Dietary Supplement Use Among U.S. Adults Has Increased Since NHANES III (1988–1994)
- Key findings
- Dietary supplement use in the United States has increased since the National Health and Nutrition Examination Survey (NHANES) III (1988–1994).
- The prevalence of multivitamin/multimineral use has increased since NHANES III (1988–1994).
- The prevalence of supplemental calcium use has increased since NHANES III (1988–1994) for women aged 60 and over, but varies by racial and ethnic group.
- Use of dietary supplements containing folic acid differs by race and ethnicity among women aged 20–39.
- Use of dietary supplements containing vitamin D has increased since NHANES III (1988–1994).
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 61, April 2011
Jaime Gahche, M.P.H.; Regan Bailey, Ph.D., R.D.; Vicki Burt, Sc.M., R.N.; Jeffery Hughes, M.P.H.; Elizabeth Yetley, Ph.D.; Johanna Dwyer, D.Sc., R.D.; Mary Frances Picciano, Ph.D.; Margaret McDowell, Ph.D., R.D.; and Christopher Sempos, Ph.D.
Key findings
- Use of dietary supplements is common among the U.S. adult population. Over 40% used supplements in 1988–1994, and over one-half in 2003–2006.
- Multivitamins/multiminerals are the most commonly used dietary supplements, with approximately 40% of men and women reporting use during 2003–2006.
- Use of supplemental calcium increased from 28% during 1988–1994 to 61% during 2003–2006 among women aged 60 and over.
- Use of supplements containing folic acid among women aged 20–39 did not increase since 1988–1994. In 2003–2006, 34% of women aged 20–39 used a dietary supplement containing folic acid.
- Use of dietary supplements containing vitamin D increased from 1988–1994 through 1999–2002 for men and women in most age groups.
Dietary supplements can contain nutrients in amounts as high as or higher than the Institute of Medicine’s Recommended Dietary Reference Intakes, therefore contributing substantially to total nutrient intake. Dietary supplements are widely available to U.S. consumers, and monitoring their use over time is an important component of the National Nutrition Monitoring System (1). Failure to include these nutrients when assessing the adequacy of diets and nutrition in the U.S. population may lead to inaccurate and misleading results. This report provides estimates of dietary supplement use for specific population groups over time. In addition to overall use of dietary supplements, this report focuses on estimates for specific nutrients consumed through dietary supplement use.
Keywords: vitamin D, folic acid, calcium, trends
Dietary supplement use in the United States has increased since the National Health and Nutrition Examination Survey (NHANES) III (1988–1994).

- Dietary supplement use is widespread among U.S. adults aged 20 and over. The percentage of the U.S. population who used at least one dietary supplement increased from 42% in 1988–1994 to 53% in 2003–2006 (Figure 1).
- Women were most likely to use one or more dietary supplements than men for all three time periods.
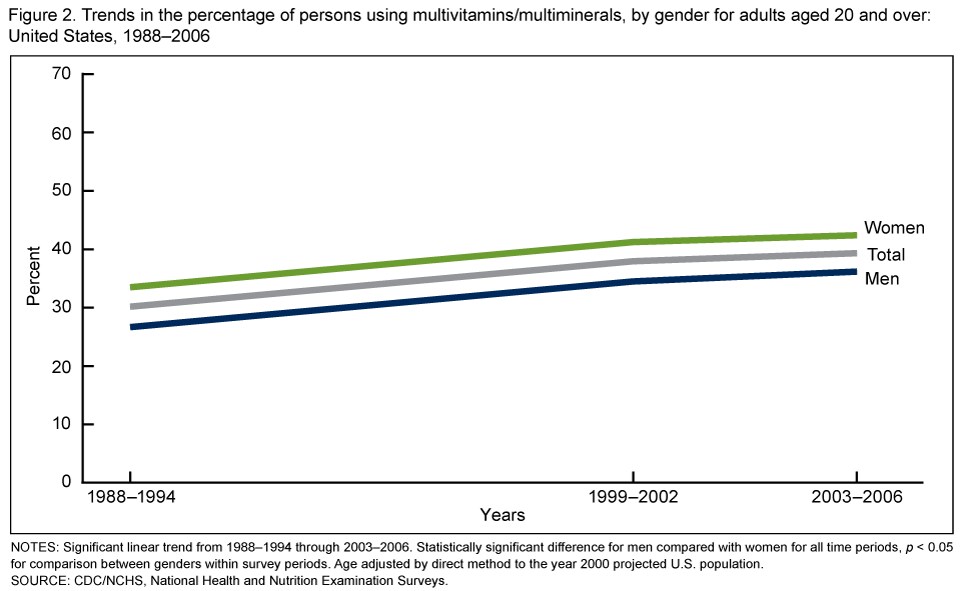
The prevalence of multivitamin/multimineral use has increased since NHANES III (1988–1994).
