
Truck Driver Fatally Injured After Falling Into an Ore Hopper
FACE 00AK007
Release Date: March 30, 2001
SUMMARY
A 58-year-old truck driver (the victim) was fatally injured as a result of falling into a hopper at an ore storage facility. The victim was driving a tractor with two trailers loaded with ore concentrate. After arriving at the storage facility and while waiting his turn to unload, he had released the tiedown straps holding the tarps onto the trailers. Strong winds blew the tarp and its rollbar off the top the first trailer, leaving them hanging over the side. The victim was unable to lift and secure the tarp and rollbar over his load. After he was signaled to enter the building housing the dumping platform, he drove the tractor through the entrance; the trailers remained outside the building. He then climbed onto the catwalk at the front of the first trailer. The facility operator tried to assist him but was unable to lift the rollbar high enough for the victim to grasp. She handed one of the front tiedown straps to him, and he was able to pull up the front end of the bar. Once the end of the bar was placed in a holding bracket, he exited the catwalk. When asked if he needed further assistance, the victim stated that he did not and would roll the tarp after the trailers were inside the building. The victim went back to the cab and pulled the trailers forward so that the operator could close the entry door.
The operator then secured and rigged the trailers for dumping and did not see the victim’s activities. After the trailers were secured and rigged, the operator looked for the victim. Not locating him inside the building, the operator went to the control room and radioed a waiting driver who stated that he had not seen the victim exit the building. The operator searched the area again and went back to the control room. She observed the victim’s feet in a video monitor that was used to view the ore transferring through a shoot to the last conveyor; his body was trapped in the shoot. The operator radioed for help and stopped the conveyor. Emergency medical personnel were requested. The victim was removed from the conveyor system and transport to a clinic where he was pronounced dead.
Based on the findings of the investigation, to prevent similar occurrences, employers should:
- Require tarps to remain secured to trailers until the trailer is ready to be unloaded;
- Ensure that workers are able to recognize and avoid hazardous situations, such as climbing on loads or anywhere outside a trailer’s catwalk;
- With the assistance of workers involved in the activity, develop procedures to remedy problems;
- Consider adding communication skills in safety classes during new hire orientation.
INTRODUCTION
At approximately 4:30 PM on July 19, 2000, a 58 year-old male truck driver (the victim) was found trapped in an ore shoot in a conveyor system. On July 21, 2000, the Alaska Department of Labor and Workforce Development (AKDOLWD) notified the Alaska Division of Public Health, Section of Epidemiology. An investigation involving an Injury Prevention Specialist for the Alaska Department of Health and Social Services, Section of Epidemiology ensued on the same day. The incident was reviewed with company safety representatives; United States Department of Labor, Occupational Safety and Health Administration officials; and the Alaska Medical Examiner. Alaska State Troopers, Medical Examiner, Mine Safety and Health Administration (MSHA), and the employer reports were requested. MSHA, who filed a report after jurisdictional clarification was obtained, initially investigated this incident.
Two companies were involved in the incident: a mining company and a commercial trucking company. Both were privately owned and had been in business for more than 25 years. The mining company had more than 350 employees at the incident site and was involved in exploration, mining, and concentration of metal ores.
The commercial trucking company had 50 employees at the incident site of which 30 to 35 were drivers. The commercial trucking company was contracted by the mining company to haul ore concentrate to a storage and barge loading facility 50 miles from the mine. The victim was a commercial driver with 30 years experience in heavy truck hauling and tractor-trailer operation and maintenance. He had worked at the site for 7 months. Two months after his hire, the trucking company changed ownership. The victim retained his job without any duty changes.
Both the mining and commercial trucking companies worked two 12-hour shifts, 7 days per week. They both had a written safety program that detailed specific work practices and employee conduct at the worksite. All employees attended an orientation to their company’s safety program upon initial hire. Drivers were assessed for knowledge of driving rules, techniques and skills; knowledge, use, and operation of scale, tripmaster, chains, tarps and safety pins; and knowledge of policies and procedures for loading and unloading ore trucks. A separate evaluation was conducted for each type of truck or tractor-trailer rig (freight, ore, fuel, low and wide deck) to be driven. Since the commercial trucking company was contracted to the mining company, employees were also required to attend all safety training classes conducted by or on behalf of the mining company. The commercial trucking company conducted monthly safety meetings.
