Use of Advance Directives in Long-term Care Populations
- Key findings
- Data from the 2004 National Nursing Home Survey and the 2007 National Home and Hospice Care Survey
- Use of ADs varies across long-term care populations.
- Use of ADs varies by age, and age relationships differ by population.
- Black care recipients were less likely than white care recipients to use any AD.
- Living wills and do not resuscitate orders were the two most common types of ADs.
- Summary
- Definitions
- Data sources, methods, and limitations
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 54, January 2011
PDF Version (823 KB)
Adrienne L. Jones, Abigail J. Moss, and Lauren D. Harris-Kojetin, Ph.D.
Division of Health Care Statistics
Key findings
Data from the 2004 National Nursing Home Survey and the 2007 National Home and Hospice Care Survey
- Overall, 28% of home health care patients, 65% of nursing home residents, and 88% of discharged hospice care patients had at least one advance directive (AD) on record.
- The most common types of ADs among home health care patients, nursing home residents, and discharged hospice care patients were living wills and do not resuscitate orders.
- Care recipients under age 65 years were less likely to have any AD than those aged 85 and over; black care recipients were less likely than white care recipients to have any AD in all three populations. These age and racial differences were larger in the home health care and nursing home populations than in the hospice care population.
An advance directive (AD) allows a patient to communicate health care preferences in the event that he or she is no longer able to make these decisions (1). Many view advance care planning (ACP)-a process that includes discussing values and goals of care among the patient, family, and physician, and determining or executing treatment directives-as a way to help ensure that wishes about end-of-life care are honored (2). Ideally, ADs are part of the ACP process. Twenty years ago, Congress passed the Patient Self-Determination Act (PSDA) requiring most health care facilities to inform adult patients about their rights to execute an AD (2). Research indicates that the preference for having an AD can be influenced by individual attitudes, cultural beliefs, health conditions, and trust in health care professionals (2-9). This report presents the latest national data on ADs in three long-term care populations-those receiving home health care or hospice care and those residing in nursing homes.
Keywords: patient self-determination act, advance care planning, aging, end of life
Use of ADs varies across long-term care populations.
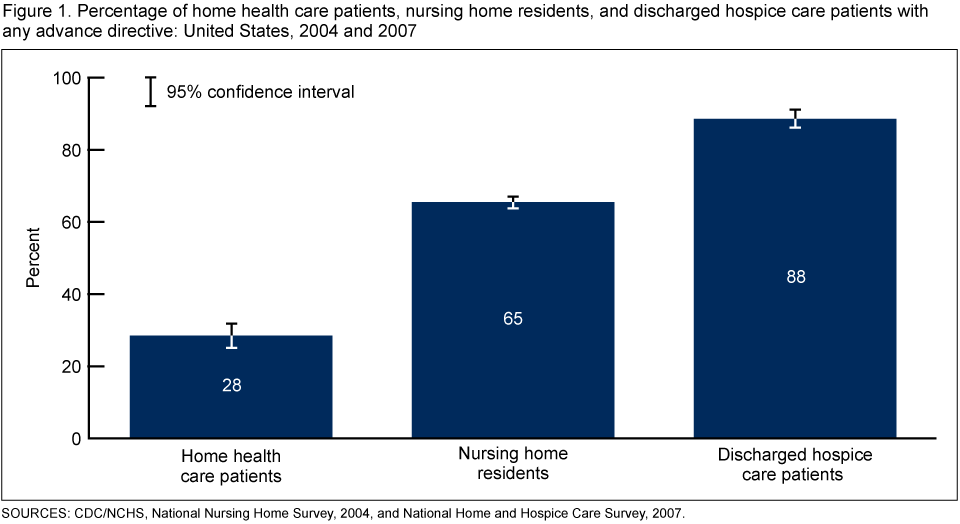
- Among the three long-term care populations, having at least one AD in the medical record was highest among discharged hospice care patients (88%) and lowest among home health care patients (28%), with 65% of nursing home residents having at least one AD (Figure 1).