- Multivitamins/multiminerals are defined as dietary supplements that contain at least three vitamins and may or may not contain minerals (2). Multivitamins/multiminerals were the most frequently reported dietary supplement across all NHANES survey years.
- Patterns of use of multivitamins/multiminerals among adults aged 20 and over paralleled the pattern noted for all dietary supplement use (Figure 2).
- The percentage of the U.S. population who used at least one multivitamin/multimineral product increased from 30% in 1988–1994 to 39% in 2003–2006, with use more common among women than men.
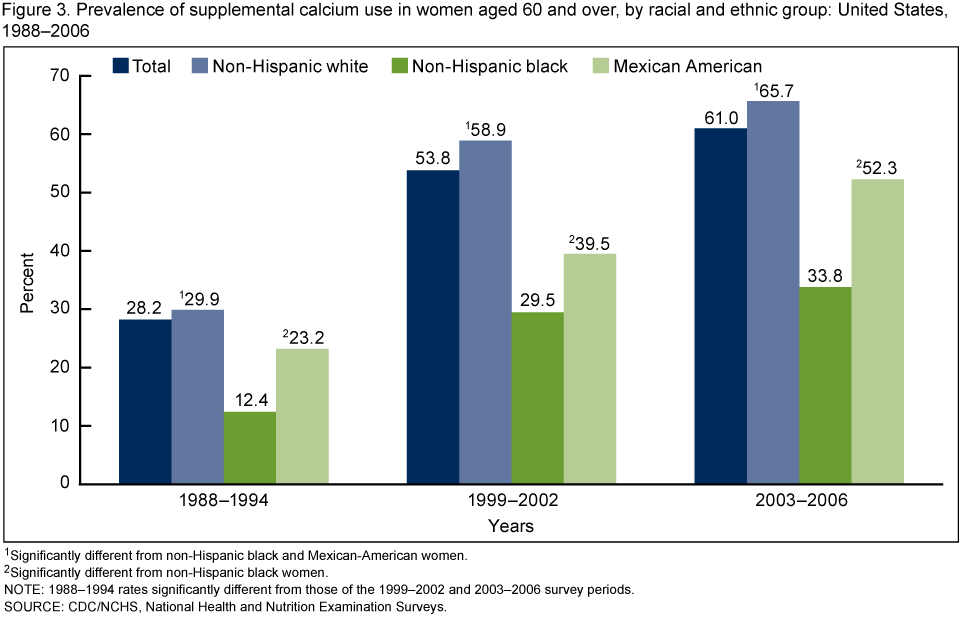
The prevalence of supplemental calcium use has increased since NHANES III (1988–1994) for women aged 60 and over, but varies by racial and ethnic group.
- Use of dietary supplements and antacids containing calcium increased from 1988–1994 through 1999–2002 among women aged 60 and over and in all racial and ethnic groups (Figure 3).
- Rates of supplemental calcium use continued to increase throughout 2003–2006 for women aged 60 and over and for non-Hispanic white women (58.9% in 1999–2002 to 65.7% in 2003–2006) and Mexican-American women (39.5% to 52.3%), but the observed increase for non-Hispanic black women was not significant.
- Non-Hispanic white women aged 60 and over were more likely to use at least one dietary supplement that contained calcium compared with non-Hispanic black and Mexican-American women for all survey periods.
- Mexican-American women aged 60 and over were more likely to use at least one dietary supplement that contained calcium than non-Hispanic black women for all survey periods.