INVESTIGATION
The incident occurred in an ore storage facility at a marine terminal, approximately 50 miles from the mine. The facility consisted of a building housing a dumping platform, a hopper, a control room, and a conveyor system to transfer the ore concentrate to one of two storage buildings. Ore concentrate was the consistency of talcum powder. This material coated the surfaces within the facility. Personnel were required to wear respirators in addition to a hardhat, safety glasses (or goggles), hearing protection, and gloves while inside the facility. During transport from the mine to the storage facility, all loads of ore concentrate were required to be covered with a tarp secured to the trailer. Weather was windy with estimated 65 mph gusts and was considered a factor in this incident.
The trailers involved in the incident were two 24-foot side dump trailers, connected in tandem behind a Mack truck with a 40-ton capacity (Figure 1). The overall length of the tractor-trailers was 74 feet. The trailers had 3-foot wide catwalks on either end.
Tractor-trailers were driven into the building and onto the dumping platform located adjacent to the hopper (Figure 2a and 2b).
The platform was 76 feet long and 10 feet wide. Four chains (two per trailer) were used to secure the driver side of the trailers to the platform. A hydraulic lift then raised the driver side of the platform and tipped the tractor-trailers as a single unit to unload ore concentrate through the trailers’ side dump doors. A wall, 41 inches tall and 76 feet long, separated the platform from the hopper. The wall was equipped with a lower guard to allow drivers to position the trailers close to the wall without damaging the tires and rims. Two spill aprons (one for each trailer) rotated into position under the trailer doors to help guide the ore concentrate into the hopper. The aprons were positioned with an approximate 4 feet long gap at the center, similar to the gap between the two trailers.
After being signaled to approach the building entrance by the facility operator, drivers stopped outside the entrance door to conduct a walk-around inspection of the tractor-trailer, pull safety pins on the trailer doors, and roll back the tarps immediately before entering. (Company policy dictated that tarps were to be secured during transport and that loads were to remain covered until this time. However, it was not unusual for drivers to loosen or remove tiedown straps, leaving the load covered, while waiting at the dump/storage site.) Tarps were rolled from the driver side to the passenger side. The tarp and rollbar were held in position on the top of the trailer by brackets. Drivers then notified the operator that they were ready to enter the dump facility.
Normally, the tractor-trailers were driven completely through the entrance onto the platform. Once inside the building, the facility operator closed the door, chained the trailers to the platform, connected vibrator lines, and opened air valves to release doglatches for the trailer doors. All personnel were required to enter the control room before the platform was tilted.
The hopper was 55 feet long and 13½ feet deep. It was 14 feet wide at the top and narrowed to a conveyor belt, approximately 3½ feet wide, at the bottom (Figure 3). When in operation, the belt moved at a speed of 20 to 35 feet per minute. A permanent ladder inside the hopper near the control room was used to access the bottom of the hopper to break-up large clumps or perform maintenance. Ore concentrate was transferred from the hopper to storage buildings (located on either side of the dump facility) via a series of conveyor belts. Ore concentrate was moved to the end of the hopper where it fell down a shoot to another belt.
Conveyor belts ran continuously except during maintenance. Each belt moved the ore concentrate to a shoot, where it would drop to the next belt (Figure 4a and 4b).
The second and third conveyor belts were also involved in this incident. The total distance along these belts was 1,016 feet with a maximum belt speed of 204 feet per minute. It was estimated that the time to travel the distance from the beginning of the second belt (below the hopper) to the end of the third belt was approximately 4½ minutes. At the beginning of the second belt, a clump sensor automatically stopped all belts if the sensor detected an ore height over 15 inches. Vertical clearance exiting the shoot housing (at the center of this belt) was 15 inches (Figure 4a). At the end of the third belt, a video camera was housed in the top of the shoot; a monitor for this camera was located in the control room. This allowed the operator to observe the ore transfer to a fourth and final belt (to the storage buildings).
