vaccination at http://www.cdc.gov/vaccines/default.htm; 3) ACIP statements for specific vaccines at http://www.cdc.gov/vaccines/pubs/acip-list.htm; and 4) reporting of adverse events at http://www.vaers.hhs.gov or by telephone, 800-822-7967. This schedule also has been presented to the American Academy of Family Physicians, the American College of Physicians, the American College of Obstetricians and Gynecologists and the American College of Nurse- Midwives for approval and publication in their respective journals.
Footnote changes for 2012
- A new footnote (1), "Additional information," has been added to the beginning of the footnotes. This footnote provides links to the full ACIP vaccine recommendations and information on travel requirements that might have been referred to previously in subsequent footnotes.
- The "Influenza vaccination" footnote (2) was revised to clarify that all persons aged 6 months and older can receive TIV and that health-care personnel (HCP) who care for persons requiring a protected environment should receive TIV. HCP younger than 50 years who do not have a contraindication may receive either the live attenuated influenza vaccine or TIV. In addition, age indications for two recently licensed formulations of TIV were included. The link to additional information regarding influenza vaccination has been removed because a link now is provided in footnote 1.
- The "Human papillomavirus (HPV) vaccination" footnote (5) now clarifies that although HPV vaccination is not specifically recommended for HCP, HCP should receive the HPV vaccine if they are in the recommended age group. This footnote also was changed to reflect the recommendation of the quadrivalent human papillomavirus (HPV4) vaccine for males at age 11 or 12 years and catch-up vaccination for males 13 through 21 years of age. Males 22 through 26 years of age may be vaccinated with HPV4 vaccine.
- The "Zoster vaccination" footnote (6) now indicates that while zoster vaccination is not specifically recommended for HCP, HCP should receive the vaccine if they are in the recommended age group. This footnote also acknowledges that the vaccine is FDA-approved for use in persons 50 years and older; however, ACIP continues to recommend that vaccination begin at age 60 years.
- The link in the "Measles, mumps, rubella (MMR) vaccination" footnote (7) that directs the reader to more information about evidence of immunity has been removed. In addition, the information about the use of MMR vaccine in outbreak settings has been removed. Readers are referred to the ACIP MMR recommendations and to the ACIP recommendations for the immunization of health-care personnel regarding the use of MMR vaccine in outbreak settings.
- The "Pneumococcal polysaccharide (PPSV) vaccination" footnote (8) has been revised to include additional examples of functional and anatomic asplenia. Language is included for persons with asymptomatic or symptomatic HIV infection and persons undergoing cancer chemotherapy or who are on other immunosuppressive therapy.
- The "Revaccination with PPSV" footnote (9) has been revised to clarify guidance for those aged 65 years and older who had been vaccinated with PPSV23 before age 65 and for whom at least 5 years has passed since their previous dose.
- The "Meningococcal vaccination" footnote (10) has been revised to include military recruits in the group recommended to receive a single dose of meningococcal vaccine. The language about college students has been clarified to indicate that first-year college students up through age 21 years who are living in residence halls should be vaccinated if they have not received a dose on or after their 16th birthday. Language regarding travel to sub-Saharan Africa and travel to Mecca has been removed, and readers are referred to the footnote on information about vaccines for travelers (1).
- The "Hepatitis B vaccination" footnote (12) has been revised to include persons with diabetes younger than 60 years old and persons 60 years and older based on need for assisted blood glucose monitoring.
- Finally, all footnotes were changed from paragraph form to a bulleted format to provide for greater ease in use of the recommendations.
Figures
- For Figure 1, the bar for Tdap/Td for persons 65 years and older has been changed to a yellow and purple hashed bar to indicate that persons in this age group should receive 1 dose of Tdap if they are a close contact of an infant younger than 12 months of age. However, other persons 65 and older who are not close contacts of infants may receive either Tdap or Td.
- The 19–26 years age group was divided into 19–21 years and 22–26 years age groups. The HPV vaccine bar was split into separate bars for females and males. The recommendation for all males 19–21 years to receive HPV is indicated with a yellow bar, and a purple bar is used for 22–26 year old males to indicate that the vaccine is only for certain high-risk groups.
- For Figure 2, a new column was added for men who have sex with men (MSM) to note in the figure that MSM is an indication for HPV, hepatitis A, and hepatitis B vaccines.