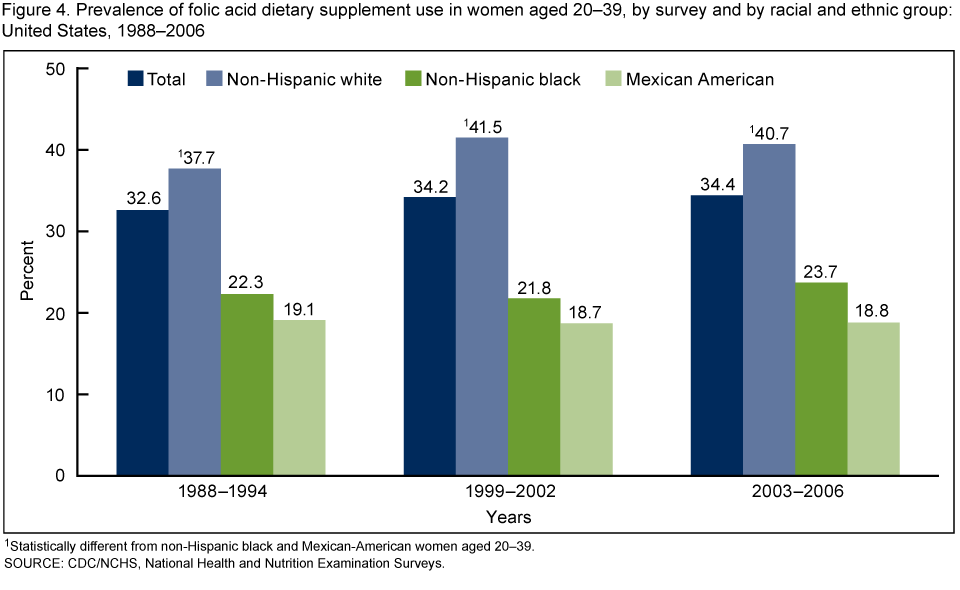
Use of dietary supplements containing folic acid differs by race and ethnicity among women aged 20–39.
- Rates of use of dietary supplements containing folic acid for all racial and ethnic groups remained stable from 1988–1994 through 2003–2006 for women aged 20–39 (Figure 4).
- Non-Hispanic white women were more likely to take one or more dietary supplements containing folic acid compared with both non-Hispanic black and Mexican-American women. The rates for non-Hispanic white women are approximately double that of the other two racial and ethnic groups.
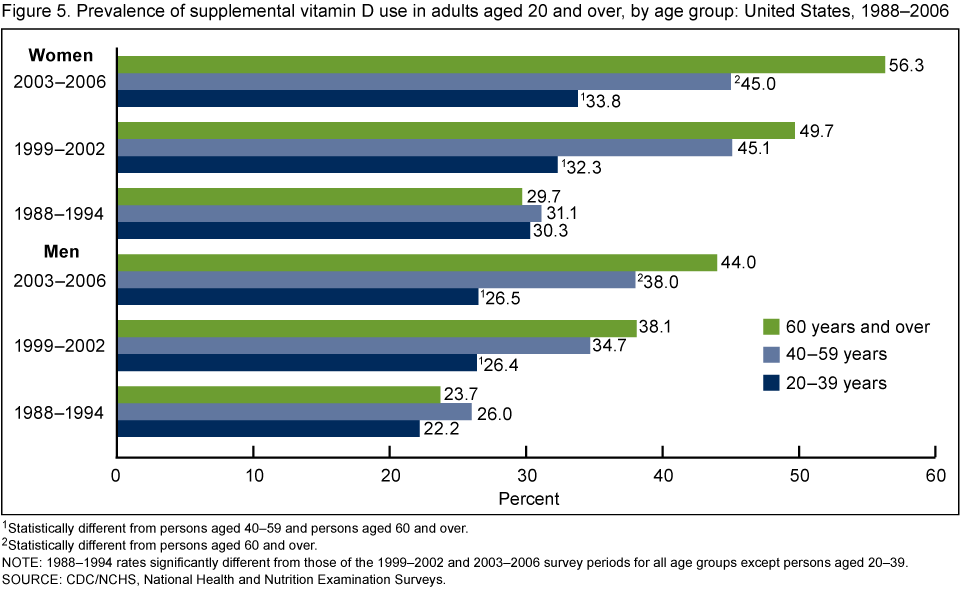
Use of dietary supplements containing vitamin D has increased since NHANES III (1988–1994).
