
Maintenance Supervisor Dies After Being Pinned Between Dump Body and Truck Frame During Troubleshooting Inspection West Virginia
Case : 00WV011-01
Release Date: September 8, 2000
SUMMARY
On May 24, 2000, a 37-year-old male asphalt and concrete plant maintenance supervisor (the victim) died of injuries sustained when he was pinned between the dump body and frame of a truck. Just prior to the incident, the victim and a coworker had decided to fix the truck’s faulty brake lights. The coworker raised the bed for better access and turned the engine off. He told the victim he was going into the shop for wooden blocks to crib the elevated dump bed. Before the coworker could return with the cribbing, the victim crawled over the left rear wheels placing himself between the elevated bed and the truck frame. Although there were no witnesses, it is believed that the victim may have mistaken the dump bed’s pull-off cable for a wire or inadvertently contacted it, causing the bed to suddenly lower. The coworker heard the victim moan and ran outside. Upon spotting the victim he yelled for help. He jumped into the truck, started the engine and raised the dump bed. Another worker notified the secretary, who had a coworker call 911 while she ran to the victim’s aid. The secretary was a certified first aid instructor. She instructed those assisting her in extrication and then assessed the victim. She started CPR and continued until EMS arrived minutes later. The victim was transported to the local hospital where he was pronounced dead. The coroner estimated the time from injury to death to be minutes.
The WV FACE Investigator concluded that to reduce the likelihood of similar occurrences, employers should:
- ensure that before making inspections, adjustments, or repairs strong, heavy, positive supports are used to secure the dump body and prevent it from lowering.
- develop, implement, and enforce a written safety program which includes, but is not limited to, task-specific safety procedures and worker training in hazard identification, avoidance, and control.
- ensure that replacement pull-off cables are identical to the original equipment and installed as per the manufacturer.
INTRODUCTION
On March 24, 2000, a 37-year-old male maintenance supervisor (the victim) died of injuries sustained when he was pinned between the dump bed and frame of his truck. On May 12, 2000, the West Virginia FACE Investigator was notified of the death by the West Virginia Department of Health and Human Resources via a death certificate. The WV FACE field investigator contacted the responding law enforcement agency. The case was discussed with the investigating officer and a copy of the police report was obtained. The WV FACE field investigator traveled to the site on August 2, 2000 and met with a representative of the company who employed the victim. This meeting consisted of a discussion of the incident and a review of the company’s safety program. The dump truck’s history, including similar maintenance situations requiring elevated dump beds, was also discussed. The representative then accompanied the investigator to the incident site. The piece of equipment was examined and observed while operating. Photographs were also taken at the site. The medical examiner’s report was also obtained.
The employer in this incident was an asphalt paving company that had been in business for eleven months and employed seven. Five of the employees were present the day of the incident.
There was no formal company written safety program or company, site, and task-specific safety training. The employer did indicate that weekly safety meetings were held and that the victim was given the task of conducting these meetings. The employer also indicated that the company’s insurance carrier’s safety handbook was used as a guide for these weekly meetings. Additionally, it was reported that elevated dump beds were normally cribbed . The employer had not previously been cited by OSHA.
The victim’s job at the time of the incident was head mechanic as well as paving crew member. The victim had been working for the employer less than a year when the incident occurred.
INVESTIGATION
At approximately 7:30 a.m., on March 24, 2000 the victim began his shift at the paving facility. At approximately 12:30 p.m., the victim and a coworker had decided to fix the truck’s faulty brake lights. The company was the second owner of the truck. The company did not have an owner’s manual for the truck. The coworker raised the bed for better access and turned the engine off. The truck was not originally equipped with a permanently attached body prop, therefore he told the victim he was going into the shop for wooden blocks to crib the elevated dump bed (see Figure 1). It was reported by the company representative that cribbing the bed was usually done. Before the coworker could return with the cribbing, the victim crawled over the left rear wheel placing himself between the elevated bed and the truck frame (see Figure 2). Although there were no witnesses, it is believed that during that period, the victim may have mistaken the dump bed’s pull-off cable for a wire. Dump body systems are equipped with a pull-off cable. A pull-off cable is a section of wire rope which runs along the truck’s frame from the hydraulic valve (which controls fluid flow to the elevating mechanism) to the rear portion of the dump bed. Pull-off cables are designed to override the lever control in the cab and shut off the fluid delivery to the hoist cylinder during raising operations thereby limiting the angle of the raised bed to approximately 45 degrees from the horizontal (see Figure 3). When these cables are pulled past a certain point, they will also allow the hoisting cylinder to drain completely, abruptly lowering the bed. The coworker heard the victim moan and ran outside. Upon spotting the victim he yelled for help. He jumped into the truck, started the engine and raised the dump bed. Another worker notified the secretary, who had a coworker call 911 while she ran to the victim’s aid. The secretary was a certified first aid instructor. She instructed those assisting her in extrication and then assessed the victim. She started CPR and continued until EMS arrived minutes later. The victim was transported to the local hospital where he was pronounced dead. The coroner estimated the time from injury to death to be minutes.
CAUSE OF DEATH
The medical examiner’s report listed the immediate cause of death as compression asphyxiation.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that before making inspections, adjustments, or repairs, strong, heavy, positive supports are used to hold the dump body from inadvertently lowering.
Discussion: In this incident, the victim was working on a truck whose dump bed was elevated and then placed himself under the elevated dump bed without protection. OSHA Regulation 29 CFR 1926.600(a)(3)(i) requires that dump bodies and similar equipment shall be fully lowered or blocked when being repaired or when not in use.1 Additionally, OSHA Regulation 29 CFR 1926.601(b)(10) requires that trucks with dump bodies shall be equipped with positive means of support, permanently attached to the truck.1 (see Figure 4). Correctly chocking or blocking the raised bed would have prevented this incident by supporting and/or arresting the energy source before contacting the victim. Having had a convenient permanently attached body prop would not only have eliminated the need for his coworker to obtain cribbing, but would have eliminated the time period the victim placed himself under the elevated dump bed while he waited.
Recommendation #2: Employers should develop, implement, and enforce a written safety program which includes, but is not limited to, task-specific safety procedures and worker training in hazard identification, avoidance, and control.
Discussion: The evaluation of tasks to be performed at the work site forms the basis for the development, implementation, and enforcement of a safety program as well as task-specific safety procedures. The key elements of the program should include the communication of task-specific safe work practices and, at a minimum, training in hazard identification and the avoidance and abatement of these hazards. In this incident, the victim was fatally injured when he accessed a piece of equipment using an unsafe method to accomplish a task (not utilizing engineering controls and safe work practices). Training in the hazards associated with the work environment, and in particular, those hazards associated with working around both functioning and malfunctioning dump body systems and task-specific safety procedures for working on both functioning and malfunctioning dump body systems via a comprehensive safety program, would have given the victim the knowledge necessary to recognize and avoid a hazardous situation. For example, detailed explanations on the how and why dump bodies will suddenly lower and the precautions necessary to avoid this hazard should be part of the company training program.
Recommendation #3: Employers should ensure that replacement pull-off cables are identical to the original equipment and installed as per the manufacturer.
Discussion: The truck bed’s pull-off cable was not original. It had been replaced with a piece of transparent green plastic coated wire rope clothes line by the previous owner. It appeared to be stretched and was not enclosed in a metal tube as it was originally, but exposed and hanging (see Figure 5). It is believed that the victim may have mistaken this plastic coated cable for a wire associated with the brake lights. The original pull-off cable would have been non coated and would not have appeared electrical in nature. Additionally, most of its length would have been enclosed in tubing. Having ensured the cable’s original configuration may have eliminated the possible mistaken identity, thereby eliminating the victim handling the cable.
REFERENCES:
- Office of the Federal Register: Code of Federal Regulations, Labor, 29 CFR Part 1926, U.S. Department of Labor, Occupational Safety and Health Administration, Washington, D.C., April 25, 1975.
ILLUSTRATIONS

