
Maintenance Worker Electrocuted While Attempting to Change a Light Bulb in Washington State
Washington Case Report 04WA080
Release Date: July 31, 2008
Summary
In October of 2004, a 32-year-old male maintenance worker died from electrocution while working at an assisted living facility in Washington State. The victim was changing a broken metal halide bulb in a ceiling fixture. To remove it, the victim turned off the area wall light switch and taped the switch in the “off” position. The victim climbed into the attic space and detached the fixture “light can” to remove the broken bulb.
While holding on to the fixture in one hand, he touched the bulb base with a non-insulated tool and was electrocuted. The fixture was still hot (energized). It was part of a building emergency lighting system on a separate circuit. The wiring was not shown in the “as-built” plans he was using and it was not connected to the breaker.
Between 1:00 PM to 1:30 PM, co-workers noticed the victim was missing and conducted a search. They were unable to find him and called 911. The local fire department, rescue team eventually found the victim — deceased in the second floor ceiling location of the building. The employee was not trained or authorized to do electrical work; neither was he experienced in changing metal halide bulbs which often are difficult to remove.
To prevent similar occurrences in the future, the Washington State Fatality Assessment & Control Evaluation (FACE) investigative team advises facilities maintenance employers to follow these guidelines:
- Only qualified electricians should work on electrical systems.
- Proper Lockout-Tagout procedures should be used when work is done on any system that may contain electrical energy.
- Electrical systems and components must be tested to ensure they are de-energized before performing work. Turning off a light switch or circuit breaker may not de-energize an electrical system or its components. If you can’t test, let it rest.
- Tools for de-energizing circuits should not be supplied to untrained personnel. Make sure appropriate testing devices and insulated tools are used and verify that personnel are knowledgeable and trained in their safe operation. In most cases it is recommended that a licensed electrician perform the testing.
- Don’t rely on “as built” electrical drawings to determine current electrical system design and operation. Systems must be verified in place by testing and tracing the actual configuration.
- The facility accident prevention guidelines for these types of lighting systems should describe this electrocution hazard for maintenance personnel.
- Electrical breakers should be clearly labeled to indicate their action, location, and purpose.
Introduction
In October of 2004, the Washington State FACE Program ( WA FACE) was notified by WISHA, the Washington Industrial Safety and Health Administration (which is now known as the Division of Occupational Safety & Health, DOSH), of the death of a 32-year-old facility maintenance worker.
The Washington FACE Field Investigator met with the regional WISHA representative investigating the case.
The WISHA representative helped define the incident site location and reviewed the details of the work site, including personnel relationships and equipment usage.
After reviewing the case with the WISHA representative, the Washington FACE Field Investigator made several attempts to reach representatives of the assisted living facility.
When contact was finally made with the administrator of the assisted living facility, the administrator requested that all communication regarding the electrocution be directed to an attorney representing the facility’s parent organization.
After explaining the primary objectives of the FACE program, the WA FACE Investigator agreed to meet the organization’s attorney at his office. The attorney informed WA FACE that they had hired a Washington State forensics engineering firm to study and review elements of the incident. He invited us to contact them to review their findings. The attorney notified the engineering firm and asked that their records and investigation materials be made available to the FACE team.
Within a couple of days, the WA FACE Field Investigator and the Principle Investigator visited the forensics engineering firm to discuss their findings and their perspective regarding the fatality.
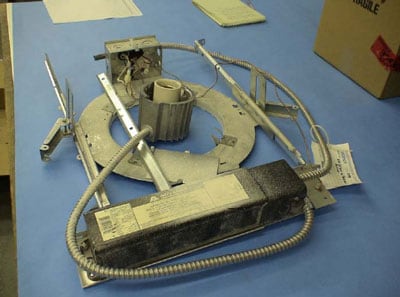
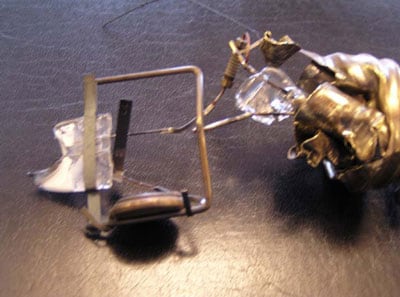
The forensics engineering firm had copies of the electrical drawings; they had the actual metal halide light fixture that had been removed from the facility; they also had the metal halide bulb, and a sample replacement bulb used at the facility.