- All age groups had similar rates of supplemental vitamin D use in 1988–1994 for both men (approximately 24%) and women (approximately 30%) (Figure 5). Rates for persons aged 20–39 remained stable for both men and women through 2003–2006, whereas for men and women aged 40–59, rates increased from 1988–1994 through 1999–2002 and remained stable in 2003–2006.
- The observed increase of supplemental vitamin D use for men aged 60 and over was not significant between the years 1999–2002 and 2003–2006 (38.1% in 1999–2002 to 44.0% in 2003–2006). For women aged 60 and over, the rates continued to increase through 2003–2006 (49.7% in 1999–2002 to 56.3% in 2003–2006).
Summary
This report indicates high use of dietary supplements in the U.S. adult population during the past 20 years, with over 40% of adults using one or more dietary supplements during 1988–1994, and over one-half of adults using supplements during 2003–2006. This is an increase from the 1970s when NHANES began monitoring use of dietary supplements. In NHANES I (1971–1975), age-adjusted supplement use prevalence was 28% among men and 38% among women aged 20 and over; in NHANES II (1976–1980), supplement use prevalence rates were 32% among men and 43% among women aged 20 and over (3). Because a high proportion of the U.S. population uses dietary supplements, it is essential for surveys and studies that assess nutrient intake to collect information on these important contributors. Of particular importance is vitamin D, which is found naturally in very few foods. Estimates of the population intake may be greatly underestimated if dietary supplements are not taken into account. In 2003–2006, 60% of women aged 60 and over took a dietary supplement containing calcium. The role of calcium in nutrient-disease or nutrient-health associations would be difficult to measure if dietary supplement use was not captured in studies. Folic acid intake is critical for women of childbearing age to prevent neural tube defects. Folate is widely available in foods such as green leafy vegetables, beans, and legumes. Additionally, the U.S. food supply is fortified with folic acid. Monitoring use of dietary supplements containing folic acid is important in evaluating the proportion of the population that has intake levels above recommendations. Therefore, it is critical to monitor intake from all sources to reach a more accurate intake estimate.
Definitions
Dietary supplement: As defined by the U.S. Congress in the Dietary Supplement Health and Education Act, which became law in 1994, a dietary supplement is a product (other than tobacco) that is intended to supplement the diet; contains one or more dietary ingredients (including vitamins, minerals, herbs or other botanicals, amino acids, and other substances) or their constituents; is intended to be taken by mouth as a pill, capsule, tablet, or liquid; and is labeled on the front panel as being a dietary supplement (4).
Adequacy of nutrient intake: Intake of a nutrient that meets the individual’s requirement for that nutrient.
Inadequacy of nutrient intake: Intake of a nutrient that fails to meet the individual’s requirement for that nutrient.
Calcium: The most abundant mineral in the body; found in some foods, added to others, available as a dietary supplement, and present in some medicines (such as antacids).
Vitamin D: A fat-soluble vitamin that occurs in many forms, is naturally found in very few foods, and is synthesized in the skin. The two dietary forms are D2 (ergocalciferol) and D3 (cholecalciferol).
Folate: A water-soluble B vitamin that is found in many foods
Folic acid: The synthetic form of folate that is found in dietary supplements and added to enriched flour and grain products such as breads, pasta, rice, and cereals.
Neural tube defect: A group of birth defects caused by incomplete development of the brain, spinal cord, or their protective coverings. Spina bifida is one of the most common defects.
Data source and methods
NHANES data were used for all of the analyses presented in this report, and all data are publicly available on the NHANES website. NHANES is conducted by the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics (NCHS) to monitor the health and nutritional status of the U.S. population. NHANES is a nationally representative sample of the U.S. civilian noninstitutionalized population. This population-based survey uses a complex, stratified, multistage probability cluster sampling design and oversamples in order to increase precision in estimates for certain groups. NHANES III was one in a series of periodic surveys conducted in two cycles during 1988–1994. In 1999, NHANES became a continuous survey, with data collected annually and released to the public in 2-year cycles. Across all NHANES waves, respondents were asked to participate in an interview at their home and in an examination conducted in a specially equipped mobile examination center.