- In addition, the diabetes indication was moved to the same column as chronic kidney disease to accommodate the new recommendation for hepatitis B vaccination of persons with diabetes.
- Because pregnant women not previously vaccinated with Tdap are now preferentially recommended for vaccination with Tdap during later pregnancy (>20 weeks gestation), the yellow bar has been extended across all risk groups.
- The HPV vaccine bar was separated into a bar for females and one for males. The bar for females is unchanged from the previous year except that the bar was extended to include HCP to clarify that HCP who are in the recommended age group for receipt of HPV vaccine are recommended for vaccination.
- Lastly, the HPV vaccine bar for males was added and indicates that all males through age 26 should be vaccinated if they are immunocompromised, have HIV, or are MSM. However, the age indication is through age 21 for males with or without these risk factors.
Reference
- CDC. Epidemiology and prevention of vaccine-preventable diseases. Atkinson W, Wolfe S, Hamborsky J, eds. 12th ed. Washington DC: Public Health Foundation; 2011.
The recommended adult immunization schedule has been approved by the Advisory Committee on Immunization Practices, the American Academy of Family Physicians, the American College of Obstetricians and Gynecologists, the American College of Physicians, and the American College of Nurse-Midwives.
Suggested citation: Centers for Disease Control and Prevention. Recommended adult immunization schedule—United States, 2012. MMWR 2012;61(4).
FIGURE 1. Recommended adult immunization schedule, by vaccine and age group1 — United States, 2012
Alternate Text: The figure above shows the recommended adult immunization schedule, by vaccine and age group in the United States for 2012. For Figure 1, the bar for Tdap/Td for persons 65 years and older has been changed to a yellow and purple hashed bar to indicate that persons in this age group should receive 1 dose of Tdap if they are a close contact of an infant younger than 12 months of age. However, other persons 65 and older who are not close contacts of infants may receive either Tdap or Td.
The 19-26 years age group was divided into 19-21 years and 22-26 years age groups. The HPV vaccine bar was split into separate bars for females and males. The recommendation for all males 19-21 years to receive HPV is indicated with a yellow bar, and a purple bar is used for 22-26 year old males to indicate that the vaccine is only for certain high-risk groups.
FIGURE 2. Vaccines that might be indicated for adults, based on medical and other indications1 — United States, 2012
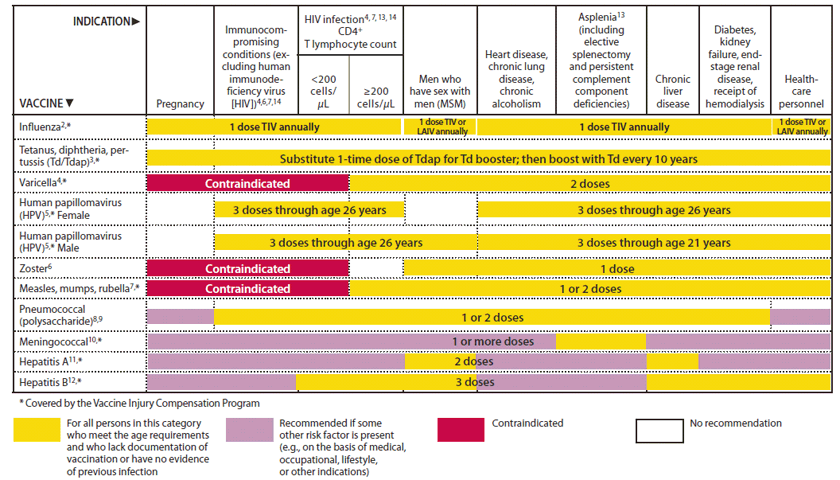
Alternate Text: The figure above shows vaccines that might be indicated for adults, based on medical and other indications in the United States, during 2012. For Figure 2, a new column was added for men who have sex with men (MSM) to note in the figure that MSM is an indication for HPV, hepatitis A, and hepatitis B vaccines.
In addition, the diabetes indication was moved to the same col¬umn as chronic kidney disease to accommodate the new recom¬mendation for hepatitis B vaccination of persons with diabetes.
Because pregnant women not previously vaccinated with Tdap are now preferentially recommended for vaccination with Tdap during later pregnancy (>20 weeks gestation), the yellow bar has been extended across all risk groups.