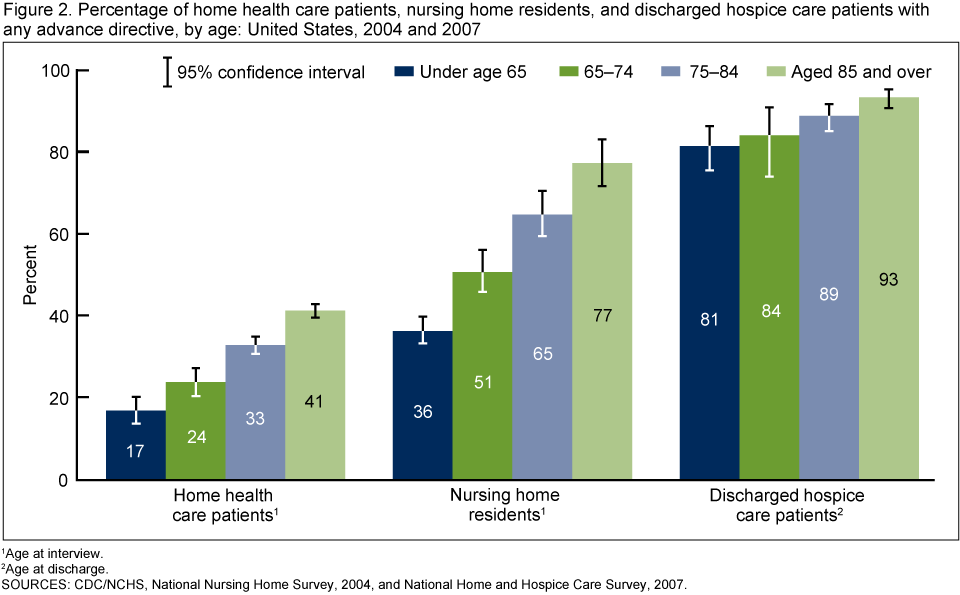
Use of ADs varies by age, and age relationships differ by population.
- Among home health care and nursing home populations, those aged 85 years and over were more than twice as likely as those under age 65 to have an AD-41% compared with 17% for home health care patients and 77% compared with 36% for nursing home residents (Figure 2).
- Age differences existed among discharged hospice care patients, but they were less pronounced than in other settings-93% of those aged 85 and over compared with 81% of those under age 65.
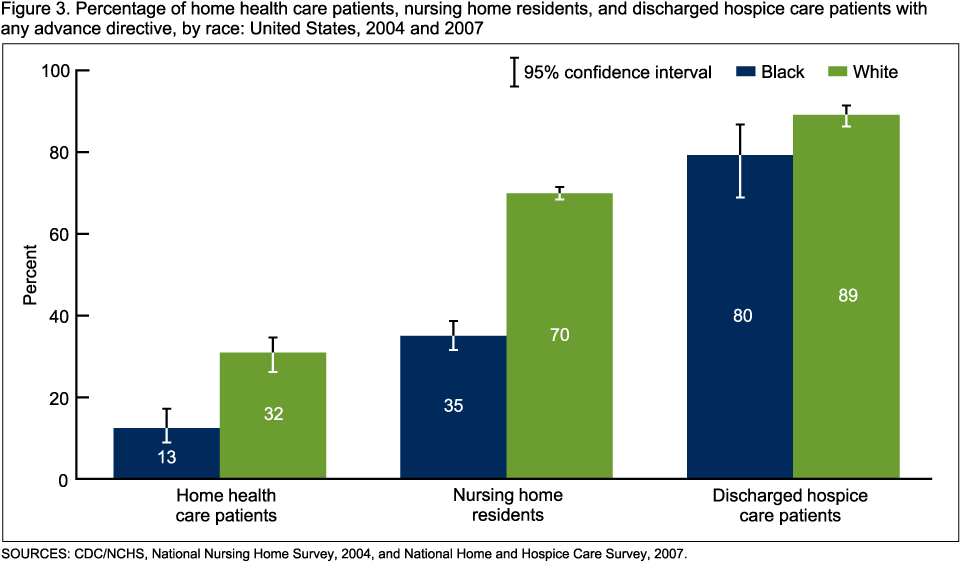
Black care recipients were less likely than white care recipients to use any AD.
