Highlights
- The Nebraska Department of Health and Human Services (NDHHS) sought to improve its understanding of substance use and overdose deaths in its communities.
- Syndromic data proved useful in characterizing populations at risk, guiding prevention efforts, and informing public health assessments of the burden of opioid misuse in communities.
- Syndromic data were also useful in tracking emerging trends in drugs (or drug types) being used and identifying where overdoses occur.

Public health problem
Opioid misuse is an urgent public health concern in the United States. Although most of the nation is focusing on the opioid epidemic, other substances remain as serious threats in Nebraska. Per the 2014 Treatment Episode Data Set report, most primary drug treatment admissions in Nebraska are related to methamphetamines and amphetamines, followed by marijuana and then opioids.1 Moreover, Nebraska's 2011–2015 death certificate data indicate that methamphetamines and amphetamines are leading causes of overdose (OD) deaths, along with opioids and benzodiazepines. Through public health surveillance, the Nebraska Department of Health and Human Services (NDHHS) sought to improve its understanding of how substance use and overdose deaths were affecting its communities.
Actions taken
NDHHS's Division of Public Health (DPH) Syndromic Surveillance Program used CDC's National Syndromic Surveillance Program (NSSP) Community of Practice resources to collaborate with the NDHHS DPH Drug Overdose Prevention (DOP) Program on two pilot projects to characterize substance use and OD deaths as follows:
- Develop and validate a Chief Complaint and Discharge Diagnosis syndromic surveillance definition for monitoring opioid OD-related emergency department (ED) visits across multiple public health jurisdictions. (Collaboration with NDHHS's DOP Program, Division of Behavioral Health [DBH], and Tri-County, Colorado Health Department.)
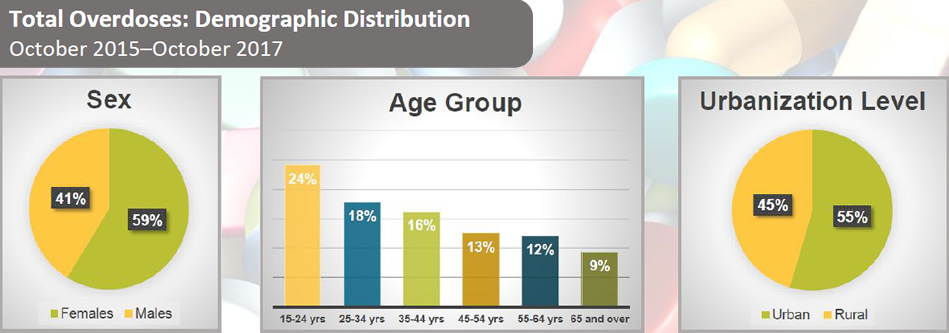
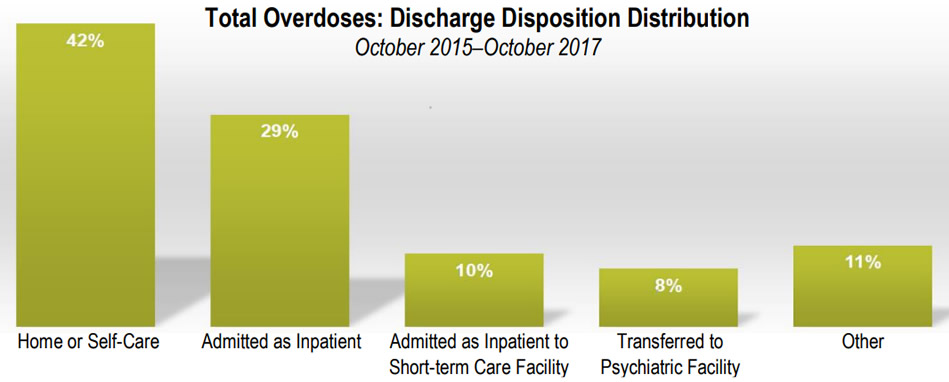
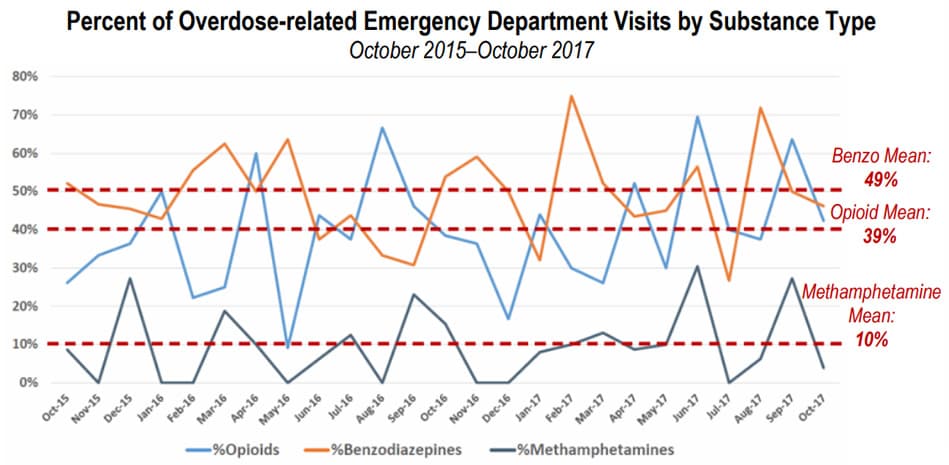
- Evaluate the utility of syndromic surveillance ED data for monitoring all-substance ODs. NDHHS developed syndromic surveillance definitions for OD-related ED visits resulting from opioids, benzodiazepines, methamphetamines, cannabis, cocaine, psychodysleptics, barbiturates, opioids+benzodiazepines, and opioids+methamphetamines. NDHHS also developed definitions for expanded surveillance of total ODs and poisonings. Definitions followed the Council of State and Territorial Epidemiologists (CSTE) Substance Abuse and Mental Health Workgroup/Alcohol and Other Drugs Subcommittee's recommended indicators. Distribution of total substance OD-related ED visits was stratified by sex, age group, and discharge disposition. (Collaboration with NDHHS DOP Program and NDHHS DBH.)