The WA FACE team reviewed all available items, taking into consideration the forensics engineering firm’s analysis and evaluation of the fatal incident.
The engineer who had conducted the forensics evaluation had left the company, so the FACE team reviewed the findings with one of the senior partners of the firm who explained the primary electrical components in the case.
The engineering firm provided insights into the hazards associated with the metal halide bulbs and the emergency lighting electrical system within the assisted living facility.
The WA FACE team made several requests via the assisted living organization’s attorney to visit the incident site, but were denied. The attorney himself enthusiastically supported the Washington State and the NIOSH FACE process and mission.
The attorney appreciated that the FACE program can be instrumental in preventing similar incidents in the future. The parent organization, however, was not comfortable with FACE doing an onsite evaluation.
We informed the attorney that our site visits help ensure a thorough and fair FACE evaluation by providing details otherwise unavailable. We reassured him of our sensitivity to their concerns and our recognition of the trauma of these events. FACE conducts its fatality reviews with great care and understanding, we pointed out.
The WA FACE team agreed to abide by any parameters and recommendations by the parent company when conducting their site visit evaluation, yet a third request was denied. The FACE team decided to proceed with the best resources and information that was available to provide a meaningful investigation report.
The incident being reviewed by FACE took place at an assisted living facility located in southern Washington State. This facility is a sub-unit of a much larger organization with several facilities located in the Northwest region. Each site is set up as an individual LLC (limited Liability Company).
The parent company is headquartered out of state and employs over 1,000 people. The company manages over 2,300 apartments and housing units in multiple states.
The organization’s staff positions include site administrators, activity directors, housekeepers, nurses, caregivers, cooks, dietary aides, licensed practical nurses (LPN/RCCs), and maintenance personnel.
The company started in 1979 as a construction company and then transitioned through real-estate sales and development, before evolving into its current senior living operations business in 1995.
The facility where the incident occurred was opened in 2001 and employed 38 people at the time of the incident, including the victim.
The facility administrator has many duties including safety of the site. The facility maintenance employee (the victim) reported to the facility administrator.
The organization had written safety processes in place, but the FACE team was not able to evaluate the scope and effectiveness of their safety program. The facility had a written process for handling general electrical issues and also had a Lockout-Tagout process in place.
It is not clear how well these safety guidelines were understood by the facility administrator or the victim. Our investigation indicates that the victim had some knowledge of proper safety procedures when working with the facility’s lighting system; however, there were elements of the process that were either missed or not clearly defined or understood by the victim.
The facility had a safety committee, but the FACE investigation team was not able get any details of its processes.
It is also not clear how much experience the victim had in performing facility electrical work. As the maintenance person, it appears the victim was more of a generalist, having the skills to perform a wide variety of maintenance work for the facility, but for more complex maintenance issues would be expected to request external help, such as a contractor.
For most organizations, hiring a contractor needs the approval of the site facility administrator and sometimes the parent organization, depending on the cost of the work required. This might make a maintenance worker reluctant to ask for outside help.
Changing a light bulb should be an easy task for any maintenance person, but there are hidden hazards when dealing with electrical system maintenance and repair. Electrical system work should only be done by a qualified or certified person.
The victim had worked for this employer for approximately five months prior to the fatal incident. Previously, the victim worked as a maintenance supervisor for an auto dealership. He had also previously worked as an auto mechanic.