On the day of the incident, the victim was on his third trip of the day and was in line waiting to enter the storage facility. The victim was observed loosening the tiedown straps of the tarps on the trailers. Wind gusts, estimated at 65 mph or greater, blew the tarp and rollbar off the first trailer, leaving it hanging over the passenger side of the dump doors. In this position, the tarp hung next to the dump doors and prevented the doors from opening properly. The victim was signaled to approach the building entrance. Prior to entering the building, he was observed by another driver to be moving around the tractor-trailers. He signaled the facility operator and drove the tractor-trailers forward. However, the victim stopped short. The tractor was through the building entrance; the trailers remained outside. He then exited the cab and climbed onto the front catwalk of the first trailer. The operator went to see why he stopped. Since it was necessary to bring the trailers close to the wall as possible, the tarp could possibly become trapped and damaged. While standing on the ground next to the front trailer, the operator helped the victim ith the front section of the tarp. She was unable to lift the rollbar to the victim, so she handed a strap to him so he could pull up the front end of the rollbar and place it in the bracket. She asked if he needed further assistance. He declined help, leaving the rollbar hanging at an angle across the dump doors. The victim stated that he could roll the tarp after he pulled completely into the building. He went back to the cab and drove the tractor-trailers onto the platform.
The operator closed the door, connected the chains and vibrator lines, and opened the air valves to the doglatches. During this time, she witnessed no unusual activity but did hear a couple of thumps. After finishing her activities, she called and looked for the victim near the platform and in the control room. Getting no response to her call, she radioed the next driver and asked if he had seen the victim exit the building. She searched the area again and went back to the control room. At this time, she looked at the video monitor connected to the camera inside the shoot to the final conveyor belt. She saw the victim trapped at the top of the shoot.
The operator immediately radioed for help and stopped the belts. Emergency medical personnel arrived 4 minutes after her call. The victim was extricated and CPR was started. The victim was transported to the mine site clinic where he was pronounced dead.
The incident was not witnessed, however two boot prints found on top of the ore concentrate in the front passenger side of the first trailer suggested that the victim had climbed onto the load while parked on the dump platform. Immediately after the incident, the tarp and rollbar was hanging at an angle; the back of the rollbar was about halfway down the back of the trailer (Figure 5). A portion of the tarp was found on top of the load (passenger side). In addition, a possible boot print was found on the top surface of the wall between the spill aprons. With the restricted area between the driver side of the tractor-trailer and the building wall, it was highly unlikely that the victim walked around the tractor-trailer without being noticed by the operator. Based upon these circumstances, the victim must have fallen into the hopper and then been carried by the first conveyor belt to the end of the hopper. He then fell through the first shoot and was carried by the second conveyor belt. He fell through the shoot at the end of this belt and was carried by the third conveyor belt in the transfer system to the third shoot, where his body became trapped.
The final event that led to the victim falling into the hopper could not be determined. From the top of a trailer, an object will fall to the bottom of the hopper in less than 2 seconds. A fall of this distance can potentially cause incapacitating injuries. The following are possible sequences leading to the incident:
- While standing on the load, the victim lost his balance and fell into the hopper; or
- The victim moved to the end of the first trailer by walking across the tarp on top of the load. He then reached over the side to grasp and pull up the tarp or the rollbar, lost his balance, and fell over the side of the trailer into the hopper; or
- The victim may have climbed outside of the rear catwalk on the first trailer in an attempt to pull up the rollbar. He either lost his grasp or balance and then fell into the hopper.
After the incident, the automatic and manual stop mechanisms for the conveyor belts, including the clump sensor and emergency stop cables, were tested and found functional.
CAUSE OF DEATH
The Medical Examiner’s report listed the cause of death as multiple crush and impact injuries.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should require tarps to remain secured to trailers until the trailer is ready to be unloaded.