Outcome
Both projects demonstrate how syndromic surveillance can enhance substance OD prevention programs by characterizing populations at risk and guiding prevention efforts. Syndromic data are one more indicator that can be used to inform public health assessments of the burden of opioid misuse in communities. The project findings also show these data can be used in near real-time to track emerging trends in drugs (or drug types) being used and identify where ODs occur.
Collaboration with internal and external partners was key
NDHHS described its work with Tri-County, Colorado Health Department in July 2017 at the International Society for Disease Surveillance (ISDS) Opioid Webinar Series and at the 2018 ISDS Conference. NDHHS also presented an abstract about the collaboration between its DOP Program and DBH at the 2018 CSTE Conference. The syndromic surveillance Discharge Diagnosis definitions developed through collaborative efforts are now being used routinely, and both collaborative internal partnerships and projects will continue throughout 2019.
Lessons learned
These projects show that syndromic surveillance data can provide supplemental information to:
- Enhance substance OD prevention programs to inform timely assessments of burden, define populations at risk, and guide prevention efforts.
- Track emerging trends in drugs (or drug types) being used and where ODs occur—all in near real-time. Findings could be used to direct naloxone and treatment resources and to inform local public health departments and prevention coalitions that provide education and prevention activities.
The project's success is largely due to collaboration, high percentage of data completeness, and access to resources provided by the CDC NSSP and its Community of Practice, especially participation from the Overdose Surveillance Committee.
Resources
Sandra Gonzalez, Epidemiology SyS Coordinator
Division of Public Health
Nebraska Department of Health and Human Services
sandra.gonzalez@nebraska.gov
Centers for Disease Control and Prevention
Office of Public Health Data, Surveillance, and Technology
Detect and Monitor Division
www.cdc.gov/nssp
The findings and outcomes described in this syndromic success story are those of the authors and do not necessarily represent the official position of the National Syndromic Surveillance Program or the Centers for Disease Control and Prevention.
- Substance Abuse and Mental Health Services Administration (SAMHSA), Center for Behavioral Health Statistics and Quality. Treatment Episode Data Set (TEDS): 2004–2014. State Admissions to Substance Abuse Treatment Services. BHSIS Series S-85, HHS Publication No. (SMA) 16-4987. Rockville (MD): SAMHSA; 2016.