- Black care recipients were half as likely to have an AD when compared with white care recipients in the home health care (13% compared with 32%) and nursing home (35% compared with 70%) populations (Figure 3).
- In the hospice care setting, black care recipients (80%) were also less likely than white
care recipients (89%) to have an AD; however, the differences were smaller.
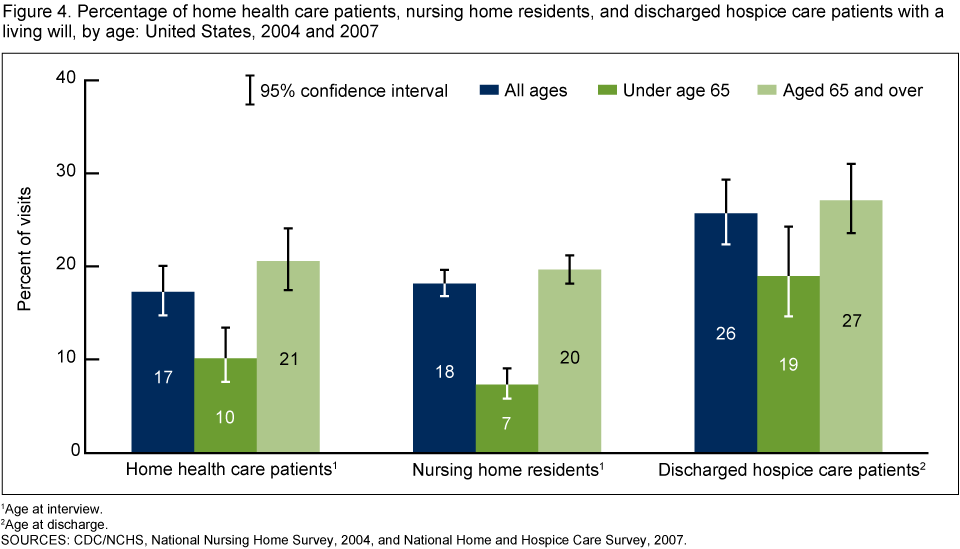
Living wills and do not resuscitate orders were the two most common types of ADs.
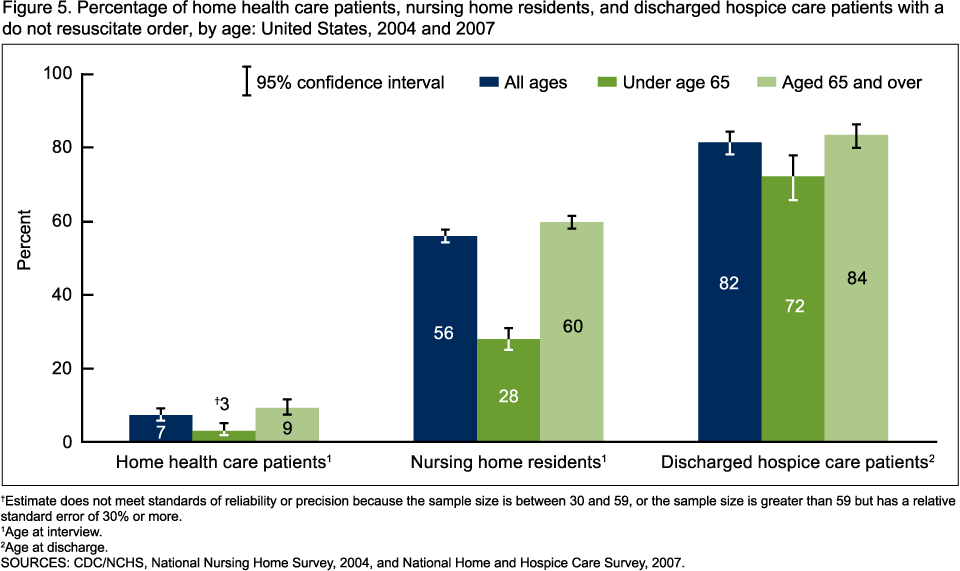
- Do not resuscitate (DNR) orders were more common than living wills among nursing home residents (56% compared with 18%) and discharged hospice care patients (82% compared with 26%) (Figures 4 and 5). In contrast, DNR orders (7%) were less common than living wills (17%) among home health care patients.