Figure 1. The arrow points to the method of blocking which would have been used had the victim waited.
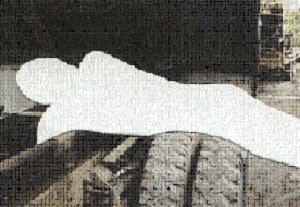
Figure 2. The figure represents the victim’s position prior to the bed lowering.

Figure 3. The arrow points to a properly installed and enclosed pull-off cable.

Figure 4. The arrow points to the convenient and permanently attached body support installed after the incident as per OSHA’s recommendations.
The support folds when not in use.
Figure 5. This photo shows the center section of the stretched and unprotected cable.
FATALITY ASSESSMENT AND CONTROL EVALUATION PROGRAM
The WVU Center for Rural Emergency Medicine, through a contract with the West Virginia Department of Health and Human Resources, conducts investigations on the causes of work-related fatalities within the state. The goal of this program is to prevent future fatal work-place injuries. West Virginia FACE intends to achieve this goal by identifying and studying the risk factors that contribute to work-place fatalities, by recommending intervention strategies, and by disseminating prevention information to employers, employees, trade associations, unions, equipment manufacturers, students, teachers, and others with an interest in work-place safety.
Please use information listed on the Contact Sheet on the NIOSH FACE website to contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.