On a Tuesday morning in October of 2004, the victim was electrocuted when he made contact with an exposed energized metal halide light conductor and a grounded item.
Back to Top
Investigation
The assisted living facility’s maintenance person (the victim) worked from 7:30 AM to 3:30 PM Monday through Friday. The victim was also on call to deal with emergency maintenance issues, but according to the facility administrator call-ins were very rare.
On a typical Monday morning (the day prior to the fatal incident), the victim’s many duties for the day included the apparently simple task of replacing a burned-out bulb at the facility.
In reviewing the “chain-of-events” descriptions by the victim’s co-workers, it appears that the victim took a very methodical and a very conscientious approach to what seemed a basic maintenance task.
It is unclear what conversations the victim may have had or whether he had reviewed the electrical problem with the facility administrator. Our investigation revealed the victim talked to a co-worker regarding the broken bulb, and had a plan to fix it. (Neither the co-worker nor the facility administrator was familiar with general maintenance procedures, nor were they familiar with electrical safety practices.)
The victim had many general maintenance skills, but though comfortable with basic electrical work, he had no specific training in electrical repairs. The victim was the only facility maintenance person for that site, and reported to the assisted living facility administrator.
The job description indicated that “The Plant Operations Director (the victim) is responsible for the total maintenance and repair of the facility including both the building plumbing, masonry, carpentry, painting, electrical, refrigeration, air conditioning, flooring and grounds.”
A facility representative confirmed that no technical skill inquiries were made in evaluating the victim for the position. The facility had primarily asked hiring questions about the victim’s work ethic, dependability and flexibility for the job, but not about his skill level.
The facility indicated that they wanted someone who knew basic maintenance work, was dependable, and responsive to needs beyond normal working hours. No training documents were found defining what training the victim had.
Based on his assigned duties, the facility determined the victim did not need specialized training, according to their representative. The facility said they would hire contractors to perform work that went beyond normal maintenance duties.
On the Monday evening before the incident it appears that the victim had checked the problem and noted that it was not a simple fix. The fixture was located in an open area of the facility. The victim assessed the situation and formulated a plan to fix the bulb which was located in a recessed “light can” fixture approximately 16 feet in the ceiling above floor level.
The FACE investigation was unable to determine if the metal halide bulb had broken before or during an attempted bulb replacement on that Monday.
Metal halide bulbs can get extremely hot and sometimes fail as the constant heat takes a toll on the glass of the inner and outer cone, causing them to deteriorate and possibly break.
The victim recognized this was not a routine job, he noticed that bulb conductor was exposed and had to be de-energized. He also recognized that the base was broken high up in the recessed fixture, and thus it was not possible to remove the base of the bulb easily by using a ladder in the interior sitting area room side of the light fixture.
The next step the victim took was to search out the electrical power source for that light fixture. He also performed other tasks during the day while working on this problem.
The victim briefly talked with the assistant facility administrator about the difficulty he was having finding the breaker to shut the power to the light fixture. We believe they considered using walkie talkies so that one person could be in the facility sitting room while the victim “flipped” the breakers until they found the one that shut off the lights for the sitting area. This idea was not followed up on.
The victim found “as-built” drawings for the facility’s electrical systems and took them home to study that evening.
The next morning (Tuesday) the victim (based on the co-worker’s interviews and incident investigation findings) put fixing the bulb high on his agenda. He went to the sitting room area where the broken light was located, turned off the light switch for that location, and then placed tape over the switch. (See Photo 2)
Using the “as-built” electrical drawings the victim located the breaker panel for the lights in the sitting room. He then switched the breaker into the “off” position. We believe that he checked that the lights in the sitting area were off and then opened the overhead access panel in the ceiling to find the light fixture with the broken metal halide bulb.
The victim crawled in the ceiling overhead area and over to the light fixture. He removed “light can,” which housed the broken metal halide bulb. He next pulled out a multi-tool from his pocket and attempted to unscrew the broken end of the bulb from the light socket.