The HPV vaccine bar was separated into a bar for females and one for males. The bar for females is unchanged from the previous year except that the bar was extended to include HCP to clarify that HCP who are in the recommended age group for receipt of HPV vaccine are recommended for vaccination.
Lastly, the HPV vaccine bar for males was added and indicates that all males through age 26 should be vaccinated if they are immunocompromised, have HIV, or are MSM. However, the age indication is through age 21 for males with or without these risk factors.
1. Additional information
2. Influenza vaccination
-
Annual vaccination against influenza is recommended for all persons 6 months of age and older.
-
Persons 6 months of age and older, including pregnant women, can receive the trivalent inactivated vaccine (TIV).
-
Healthy, nonpregnant adults younger than age 50 years without high-risk medical conditions can receive either intranasally administered live, attenuated influenza vaccine (LAIV) (FluMist), or TIV. Health-care personnel who care for severely immunocompromised persons (i.e., those who require care in a protected environment) should receive TIV rather than LAIV. Other persons should receive TIV.
-
The intramuscular or intradermal administered TIV are options for adults aged 18–64 years.
-
Adults aged 65 years and older can receive the standard dose TIV or the high-dose TIV (Fluzone High-Dose).
3. Tetanus, diphtheria, and acellular pertussis (Td/Tdap) vaccination
-
Administer a one-time dose of Tdap to adults younger than age 65 years who have not received Tdap previously or for whom vaccine status is unknown to replace one of the 10-year Td boosters.
-
Tdap is specifically recommended for the following persons:
— pregnant women more than 20 weeks' gestation,
— adults, regardless of age, who are close contacts of infants younger than age 12 months (e.g., parents, grandparents, or child care providers), and
— health-care personnel.
-
Tdap can be administered regardless of interval since the most recent tetanus or diphtheria-containing vaccine.
-
Pregnant women not vaccinated during pregnancy should receive Tdap immediately postpartum.
-
Adults 65 years and older may receive Tdap.
-
Adults with unknown or incomplete history of completing a 3-dose primary vaccination series with Td-containing vaccines should begin or complete a primary vaccination series. Tdap should be substituted for a single dose of Td in the vaccination series with Tdap preferred as the first dose.
-
For unvaccinated adults, administer the first 2 doses at least 4 weeks apart and the third dose 6–12 months after the second.
-
If incompletely vaccinated (i.e., less than 3 doses), administer remaining doses.
Refer to the ACIP statement for recommendations for administering Td/Tdap as prophylaxis in wound management (See footnote 1).
4. Varicella vaccination
-
All adults without evidence of immunity to varicella (as defined below) should receive 2 doses of single-antigen varicella vaccine or a second dose if they have received only 1 dose.
-
Special consideration for vaccination should be given to those who
— have close contact with persons at high risk for severe disease (e.g., health-care personnel and family contacts of persons with immunocompromising conditions) or
— are at high risk for exposure or transmission (e.g., teachers; child care employees; residents and staff members of institutional settings, including correctional institutions; college students; military personnel; adolescents and adults living in households with children; nonpregnant women of childbearing age; and international travelers).
-
Pregnant women should be assessed for evidence of varicella immunity. Women who do not have evidence of immunity should receive the first dose of varicella vaccine upon completion or termination of pregnancy and before discharge from the health-care facility. The second dose should be administered 4–8 weeks after the first dose.
-
Evidence of immunity to varicella in adults includes any of the following:
— documentation of 2 doses of varicella vaccine at least 4 weeks apart;
— U.S.-born before 1980 (although for health-care personnel and pregnant women, birth before 1980 should not be considered evidence of immunity);
— history of varicella based on diagnosis or verification of varicella by a health-care provider (for a patient reporting a history of or having an atypical case, a mild case, or both, health-care providers should seek either an epidemiologic link to a typical varicella case or to a laboratory-confirmed case or evidence of laboratory confirmation, if it was performed at the time of acute disease);
— history of herpes zoster based on diagnosis or verification of herpes zoster by a health-care provider; or
— laboratory evidence of immunity or laboratory confirmation of disease.
5. Human papillomavirus (HPV) vaccination
-
Two vaccines are licensed for use in females, bivalent HPV vaccine (HPV2) and quadrivalent HPV vaccine (HPV4), and one HPV vaccine for use in males (HPV4).
-
For females, either HPV4 or HPV2 is recommended in a 3-dose series for routine vaccination at 11 or 12 years of age, and for those 13 through 26 years of age, if not previously vaccinated.