NHANES includes information on participants’ demographic characteristics and health status, including dietary supplement use, as part of a personal interview conducted in the participant’s home. Dietary supplement data were collected using a similar methodology in both NHANES III and in 1999–2006. NHANES participants showed their prescription and nonprescription dietary supplement and nonprescription antacid containers to interviewers. In all survey periods, interviewers recorded the supplement name, manufacturer, and address, and collected information on duration of use, frequency of use in the past month or past 30 days, and the amount taken when used. Product label information was obtained by NCHS nutritionists and is also publicly released with the dietary supplement-use data.
NHANES data for adults aged 20 and over were used to calculate the prevalence of dietary supplement intake for three time periods (1988–1994, 1999–2002, and 2003–2006) by demographic characteristics for five supplement categories: 1) any supplement, 2) multivitamin/multimineral (contains at least three vitamins and may or may not contain minerals), 3) supplement with folic acid, 4) supplement with vitamin D, and 5) supplement with calcium, including antacids containing calcium. Demographic variables used in the analyses were age, gender, and race and ethnicity. Race and ethnicity were self-reported and categorized as Mexican American, non-Hispanic black, non-Hispanic white, and other. People in the “other” racial and ethnic category were included in analyses of the total sample, but results for this group are not shown separately. Pregnant women were excluded from the analytic sample. The analytic sample size was 37,596: 18,504 in NHANES 1988–1994; 9,660 in NHANES 1999–2002; and 9,432 in NHANES 2003–2006. Response rates were 81% in NHANES 1988–1994, 77% in NHANES 1999–2002, and 73% in NHANES 2003–2006.
All analyses used the interview sample weights, which account for unequal probabilities of selection, person-level nonresponse, and a poststratification adjustment to the estimated U.S. population. Taylor series linearization was used to calculate standard errors. All estimates that were not age-specific were age-adjusted to the 2000 U.S. standard population using three age groups: 20–39, 40–59, and 60 and over (5). Trends were tested to evaluate changes in estimates across survey periods. Differences among groups were assessed using a univariate t statistic. To account for multiple comparisons, statistical significance was set as a P value less than 0.0175, using the Bonferroni method to adjust for the three comparisons. Statistical analyses were conducted using SAS version 9.2 (SAS Institute, Cary, N.C.) and SUDAAN version 10.90 (Research Triangle Institute, Research Triangle Park, N.C.).
About the authors
Jaime Gahche, Vicki Burt, and Jeffery Hughes are with the CDC’s NCHS, Division of Health and Nutrition Examination Surveys. Regan Bailey, Elizabeth Yetley, Johanna Dwyer, Mary Frances Picciano (deceased, August 2010), and Christopher Sempos are with the National Institutes of Health’s (NIH) Office of Dietary Supplements. Margaret McDowell is with NIH’s National Institute of Diabetes and Digestive and Kidney Diseases.
References
- Heimbach JT. Using the national nutrition monitoring system to profile dietary supplement use. J Nutr 131(4 Suppl):1335S–8S. 2001.
- Radimer K, Bindewald B, Hughes J, Ervin B, Swanson C, Picciano MF. Dietary supplement use by US adults: Data from the National Health and Nutrition Examination Survey, 1999–2000. Am J Epidemiol 160(4):339–49. 2004.
- Briefel RR, Johnson CL. Secular trends in dietary intake in the United States. Annu Rev Nutr 24:401–31. 2004.
- Dietary Supplement Health and Education Act of 1994, Pub. L. No. 103–417, 103rd Congress (Oct. 25, 1994).
- Klein RJ, Schoenborn CA. Age adjustment using the 2000 projected U.S. population. Healthy People 2010 Stat Notes (20):1–10. 2001.
Suggested citation
Gahche J, Bailey R, Burt V, et al. Dietary supplement use among U.S. adults has increased since NHANES III (1988–1994). NCHS data brief, no 61. Hyattsville, MD: National Center for Health Statistics. 2011.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health and Nutrition Examination Surveys
Clifford L. Johnson, M.S.P.H., Director