Selected Oral Health Indicators in the United States, 2005–2008
- Key findings
- Untreated dental caries and dental restoration prevalence varied by age.
- Untreated dental caries and existing dental restoration prevalence varied by race and ethnicity and poverty level across the lifespan.
- Among children and adolescents aged 5–19 years, dental sealant prevalence was highest among non-Hispanic white persons and those living at 200% or more of the poverty level.
- More non-Hispanic white and Mexican-American adults had retained all of their permanent teeth compared with non-Hispanic black adults.
- Edentulism was significantly higher among older adults living in poverty compared with those living at 200% of the poverty level or higher.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 96, May 2012
Please note: A correction was made to the online HTML and PDF versions on June 6, 2012. See the Figure 1 and Table notes for more details.
PDF Version (642 KB)
Bruce A. Dye, D.D.S., M.P.H.; Xianfen Li, M.S.; and Eugenio D. Beltrán-Aguilar, D.M.D., M.S., Dr.P.H.
Key findings
Data from the National Health and Nutrition Examination Survey, 2005–2008
- More than one in five people had untreated dental caries and 75% had existing dental restorations.
- Prevalence of untreated dental caries varied significantly by poverty level for all age groups; however, there was little difference in dental restoration prevalence by poverty level for children and adolescents aged 5–19 years.
- Twenty-seven percent of children and adolescents aged 5–19 years had at least one dental sealant.
- Nearly 38% of non-Hispanic black adults had not lost a permanent tooth compared with 51% for non-Hispanic white and 52% for Mexican-American persons.
- Almost 23% of adults aged 65 and over were edentulous.
Oral health is an important contributor to overall health for individuals and the population. Dental caries both untreated and treated and tooth loss are key indicators of oral health and are used to monitor oral health status in the United States and internationally (1,2). Although prevalence of dental caries has been declining in the United States, the magnitude of the decline has varied across different population groups during the past two decades (3). Tooth loss also has been declining in the United States (3), mostly due to improvements in treatment modalities, patient attitudes regarding tooth preservation, and better prevention (4). Plastic-like coatings (dental sealants) have been applied to the chewing surfaces of children’s teeth to prevent tooth decay and to some extent tooth loss. This report describes the prevalence of untreated dental caries, existing dental restorations, dental sealants, and tooth loss in the United States by age, race and ethnicity, and poverty level in 2005–2008.
Keywords: dental caries, dental sealants, edentulism, National Health and Nutrition Examination Survey
Untreated dental caries and dental restoration prevalence varied by age.
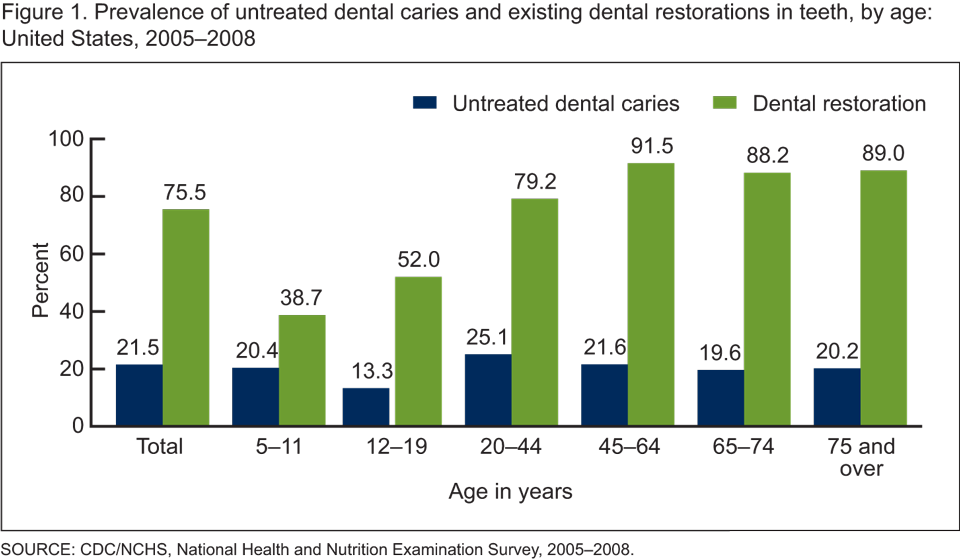
Figure 1. Prevalence of untreated dental caries and existing dental restorations in teeth, by age: United States, 2005–2008
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2008.