As the victim grabbed the exposed conductor of the broken metal halide bulb with the non-insulated multi-tool, he simultaneously held onto to the grounded metal light fixture housing. At that instant the victim was electrocuted. The circuit providing power to the light fixture was still on.
The light had not been turned off by the wall switch located in the sitting room, nor was it turned off at the breaker box located at the facility operations mechanical / electrical room.
When the victim simultaneously touched the exposed metal halide bulb conductor and the grounded metal light fixture, he completed a path to ground and was electrocuted when he became part of the electrical circuit. The victim was electrocuted by 120 volts at 15amps which traveled through a ballast (step-up transformer) that increased the voltage to 300 volts. This overhead light was part of an emergency light system for the area.
The victim was seen at the assisted living facility at around 7:30 AM on Tuesday morning. At around 9:00 AM it was reported that the victim was in the attic changing a light bulb.
Sometime after the morning meeting several of the facility staff went to see how the victim was doing. They tried to call him on the radio he carries, but got no answer. The staff indicated that the victim always responded very quickly when contacted by radio.
They next tried his cell phone; again, there was no answer. During their search they found a ladder and a cold cup of coffee on a second floor wing of the facility. One of the staff climbed up the ladder — which was under the open access panel leading to the attic area — and called for the victim: again, there was no answer. The staff member looked into the dark attic but could not see the victim.
Concern mounted, and facility staff started checking the rest of the grounds. They knew he would not leave the premises without telling someone. They checked his time clock to see if he had checked out — he had not.
They noticed his car was still in the facility parking lot. They checked for him in the locked maintenance rooms where the electrical breakers were located. They looked for him in empty assisted living apartments. They looked in storage locations; they looked all over, while continually calling his radio and cell phone. Finally, they called 911 sometime between 1:00 and 1:15 that afternoon.
The local fire department soon arrived at the assisted living facility. After a brief search, they found the victim in the attic, lying on the emergency light fixture. They were not able to resuscitate him; he appeared to have been dead for some time. The fire department called the police and the medical examiner’s office to investigate the incident.
The assisted living facility hired an electrical contractor to help resolve the electrical hazard created by the broken metal halide bulb.
The parent organization hired a forensics engineering firm to investigate the incident. The senior forensics engineer worked with the electrical contractor to help trace the events of that fateful Tuesday.
Their review determined that a breaker designated as breaker #12 had been turned off at the breaker box. The “as-built” drawings show that the light fixture in the incident was connected to breaker #12, but it was not.
The emergency lighting system (including the light involved in the incident) was tied into another breaker located elsewhere in the facility. There were no locks or tags applied to the circuit breaker and no tag applied to the light switch that the victim had turned off and taped in the common sitting room.
The investigation noted that labels were applied to the circuit breakers before the facility opened but many had since changed. It was also noted that some breakers marked as blanks actually had active breakers installed in those spots. None of the breakers found at the facility were identified as an emergency lighting circuit except for a backup generator system. The specific circuit that the victim worked on was not identified within any of the breakers at the facility.
All of the breakers have been traced, tagged, and relabeled by a qualified electrical contractor since the incident. The assisted living facility has also stopped the purchase and storage of metal halide bulbs. The facility will only have an electrician / electrical contractor change or replace these bulbs. Their maintenance personnel will not handle halide bulbs at any of the organization’s assisted living facilities in the northwest.
Cause of Death
The medical examiner determined that the cause of death was due to electrocution after contact with a low voltage electrical source.
Recommendations/Discussion
Recommendation #1: Only qualified electricians should work on electrical systems.
Discussion: This fatal injury (electrocution) occurred when the victim came in contact with a live electrical circuit while trying to replace a burned-out, broken metal halide bulb.
Electrical systems are so commonplace we sometimes become complacent when working in or around them. It takes very little electrical current to result in a fatality; for example, the current drawn from a 7 ½ watt, 120 volt lamp is enough to cause death.