Discussion: In this incident, the victim followed prescribed work practices that required the tarp to be secured to the trailer while driving to the storage facility. However, it was not an unusual practice for drivers to leave the load covered and loosen or release tiedown straps while waiting to unload. Employers should consider conducting random work site safety inspections and supervisor observations to evaluate compliance with and understanding of established standards and practices and assess possible additions and modifications to standard work practices. In addition, steps for specific practices to be outlined in a safety, health, and environmental program should be discussed with employees to identify routine practices and reasonable actions for unusual occurrences to ensure worker compliance.
Recommendation #2: Employers should ensure that workers are able to recognize and avoid hazardous situations, such as climbing on loads or anywhere outside a trailer’s catwalk.
Discussion: In this incident, the driver positioned himself outside of prescribed safe work areas (trailer catwalks, areas near the hopper with barriers or guardrails) in an extremely hazardous position. The fall protection system on the catwalks at the ends of the trailers had both guard rails and mid rails to prevent workers from falling from these raised platforms. In unusual circumstances, activities outside these areas must be discussed with a supervisor, and a fall protection system agreed upon before beginning a task on an elevated area.
Recommendation #3: With the assistance of workers involved in the activity, employers should develop procedures to remedy problems.
Discussion: In this incident, an unusual situation occurred where a tarp needed to be replaced on a trailer before the ore concentrate could be unloaded. A job safety analysis (JSA) is a procedure used to review methods or steps for a task, identify potential hazards, and outline recommended actions and procedures to be used to eliminate or control hazards. Key to an effective JSA is input from workers performing the task(s). Through their observations and experience, tasks can be broken down to a sequence of steps or actions, which are used to identify hazards connected to the task or produced by the environment. Employers, supervisors, and safety managers can then review and modify current safety strategies used to safeguard workers and promote a safe work environment.
Recommendation #4: Employers should consider adding communication skills in safety classes during new hire orientation.
Discussion: In this incident, the facility operator was unaware how the victim intended to retrieve and roll the tarp. Good communication skills are essential in all job situations. On-the-job communication includes discussions, statements, andadvisements before, during, and after work duties. These communications need to be clear and concise in order to advise or alert co-workers or other persons at the worksite to actions that could jeopardize the performance and/or efficiency of their job duties or that could cause potential injury. Employers should consider adding communication skills in safety orientation classes. Suggested techniques to aid in successful communication include:
- Make eye contact with the person or persons you are advising;
- Use the name of the person to whom you are speaking;
- Require a response before taking action.
REFERENCES
National Safety Council. Accident Prevention Manual for Business & Industry: Administration & Programs. 10th ed. Chicago IL; 1992.
Fatality Assessment and Control Evaluation (FACE) Project
The Alaska Division of Public Health, Section of Epidemiology performs Fatality Assessment and Control Evaluation (FACE) investigations through a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR). The goal of these evaluations is to prevent fatal work injuries in the future by studying the working environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact.
To contact Alaska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
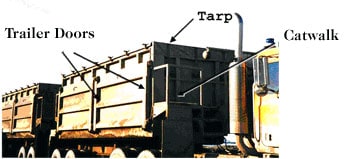
Figure 1. View of trailer and front catwalk

Figure 2a. Entrance to dump building

Figure 2b. Dumping platform and wall adjacent to hopper

Figure 3. Hopper, center divider, and conveyor belt at bottom

Figure 4a. Second conveyor belt exiting chute below hopper

Figure 4b. Second conveyor belt
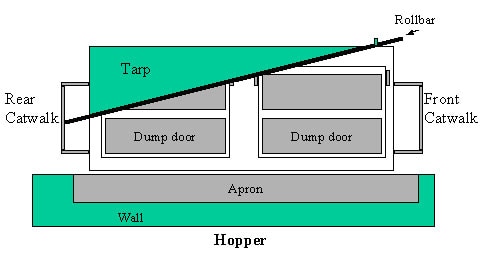
Figure 5. Diagram of tarp and rollbar hanging over side of front trailer (not to scale)