CORRECTION: The word “permanent” was removed from the title of Figure 1 and the Table. This change was made to clarify that the prevalence estimates shown for tooth decay and dental restorations was for all teeth present at the time of assessment, not permanent teeth alone.
In 2005–2008, more than one in five people had untreated dental caries and three in four people had at least one dental restoration in the United States (Figure 1). Untreated dental caries among children aged 5–11 years was 20% and was 13% among adolescents aged 12–19. The prevalence of untreated caries among younger adults aged 20–44 was 25% and gradually decreased among the older age groups to approximately 20% for adults aged 65 and over. The prevalence of existing dental restorations increased as individuals aged from childhood into adulthood and plateaued in age groups starting at 45 and over. Thirty-nine percent of children aged 5–11 years and 52% of adolescents aged 12–19 had a dental restoration. The prevalence of having a dental restoration increased to 79% for adults aged 20–44 and then to nearly 92% for those aged 45–64. For older adults, dental restoration prevalence was 88% for those aged 65–74 and 89% for those aged 75 and over.
Untreated dental caries and existing dental restoration prevalence varied by race and ethnicity and poverty level across the lifespan.
Prevalence of untreated caries was nearly twice as high for non-Hispanic black persons (34%) compared with non-Hispanic white persons (18%) in 2005–2008 (Table). Prevalence of untreated caries was significantly higher for both non-Hispanic black and Mexican-American persons compared with non-Hispanic white children, adults, and older adults. Among persons aged 5–19 years, untreated caries were at least twice as high for those living below 100% of the poverty level (25%) compared with those living at 200% of the federal poverty level or higher (12%). Prevalence of untreated caries was significantly higher for adults living below 100% of the federal poverty level compared with those living at the 200% level or higher.
Table. Prevalence of untreated dental caries and existing dental restorations in teeth, by sex, race and ethnicity, and poverty level: United States, 2005–2008
| Characteristic | Untreated dental caries | Dental restoration | ||||||
|---|---|---|---|---|---|---|---|---|
| Age in years | ||||||||
| Total | 5–19 | 20–64 | 65 and over | Total | 5–19 | 20–64 | 65 and over | |
| Total | 21.5 | 16.6 | 23.7 | 19.9 | 75.5 | 45.9 | 84.3 | 88.5 |
| Race and ethnicity | ||||||||
| Non-Hispanic white1 | 17.8 | 13.3 | 19.3 | 17.8 | 80.1 | 46.2 | 88.8 | 91.6 |
| Non-Hispanic black | 234.2 | 222.6 | 239.7 | 235.8 | 262.6 | 240.4 | 273.1 | 263.7 |
| Mexican American | 231.1 | 222.4 | 235.2 | 236.4 | 261.8 | 50.1 | 267.4 | 269.3 |
| Poverty level | ||||||||
| Below 100% | 235.8 | 225.4 | 241.9 | 241.3 | 262.7 | 48.6 | 271.5 | 263.3 |
| 100% to less than 200% | 230.5 | 219.3 | 237.7 | 222.5 | 268.8 | 46.3 | 275.1 | 285.6 |
| 200% or higher1 | 15.5 | 12.1 | 16.6 | 15.3 | 80.2 | 44.5 | 89.0 | 92.6 |
| Sex | ||||||||
| Male | 224.6 | 17.6 | 227.2 | 225.1 | 272.1 | 44.8 | 280.5 | 286.3 |
| Female1 | 18.6 | 15.5 | 20.2 | 15.6 | 78.7 | 47.0 | 88.0 | 90.4 |
1Reference group.
2p < 0.05.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2008.
CORRECTION: The word “permanent” was removed from the title of Figure 1 and the Table. This change was made to clarify that the prevalence estimates shown for tooth decay and dental restorations was for all teeth present at the time of assessment, not permanent teeth alone.