According to the Electrical Safety Foundation International (ESFI), more than 46,000 workers have suffered some type of electrical injury within the past decade and nearly 300 workers in the U.S. die every year from exposure to electrical hazards.
Many maintenance generalists may not have the electrical background, proper experience, or proper tools to work on electrical systems correctly. Many learn some of their skills from coworkers who may not be “qualified” to work on electrical systems.
It is the employer’s responsibility to ensure that workers who work with or around electrical systems are qualified and able to recognize and work safely with electrical hazards.
Maintenance personnel face serious risk of electrical exposure within their normal job routine but are most likely not qualified per WISHA and OSHA standards to make repairs or work with live (hot) electrical components within their operations. As in this case, trying to do an electrical assessment with in-house staff can be a recipe for disaster.
Hiring qualified electrical specialists / electrical contractors to work with the maintenance person on the assisted living facility’s electrical system would have reduced or even eliminated the inherent risks.
The National Safety Council estimates that anywhere from 600 to 1,000 people (this includes both occupational and non-occupational incidents) die every year from electrocution.
The NSC further states that nearly half of those who die from electrocution are from voltages that are less than 600 volts, and that they were working on exposed energized circuits at the time when the fatal injury occurred.
Electrocutions generally rank around the fourth or fifth leading cause of occupational fatalities in the U.S. (depending on the period of time measured) and averages approximately 7th in Washington State.
Recommendation #2: Proper Lockout-Tagout procedures should be used when work is done on any system that may contain electrical energy.
Discussion: Anyone who installs, operates, or maintains electrical equipment or components should be aware of the hazards involved. The electrical system they plan to work on needs to be Locked-Out and de-energized before any work begins. If there is any doubt, stop!
Lockout-Tagout (LOTO) or lock and tag is used to ensure that machines and circuits are properly shut off and not turned on again prior to the completion of maintenance or servicing work.
There is a difference between turning off electrical equipment or a circuit and actually disconnecting it. When you turn off a switch, you are opening a circuit, but there’s still electrical energy at the switch. A short in the switch or someone inadvertently turning on the switch will start electrical current flow again. Lockout-Tagout procedures minimize this risk by preventing unexpected startup of electrical systems.
The victim at this facility assumed the electrical drawings were correct. Many people trust the circuit breaker labels and facility electrical drawings to determine the electrical circuits.
These drawings and plans should only be used a guidelines. (See recommendations discussion on as-built drawings No.5, and labeling No.7 for further discussion.)
In many facilities there might be a need for a qualified electrical contractor to conduct an electrical systems assessment to ensure proper Lockouts can be placed.
Many electrical incidents that have been reported over the past several years within the FACE program involved inexperienced or unqualified workers attempting to perform work on or near electrical systems. Factors contributing to these incidents included:
- Lack of a Lockout-Tagout process or procedure
- Lockout procedure not followed or used
- Inadequate assessment or inadequate identification of the hazards and control methods
- Improper or inadequate test equipment
- Being unfamiliar in the proper use of the test equipment
- Inadequate job planning
Never work on equipment or circuits unless they are de-energized, locked out and tagged. Test all circuits before starting work to ensure there is no power.
The following questions should be considered before working on electrical systems:
- Are the facility policies and procedures that govern the control of hazardous energy understood by all workers involved in the task?
- Is Lockout-Tagout necessary to safely perform the work?
- Has the consequence of proceeding without hazardous energy controls been considered?
- Has the pressure to complete the task become a factor?
- Has authorization been given to perform work without implementing hazardous energy controls?
- Has the proper level of oversight/supervision been assigned for this task?
- Who will verify that hazards have been properly isolated?
- Will isolation points be independently verified before start of work?
- Has a zero-energy condition been verified and the re-accumulation of energy been prevented?
Even for a minor repair, always follow proper Lockout-Tagout procedures.