-
For males, HPV4 is recommended in a 3-dose series for routine vaccination at 11 or 12 years of age, and for those 13 through 21 years of age, if not previously vaccinated. Males 22 through 26 years of age may be vaccinated.
-
HPV vaccines are not live vaccines and can be administered to persons who are immunocompromised as a result of infection (including HIV infection), disease, or medications. Vaccine is recommended for immunocompromised persons through age 26 years who did not get any or all doses when they were younger. The immune response and vaccine efficacy might be less than that in immunocompetent persons.
-
Men who have sex with men (MSM) might especially benefit from vaccination to prevent condyloma and anal cancer. HPV4 is recommended for MSM through age 26 years who did not get any or all doses when they were younger.
-
Ideally, vaccine should be administered before potential exposure to HPV through sexual activity; however, persons who are sexually active should still be vaccinated consistent with age-based recommendations. HPV vaccine can be administered to persons with a history of genital warts, abnormal Papanicolaou test, or positive HPV DNA test.
-
A complete series for either HPV4 or HPV2 consists of 3 doses. The second dose should be administered 1–2 months after the first dose; the third dose should be administered 6 months after the first dose (at least 24 weeks after the first dose).
-
Although HPV vaccination is not specifically recommended for health-care personnel (HCP) based on their occupation, HCP should receive the HPV vaccine if they are in the recommended age group.
6. Zoster vaccination
-
A single dose of zoster vaccine is recommended for adults 60 years of age and older regardless of whether they report a prior episode of herpes zoster. Although the vaccine is licensed by the Food and Drug Administration (FDA) for use among and can be administered to persons 50 years and older, ACIP recommends that vaccination begins at 60 years of age.
-
Persons with chronic medical conditions may be vaccinated unless their condition constitutes a contraindication, such as pregnancy or severe immunodeficiency.
-
Although zoster vaccination is not specifically recommended for health-care personnel (HCP), HCP should receive the vaccine if they are in the recommended age group.
7. Measles, mumps, rubella (MMR) vaccination
-
Adults born before 1957 generally are considered immune to measles and mumps. All adults born in 1957 or later should have documentation of 1 or more doses of MMR vaccine unless they have a medical contraindication to the vaccine, laboratory evidence of immunity to each of the three diseases, or documentation of provider-diagnosed measles or mumps disease. For rubella, documentation of provider-diagnosed disease is not considered acceptable evidence of immunity.
-
A routine second dose of MMR vaccine, administered a minimum of 28 days after the first dose, is recommended for adults who
— are students in postsecondary educational institutions;
— work in a health-care facility; or
— plan to travel internationally.
-
Persons who received inactivated (killed) measles vaccine or measles vaccine of unknown type from 1963 to 1967 should be revaccinated with 2 doses of MMR vaccine.
-
A routine second dose of MMR vaccine, administered a minimum of 28 days after the first dose, is recommended for adults who
— are students in postsecondary educational institutions;
— work in a health-care facility; or
— plan to travel internationally.
-
Persons vaccinated before 1979 with either killed mumps vaccine or mumps vaccine of unknown type who are at high risk for mumps infection (e.g., persons who are working in a health-care facility) should be considered for revaccination with 2 doses of MMR vaccine.
-
For women of childbearing age, regardless of birth year, rubella immunity should be determined. If there is no evidence of immunity, women who are not pregnant should be vaccinated. Pregnant women who do not have evidence of immunity should receive MMR vaccine upon completion or termination of pregnancy and before discharge from the health-care facility.
-
For unvaccinated health-care personnel born before 1957 who lack laboratory evidence of measles, mumps, and/or rubella immunity or laboratory confirmation of disease, health-care facilities should consider routinely vaccinating personnel with 2 doses of MMR vaccine at the appropriate interval for measles and mumps or 1 dose of MMR vaccine for rubella.
8. Pneumococcal polysaccharide (PPSV) vaccination
-
Vaccinate all persons with the following indications:
— age 65 years and older without a history of PPSV vaccination;
— adults younger than 65 years with chronic lung disease (including chronic obstructive pulmonary disease, emphysema, and asthma); chronic cardiovascular diseases; diabetes mellitus; chronic liver disease (including cirrhosis); alcoholism; cochlear implants; cerebrospinal fluid leaks; immunocompromising conditions; and functional or anatomic asplenia (e.g., sickle cell disease and other hemoglobinopathies, congenital or acquired asplenia, splenic dysfunction, or splenectomy [if elective splenectomy is planned, vaccinate at least 2 weeks before surgery]);
— residents of nursing homes or long-term care facilities; and
— adults who smoke cigarettes.