Dental restoration prevalence was significantly lower for both non-Hispanic black and Mexican-American persons (62%) compared with non-Hispanic white persons (80%) in 2005–2008. Although both non-Hispanic black and Mexican-American adults had a significantly lower prevalence of dental restorations compared with non-Hispanic white adults, only non-Hispanic black children and adolescents (40%) had a significantly lower prevalence compared with non-Hispanic white children and adolescents (46%). Among persons aged 5–19 years, the prevalence of dental restorations ranged from nearly 45% for those living at 200% or higher of the federal poverty level to nearly 49% for persons living below 100% of the poverty level. Prevalence of dental restorations was significantly lower for adults aged 20–64 living below 100% of the poverty level (72%) compared with adults living at 200% of the poverty level or higher (89%). For adults aged 65 and over living in poverty, dental restoration prevalence was significantly lower (63%) compared with those living at 200% of the poverty level or higher (93%).
Among children and adolescents aged 5–19 years, dental sealant prevalence was highest among non-Hispanic white persons and those living at 200% or more of the poverty level.
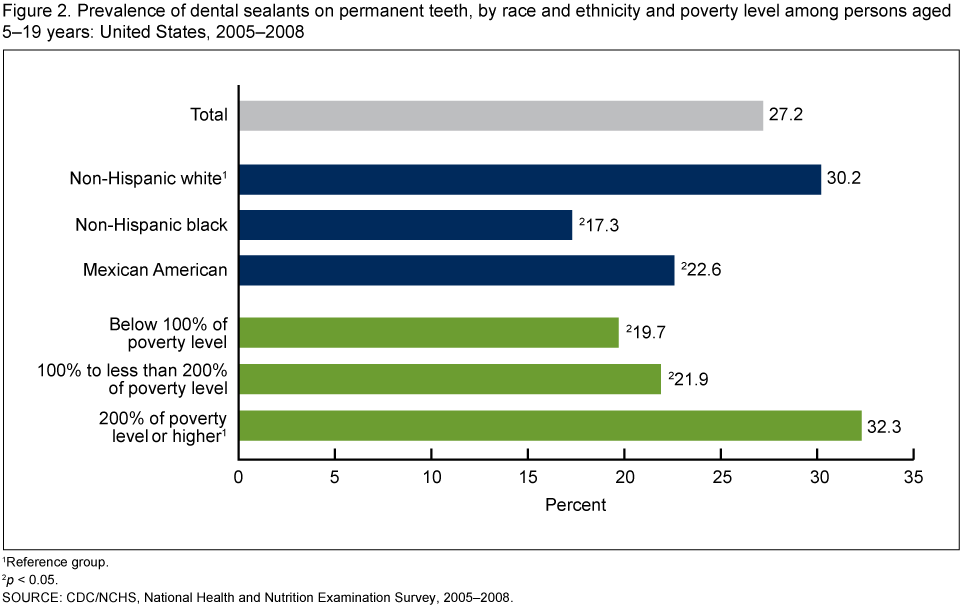
Twenty-seven percent of children and adolescents aged 5–19 years had at least one dental sealant on a permanent tooth. Thirty percent of non-Hispanic white children and adolescents had a dental sealant compared with 23% for Mexican-American and 17% for non-Hispanic black children and adolescents (Figure 2). Dental sealant prevalence was significantly lower for children and adolescents aged 5–19 years living below 200% of the poverty level (20%–22%) compared with those living at 200% of the poverty level or higher (32%).
Figure 2. Prevalence of dental sealants on permanent teeth, by race and ethnicity and poverty level among persons aged 5–19 years: United States, 2005–2008
1Reference group.
2p < 0.05.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2008.
More non-Hispanic white and Mexican-American adults had retained all of their permanent teeth compared with non-Hispanic black adults.