Recommendation #3: Electrical systems and components must be tested to assure they are de-energized before performing work. Do not assume a light switch or breaker shuts off power to a device. If you can’t test, let it rest.
Discussion: Anyone who works on an electrical system should know how to verify that power has been shut off and isolated before any work is performed.
It appears the victim in this incident did not test the electrical system to make sure the emergency light was de-energized.
Testing electrical equipment requires technical knowledge of appropriate testing procedures, and protective equipment designed for electrical hazard.
Only a qualified person should use electrical testing devices to determine if the circuit or equipment is energized.
In this incident the victim made an attempt to shut down the power for the broken light. However, he was not able to accurately identify the power source to the light.
Use a circuit tester to make sure a device is not active after the power has been shut off – sometimes backup circuits may restore power. Never work on a live circuit, device, receptacle, or switch!
Always wear the proper protective equipment when testing or working near energized parts. The National Fire Protection Association (NFPA) Standard 70E stipulates what equipment is necessary based on the hazard level.
When conducting electrical tests, make sure you do not touch any metal parts including the probe tips.
There have been many serious burns, fatalities, and catastrophic system failures because testing equipment was incorrectly selected or incorrectly used on electrical circuits.
It’s important for contractors, maintenance personnel, and electricians to know the test equipment and test criteria required for specific applications before they work on them.
Never provide a path for electricity to go through your body — in a micro-second a routine electrical maintenance repair can turn tragic
Recommendation #4: Tools for de-energizing circuits should not be supplied to untrained personnel. Make sure appropriate testing devices are used and that personnel are knowledgeable and trained in their safe operation. In most cases a licensed electrician should perform the testing.
Discussion: Many workers have been seriously hurt or fatally injured by attempting to measure voltage on a circuit they thought was not live. In this investigation we noted that the victim had an electrical test device available to him, but he apparently did not use it.
Testing incidents often occur when companies do not have written policies and procedures in place for electrical system troubleshooting, maintenance, and repair.
There are several considerations when planning and conducting testing of an electrical system:
- Always use electrical-rated personal protective equipment (e.g., insulated gloves and boots, double-insulated tools, and rubber mats) when working on energized electrical circuits and equipment.
- Stop work if an unanticipated electrical hazard or condition is encountered and seek appropriate assistance.
- Employers need to provide proper training for their maintenance workers to include the hazards and limitations of each instrument. Have employees read and follow all manufacturers’ instructions. Seek the assistance of someone who has used the tester before or consult manufacturers for training opportunities.
- Although it’s highly recommended that testing electrical systems be done by a qualified person / electrician, all maintenance workers should know the basics.
Limit the use of multi-meters that have manual settings. A common problem is that employees switch to an ohmmeter or ammeter setting, instead of voltage, and then connect to a voltage source. Instead, consider using single-function voltmeters or other instruments that don’t depend on manual settings. To further reduce the chance of operator error, avoid meters that have manual test lead plug connections.
Select the appropriate tester and setting. Most testers are designed for a specific voltage range or a select set of ranges. The tester or setting should match the voltage of the equipment or type of system you will be working on or near. When you are unsure, stop and get help from a qualified source.
All test equipment and hand tools must be insulated and rated for the voltage of the circuits they will be used on. All tools and equipment used for maintenance must also be periodically inspected to ensure they are not damaged and are still in good working condition.
Make sure the test equipment has been calibrated, evaluated, and tested in accordance with the manufacturer’s specifications. Inspect the equipment and employee use of equipment in the field.
Providing some recurrent basic training and education in electrical systems and assessment process can save lives.
Recommendation #5: Don’t rely on “as built” electrical drawings to determine current electrical system design and operation. Systems must be verified in place by testing and tracing the actual configuration.
Discussion: To meet general safety requirements, all facilities should keep their one-line electrical drawings well documented and updated. When changes are made, the system needs to be reanalyzed to assess the impact and hazards to workers.