-
Persons with asymptomatic or symptomatic HIV infection should be vaccinated as soon as possible after their diagnosis.
-
When cancer chemotherapy or other immunosuppressive therapy is being considered, the interval between vaccination and initiation of immunosuppressive therapy should be at least 2 weeks. Vaccination during chemotherapy or radiation therapy should be avoided.
-
Routine use of PPSV is not recommended for American Indians/Alaska Natives or other persons younger than 65 years of age unless they have underlying medical conditions that are PPSV indications. However, public health authorities may consider recommending PPSV for American Indians/Alaska Natives who are living in areas where the risk for invasive pneumococcal disease is increased.
9. Revaccination with PPSV
-
One-time revaccination 5 years after the first dose is recommended for persons 19 through 64 years of age with chronic renal failure or nephrotic syndrome; functional or anatomic asplenia (e.g., sickle cell disease or splenectomy); and for persons with immunocompromising conditions.
-
Persons who received PPSV before age 65 years for any indication should receive another dose of the vaccine at age 65 years or later if at least 5 years have passed since their previous dose.
-
No further doses are needed for persons vaccinated with PPSV at or after age 65 years.
10. Meningococcal vaccination
-
Administer 2 doses of meningococcal conjugate vaccine quadrivalent (MCV4) at least 2 months apart to adults with functional asplenia or persistent complement component deficiencies.
-
HIV-infected persons who are vaccinated should also receive 2 doses.
-
Administer a single dose of meningococcal vaccine to microbiologists routinely exposed to isolates of
Neisseria meningitidis, military recruits, and persons who travel to or live in countries in which meningococcal disease is hyperendemic or epidemic.
-
First-year college students up through age 21 years who are living in residence halls should be vaccinated if they have not received a dose on or after their 16th birthday.
-
MCV4 is preferred for adults with any of the preceding indications who are 55 years old and younger; meningococcal polysaccharide vaccine (MPSV4) is preferred for adults 56 years and older.
-
Revaccination with MCV4 every 5 years is recommended for adults previously vaccinated with MCV4 or MPSV4 who remain at increased risk for infection (e.g., adults with anatomic or functional asplenia or persistent complement component deficiencies).
11. Hepatitis A vaccination
-
Vaccinate any person seeking protection from hepatitis A virus (HAV) infection and persons with any of the following indications:
— men who have sex with men and persons who use injection drugs;
— persons working with HAV-infected primates or with HAV in a research laboratory setting;
— persons with chronic liver disease and persons who receive clotting factor concentrates;
— persons traveling to or working in countries that have high or intermediate endemicity of hepatitis A; and
— unvaccinated persons who anticipate close personal contact (e.g., household or regular babysitting) with an international adoptee during the first 60 days after arrival in the United States from a country with high or intermediate endemicity. (See footnote 1 for more information on travel recommendations). The first dose of the 2-dose hepatitis A vaccine series should be administered as soon as adoption is planned, ideally 2 or more weeks before the arrival of the adoptee.
-
Single-antigen vaccine formulations should be administered in a 2-dose schedule at either 0 and 6–12 months (Havrix), or 0 and 6–18 months (Vaqta). If the combined hepatitis A and hepatitis B vaccine (Twinrix) is used, administer 3 doses at 0, 1, and 6 months; alternatively, a 4-dose schedule may be used, administered on days 0, 7, and 21–30 followed by a booster dose at month 12.