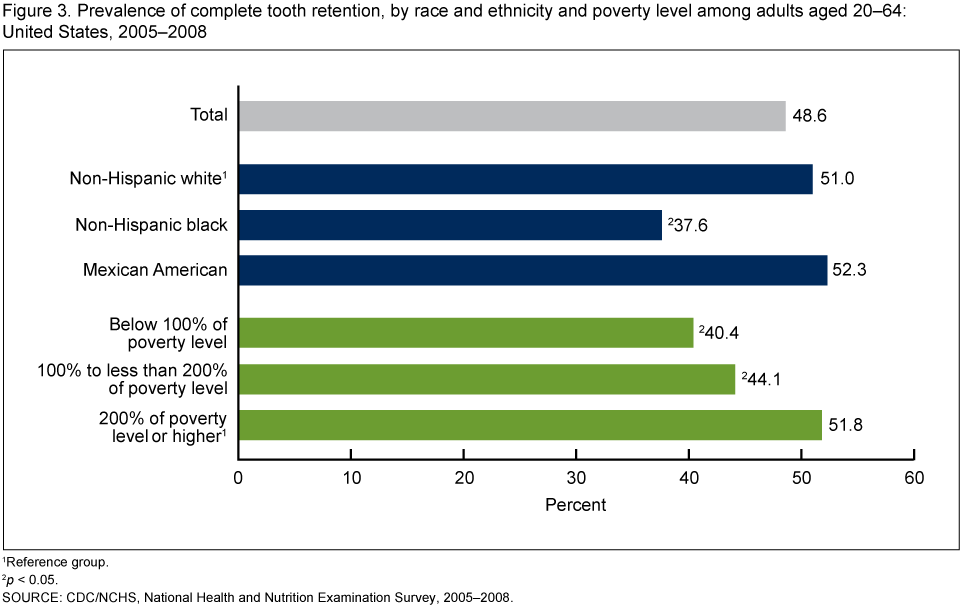
Approximately 49% of adults aged 20–64 had a full set of permanent teeth (excluding third molars) (Figure 3). Tooth retention was higher among Mexican-American (52%) and non-Hispanic white (51%) persons, whereas only 38% of non-Hispanic black persons had experienced no tooth loss due to dental disease. For adults aged 20–64 living at 200% of poverty level or higher, 52% had not lost a permanent tooth; approximately 40% of adults living below 100% of the poverty level had retained all of their permanent teeth.
Figure 3. Prevalence of complete tooth retention, by race and ethnicity and poverty level among adults aged 20–64: United States, 2005–2008
1Reference group.
2p < 0.05.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2008.
Edentulism was significantly higher among older adults living in poverty compared with those living at 200% of the poverty level or higher.
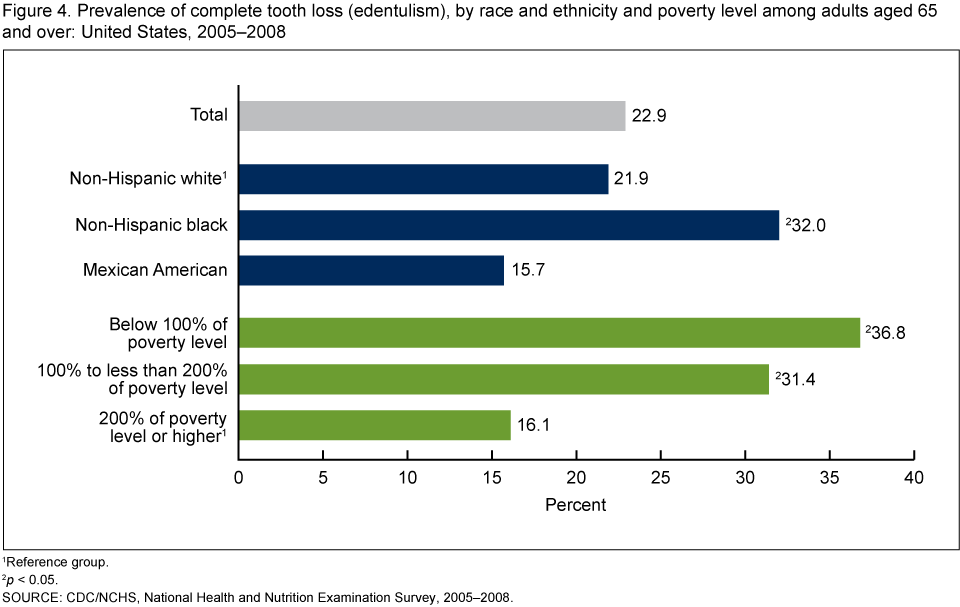
Twenty-three percent of adults aged 65 and over were edentulous (Figure 4). More non-Hispanic black adults aged 65 and over were edentulous (32%) compared with non-Hispanic white adults (22%), whereas only 16% of Mexican-American adults had complete tooth loss. The prevalence of complete tooth loss was more than twice as high for older adults living below 100% of the poverty level (37%) compared with those living at 200% of the poverty level or higher (16%).