The lack of accurate drawings to safely isolate electrical systems has been noted in past electrical investigations as contributing factors in many electrical injuries. Therefore, employers should have their facility drawings, equipment and electrical systems, evaluated, identified, traced, and verified by qualified personnel to ensure they reflect as-built system configurations.
As part of the as-built drawing verification process, walk down the work site to (1) identify equipment to be worked on, (2) ensure that equipment to be isolated is clearly marked, (3) verify or modify drawings to reflect as-built conditions, and (4) identify additional hazards or other safety issues.
As-built drawings should not be the sole source for locating electrical systems unless they have been verified by a qualified person and a recent system assessment has been conducted.
Many electrical contractors analyze a circuit using a systems approach to determine exactly what is wrong. They also understand and effectively use tools such as prints, diagrams, and test instruments to identify problem components and have the knowledge on how to repair them safely.
Recommendation #6: The facility accident prevention guidelines for these types of lighting systems should describe this electrocution hazard for maintenance personnel.
Discussion: Washington Administrative Code WAC 296-800-140 requires employers to have an “Accident Prevention Policy.”
Workers must be informed about the potential hazards and the proper PPE for each task, and they must be trained to properly use their equipment and tools.
NFPA 70E states that employees, “Shall be trained in, and familiar with, the specific maintenance procedures and tests required.” It is recommended that this training should be repeated annually.
The employer should audit policies, procedures and employee qualifications regularly. Make sure procedures and employee training are up-to-date with current standards and equipment used.
All electrical safety programs must include documented safety training and self-certification for employees. Training must be conducted by instructors who can train employees to identify electrical hazards, assess and minimize hazards, and to utilize specific safe work practices and procedures.
Management that is fully committed to worker safety will ensure these procedures are implemented.
Recommendation #7: Electrical breakers should be clearly labeled to indicate their action, location, and purpose.
Discussion: Electricity travels in a circle: it moves along a “hot” wire toward a light or receptacle, supplies energy to the light, and then returns along the neutral wire to ground. This complete path is a circuit. In a lighting system wiring, a circuit usually indicates a group of lights or receptacles connected along such a path.
If each circuit breaker isn’t already numbered inside the electric panel, the employer should hire a qualified electrician to have them identified, tagged and numbered. After each number, it should be noted which devices the breaker controls. For an even more thorough mapping, you can sketch a floor plan and make notes that identify the breaker numbers for each light and receptacle in the facility.
It’s important to label equipment per NEC and NFPA standards. Both the NEC and NFPA 70E require equipment that may be worked on while energized to be field marked with arc-flash warning labels.
Employers should conduct and use facility surveys to ensure that all hazardous energy sources (including those in adjacent equipment) are identified before beginning any installation, maintenance, service, or repair tasks. Energy-isolating devices such as breaker panels should be clearly labeled.
Equipment should be reviewed for proper labeling and re-labeling needs, as conditions warrant.
Back to Top
Acknowledgements
This report was reviewed by stakeholders from labor and business communities and various Washington State and Federal worker safety agencies. Though we are unable to acknowledge specific individuals for their contributions to this report, we would like to recognize the following for their help and support of the FACE mission and objectives:
- The Employer’s representative involved in the incident
- The Forensics Engineering Firm who reviewed the electrical system
- IBEW-JATC
- DOSH Compliance Operations
- DOSH Enforcement
- Federal Face Program Management (NIOSH)
- Safety & Health Assessment & Research for Prevention (SHARP)
- Washington State Attorney General’s Office
Appendix – Site Photographs

|

|
|

|
|

|
|
Photo 6. This photo shows a new metal halide bulb that the assisted living organization is now using at the facility. The facility no longer keeps the metal halide bulbs on site. They have an electrical contractor come into the facility to replace any metal halide bulbs that are no longer working within their emergency lighting system.
|
Washington FACE Program/SHARP
To contact Washington State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