12. Hepatitis B vaccination
-
Vaccinate persons with any of the following indications and any person seeking protection from hepatitis B virus (HBV) infection:
— sexually active persons who are not in a long-term, mutually monogamous relationship (e.g., persons with more than one sex partner during the previous 6 months); persons seeking evaluation or treatment for a sexually transmitted disease (STD); current or recent injection-drug users; and men who have sex with men;
— health-care personnel and public-safety workers who are exposed to blood or other potentially infectious body fluids;
— persons with diabetes younger than 60 years as soon as feasible after diagnosis; persons with diabetes who are 60 years or older at the discretion of the treating clinician based on increased need for assisted blood glucose monitoring in long-term care facilities, likelihood of acquiring hepatitis B infection, its complications or chronic sequelae, and likelihood of immune response to vaccination;
— persons with end-stage renal disease, including patients receiving hemodialysis; persons with HIV infection; and persons with chronic liver disease;
— household contacts and sex partners of persons with chronic HBV infection; clients and staff members of institutions for persons with developmental disabilities; and international travelers to countries with high or intermediate prevalence of chronic HBV infection; and
— all adults in the following settings: STD treatment facilities; HIV testing and treatment facilities; facilities providing drug-abuse treatment and prevention services; health-care settings targeting services to injection-drug users or men who have sex with men; correctional facilities; end-stage renal disease programs and facilities for chronic hemodialysis patients; and institutions and nonresidential daycare facilities for persons with developmental disabilities.
-
Administer missing doses to complete a 3-dose series of hepatitis B vaccine to those persons not vaccinated or not completely vaccinated. The second dose should be administered 1 month after the first dose; the third dose should be given at least 2 months after the second dose (and at least 4 months after the first dose). If the combined hepatitis A and hepatitis B vaccine (Twinrix) is used, give 3 doses at 0, 1, and 6 months; alternatively, a 4-dose Twinrix schedule, administered on days 0, 7, and 21–30 followed by a booster dose at month 12 may be used.
-
Adult patients receiving hemodialysis or with other immunocompromising conditions should receive 1 dose of 40
µg/mL (Recombivax HB) administered on a 3-dose schedule or 2 doses of 20
µg/mL (Engerix-B) administered simultaneously on a 4-dose schedule at 0, 1, 2, and 6 months.
13. Selected conditions for which Haemophilus influenzae type b (Hib) vaccine may be used
-
1 dose of Hib vaccine should be considered for persons who have sickle cell disease, leukemia, or HIV infection, or who have anatomic or functional asplenia if they have not previously received Hib vaccine.
14. Immunocompromising conditions
-
Inactivated vaccines generally are acceptable (e.g., pneumococcal, meningococcal, and influenza [inactivated influenza vaccine]), and live vaccines generally are avoided in persons with immune deficiencies or immunocompromising conditions. Information on specific conditions is available at
http://www.cdc.gov/vaccines/pubs/acip-list.htm.
These schedules indicate the recommended age groups and medical indications for which administration of currently licensed vaccines is commonly indicated for adults ages 19 years and older, as of January 1, 2012. For all vaccines being recommended on the adult immunization schedule: a vaccine series does not need to be restarted, regardless of the time that has elapsed between doses. Licensed combination vaccines may be used whenever any components of the combination are indicated and when the vaccine's other components are not contraindicated. For detailed recommendations on all vaccines, including those used primarily for travelers or that are issued during the year, consult the manufacturers' package inserts and the complete statements from the Advisory Committee on Immunization Practices (http:// www.cdc.gov/vaccines/pubs/acip-list.htm).
Report all clinically significant postvaccination reactions to the Vaccine Adverse Event Reporting System (VAERS). Reporting forms and instructions on filing a VAERS report are available at http://www.vaers.hhs.gov or by telephone, 800-822-7967.
Information on how to file a Vaccine Injury Compensation Program claim is available at http://www.hrsa.gov/vaccinecompensation or by telephone, 800-338-2382. Information about filing a claim for vaccine injury is available through the U.S. Court of Federal Claims, 717 Madison Place, N.W., Washington, D.C. 20005; telephone, 202-357-6400.
Additional information about the vaccines in this schedule, extent of available data, and contraindications for vaccination also is available at http://www.cdc.gov/vaccines or from the CDC-INFO Contact Center at 800-CDC-INFO (800-232-4636) in English and Spanish, 8:00 a.m. to 8:00 p.m., Monday through Friday, excluding holidays.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services.
|
Vaccine
|
Contraindications
|
Precautions
|
|
Influenza, injectable trivalent (TIV)
|
Severe allergic reaction (e.g., anaphylaxis) after previous dose of any influenza vaccine or to a vaccine component, including egg protein.
|
Moderate or severe acute illness with or without fever.
History of Guillain-Barré syndrome (GBS) within 6 weeks of previous influenza vaccination.
|
|
Influenza, live attenuated (LAIV)2
|
Severe allergic reaction (e.g., anaphylaxis) after previous dose of any influenza vaccine or to a vaccine component, including egg protein.