Figure 4. Prevalence of complete tooth loss (edentulism), by race and ethnicity and poverty level among adults aged 65 and over: United States, 2005–2008
1Reference group.
2p < 0.05.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005–2008.
Summary
In the United States, oral health status varied by age, race and ethnicity, and poverty level. Approximately 17% of children and adolescents aged 5–19 years had untreated dental caries and 46% had a dental restoration. Twenty percent of children aged 5–11 years and 13% of adolescents aged 12–19 had untreated caries. Untreated dental caries was significantly higher in Mexican-American and non-Hispanic black children and adolescents (23%) compared with non-Hispanic white children and adolescents (13%). One-half of Mexican-American children and adolescents had a dental restoration. Dental restoration prevalence was significantly lower for non-Hispanic black persons (40%) compared with non-Hispanic white persons (46%). Although dental sealant prevalence was 27% for all children and adolescents, more non-Hispanic white persons (30%) had a dental sealant compared with Mexican-American (23%) and non-Hispanic black (17%) persons.
Twenty-five percent of children and adolescents living in poverty had untreated dental caries compared with 12% for those living at 200% of the poverty level or higher. There was little difference in dental restoration prevalence by poverty level among persons aged 5–19 years, with prevalence ranging from nearly 45% for those living at 200% or higher of the federal poverty level, to nearly 49% for persons living below 100% of the poverty level. Dental sealant prevalence was significantly lower for those living below 100% of the poverty level (20%) compared with those living at 200% or more of the poverty level (32%).
Nearly 24% of adults aged 20–64 had untreated dental caries and 84% had a dental restoration. Prevalence of untreated dental caries was significantly higher in non-Hispanic black (40%) and Mexican-American (35%) adults compared with non-Hispanic white adults (19%). Dental restoration prevalence was significantly lower for Mexican-American (68%) and non-Hispanic black (73%) adults compared with non-Hispanic white adults (89%). Although Mexican-American persons had untreated caries and dental restorations at levels indicating a significant disparity when compared with non-Hispanic white persons, complete tooth retention was comparable between Mexican-American (52%) and non-Hispanic white (51%) adults.
Untreated caries was significantly higher among adults aged 20–64 living in poverty (42%) compared with those living at 200% of the poverty level or higher (17%). Dental restoration prevalence was significantly lower for adults living in poverty (72%) compared with those living at 200% of the poverty level or higher (89%). More adults living at 200% of the poverty level or higher had not lost a tooth due to dental disease (52%) compared with those living below 100% of the poverty level (40%).
Twenty percent of adults aged 65 and over had untreated dental caries and 89% had a dental restoration. The prevalence of untreated caries and dental restorations was similar for older adults aged 65–74 and 75 and over. Twice as many non-Hispanic black and Mexican-American older adults (36%) had untreated caries compared with non-Hispanic white older adults (18%). Ninety-two percent of non-Hispanic white older adults had at least one dental restoration, whereas less than 70% of Mexican-American and non-Hispanic black older adults had a dental restoration. Edentulism was significantly higher among non-Hispanic black older adults (32%) compared with non-Hispanic white older adults (22%), but only 16% of Mexican-American older adults were edentulous.
Prevalence of untreated caries was nearly three times greater among adults aged 65 and over living in poverty (41%) compared with those living at 200% of the poverty level or higher (15%). Dental restoration prevalence was significantly lower for adults living in poverty (63%) compared with those living at 200% of the poverty level or higher (93%). Edentulism was more than twice as high among older adults living below 100% of the poverty level (16%) compared with those living at 200% of the poverty level or higher (37%).
Definitions
Untreated dental caries: Describes dental cavities that have not received appropriate treatment.
Dental restoration: Refers to having a dental filling, crown, or other type of restorative dental material applied to the tooth regardless of the dental material type, such as amalgam, composite resin, gold alloy, and ceramic.
Dental sealants: Describes plastic-like coatings applied to the chewing surfaces of back teeth. The applied sealant resin bonds into the grooves of teeth to form a protective physical barrier.
Tooth retention: Refers to having all natural permanent teeth present, excluding third molars.
Edentulism: Refers to having all natural permanent teeth missing, including third molars.
Poverty status or percentage of poverty level: Poverty status is based on family income, family size, and the number of children in the family, and for families with two or fewer adults, on the age of the adults in the family. The poverty level is based on definitions originally developed by the Social Security Administration and includes a set of income thresholds that vary by family size and composition. Families or individuals with income below their appropriate thresholds are classified as below the poverty level. These thresholds are updated annually by the U.S. Census Bureau. Additional information can be found on the U.S. Department of Health and Human Services website.
Data source and methods
Data from the National Health and Nutrition Examination Survey (NHANES) were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population. The NHANES sample is selected through a complex, multistage design that includes selection of primary sampling units (PSUs) (counties or county equivalents), household segments within PSUs, and sample persons from selected households. The sample design includes oversampling in order to obtain reliable estimates of health and nutritional measures for population subgroups. In 2005–2008, oversampling included non-Hispanic black and Mexican-American persons. Additional information on NHANES can be found on the NHANES website
From 2005 through 2008, the NHANES oral health assessment was conducted in mobile examination centers by trained health technologists rather than dental professionals. The oral health screening included a person-based assessment for dental caries, restorations, and sealants, and was conducted using a dental light for illumination, and a disposable mirror. The screening was a fast and simple process by which an examiner visually inspected the oral cavity to detect the presence or absence of specific oral conditions. Overall examiner reliability findings indicated that health technologist performance was excellent. Additional information regarding the 2005–2008 oral health screening and quality assurance issues are published elsewhere (5).
Population estimates and standard errors were calculated in SAS-callable SUDAAN software (release 10.0; RTI International, Research Triangle Park, N.C.). Sample weights to account for differing probabilities of selection, nonresponse, and noncoverage were used for analysis. The standard errors of the percentages were estimated using Taylor series linearization, to take into account the complex sampling design. The statistical significance of differences between estimates were evaluated using two-sided t tests at the α = 0.05 level compared with a reference group within the selected variable. Calculated estimates were not age adjusted and no adjustments were made for multiple comparisons.
About the authors
Bruce A. Dye and Xianfen Li are with the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics, Division of Health and Nutrition Examination Surveys. Eugenio D. Beltrán-Aguilar is with CDC’s National Center for Chronic Disease Prevention and Health Promotion, Division of Oral Health.
References
- U.S. Department of Health and Human Services. Healthy People 2010. 2nd ed. With: Understanding and improving health, and Objectives for improving health. 2 vols. Washington, DC: U.S. Government Printing Office. 2000.
- Petersen PE. The world oral health report 2003: Continuous improvement of oral health in the 21st century—The approach of the WHO Global Oral Health Programme. Geneva, Switzerland: World Health Organization. 2003.
- Dye BA, Tan S, Smith V, et al. Trends in oral health status: United States, 1988–1994 and 1999–2004. Vital Health Stat 11(248). 2007.
- Burt BA, Eklund SA. Dentistry, Dental Practice, and the Community, 6th ed. St. Louis, MO: W.B. Saunders Company. 2005.
- Dye BA, Barker LK, Li X, Lewis BG, Beltrán-Aguilar ED. Overview and quality assurance for the oral health component of the National Health and Nutrition Examination Survey (NHANES), 2005–08. J Public Health Dent 71(1):54–61. 2011.
Suggested citation
Dye BA, Li X, Beltrán-Aguilar ED. Selected oral health indicators in the United States, 2005–2008. NCHS data brief, no 96. Hyattsville, MD: National Center for Health Statistics. 2012.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health and Nutrition Examination Surveys
Clifford L. Johnson, M.S.P.H., Director