Immune suppression.
Certain chronic medical conditions such as asthma, diabetes, heart or kidney disease.3
Pregnancy.
|
Moderate or severe acute illness with or without fever.
History of GBS within 6 weeks of previous influenza vaccination.
Receipt of specific antivirals (i.e., amantadine, rimantadine, zanamivir, or oseltamivir) 48 hours before vaccination. Avoid use of these antiviral drugs for 14 days after vaccination.
|
|
Tetanus, diphtheria, pertussis (Tdap);
tetanus, diphtheria (Td)
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
For Tdap only: Encephalopathy (e.g., coma, decreased level of consciousness, or prolonged seizures) not attributable to another identifiable cause within 7 days of administration of a previous dose of Tdap or diphtheria and tetanus toxoids and pertussis (DTP) or diphtheria and tetanus toxoids and acellular pertussis (DTaP) vaccine.
|
Moderate or severe acute illness with or without fever.
GBS within 6 weeks after a previous dose of tetanus toxoid–containing vaccine.
History of arthus-type hypersensitivity reactions after a previous dose of tetanus or diptheria toxoid–containing vaccine; defer vaccination until at least 10 years have elapsed since the last tetanus toxoid–containing vaccine.
For Tdap only: Progressive or unstable neurologic disorder, uncontrolled seizures, or progressive encephalopathy until a treatment regimen has been established and the condition has stabilized.
|
|
Varicella,2
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
Known severe immunodeficiency (e.g., from hematologic and solid tumors, receipt of chemotherapy, congenital immunodeficiency, or long-term immunosuppressive therapy4 or patients with human immunodeficiency virus (HIV) infection who are severely immunocompromised).
Pregnancy.
|
Recent (≤11 months) receipt of antibody-containing blood product (specific interval depends on product).5
Moderate or severe acute illness with or without fever.
Receipt of specific antivirals (i.e., acyclovir, famciclovir, or valacyclovir) 24 hours before vaccination; if possible, delay resumption of these antiviral drugs for 14 days after vaccination.
|
|
Human papillomavirus (HPV)
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
|
Moderate or severe acute illness with or without fever.
Pregnancy.
|
|
Zoster
|
Severe allergic reaction (e.g., anaphylaxis) to a vaccine component.
Known severe immunodeficiency (e.g., from hematologic and solid tumors, receipt of chemotherapy, or long-term immunosuppressive therapy4 or patients with HIV infection who are severely immunocompromised).
Pregnancy.
|
Moderate or severe acute illness with or without fever.
Receipt of specific antivirals (i.e., acyclovir, famciclovir, or valacyclovir) 24 hours before vaccination; if possible, avoid use of these antiviral drugs for 14 days after vaccination.
|
|
Vaccine
|
Contraindications
|
Precautions
|
|
Measles, mumps, rubella (MMR)2
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
Known severe immunodeficiency (e.g., from hematologic and solid tumors, receipt of chemotherapy, congenital immunodeficiency, or long-term immunosuppressive therapy4 or patients with HIV infection who are severely immunocompromised).
Pregnancy.
|
Moderate or severe acute illness with or without fever.
Recent (within 11 months) receipt of antibody-containing blood product (specific interval depends on product).6
History of thrombocytopenia or thrombocytopenic purpura.
Need for tuberculin skin testing.7
|
|
Pneumococcal polysaccharide (PPSV)
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
|
Moderate or severe acute illness with or without fever.
|
|
Meningococcal, conjugate, (MCV4);
meningococcal, polysaccharide (MPSV4)
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
|
Moderate or severe acute illness with or without fever.
|
|
Hepatitis A (HepA)
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
|
Moderate or severe acute illness with or without fever.
Pregnancy.
|
|
Hepatitis B (HepB)
|
Severe allergic reaction (e.g., anaphylaxis) after a previous dose or to a vaccine component.
|
Moderate or severe acute illness with or without fever.
|
|
|
More information on vaccine components, contraindications, and precautions also is available from specific vaccine package inserts and ACIP recommendations for specific vaccines, and is summarized in Atkinson W, Wolfe S, Hamborsky J, eds. Epidemiology and prevention of vaccine preventable diseases. 12th ed. Washington, DC: Public Health Foundation, 2011. Available at http://www.cdc.gov/vaccines/pubs/pinkbook/default.htm.