- Living wills and DNR orders were more prevalent among discharged hospice care patients than among home health care patients and nursing home residents. These differences were similar to those found for having any advance directive (Figure 1).
- Those aged 65 and over were more likely than their younger counterparts to have living wills in the nursing home (20% compared with 7%) and home health care populations (21% compared with 10%), and to have DNR orders among nursing home residents (60% compared with 28%) (Figures 4 and 5). Within the hospice care population, those aged 65 and over were also more likely than their younger counterparts to have living wills (27% compared with 19%) and DNR orders (84% compared with 72%), but the contrast was not as large as in the nursing home and home health care populations.
- White nursing home residents (20%) were three times as likely as black residents (6%) to have living wills and two times as likely (61%) as black residents (28%) to have DNR orders (not shown). Among the hospice care population, white patients (83%) were more likely than black patients (71%) to have DNR orders (not shown). The prevalence of living wills or DNRs among black home health care patients and the prevalence of living wills among black discharged hospice care patients are not reported because they did not meet standards of reliability.
Summary
Previous studies have found that 20 years after the PSDA was passed, population-based prevalence estimates of completed advance directives among adults in the United States range from 5% to 15% (10,12). However, this study found a higher prevalence of advance directives among adults in all three long-term care populations compared with the overall U.S. adult population. The extent to which the PSDA has influenced this higher prevalence among long-term care populations is an important area for formal evaluation. The data about nursing home residents are from 2004 and, therefore, may not reflect the current situation.
This analysis also found that having an AD is associated with the type of long-term care received. Nursing home residents and discharged hospice care patients were more than twice as likely as home health care patients to have an AD on record. This seems logical given that the vast majority of discharged hospice care patients in 2007 had the Medicare hospice benefit that requires a physician to certify the patient has a life expectancy of 6 months or less. Further, both nursing home residents and hospice care patients on average are more likely to die sooner than people receiving home health care. Given that nearly 90% of discharged hospice care patients had ADs, most hospice care patients appear aware of their rights to execute an AD.
Among the home health care and nursing home populations, those aged 65 and over were more likely than their younger counterparts to have an AD. This finding mirrors the age difference in advance directive completion found in the broader population. One study found that 37% of community-dwelling older adults had completed an advance directive; this compares with 5% to 15% of all community-dwelling adults (12). This finding may reflect higher rates of disability and chronic conditions among persons aged 65 and over, which may potentially make people more likely to consider their end-of-life care preferences.
Black care recipients were less likely than white care recipients to have any AD across all three long-term care populations. Previous, smaller-scale studies have identified differences between white adults and black adults in the use of ADs and explored potential reasons for them. These reasons include lower levels of awareness about ADs among African-American adults compared with white adults; different attitudes toward ADs among providers serving different populations; and beliefs and values among African-American persons that may contribute to these differences, including greater preferences for life-sustaining therapies, less comfort discussing death, and greater distrust of the health care system (1,4,6,8,9,11). Because religious beliefs may affect perceptions of ADs, a potentially important area for future research is the role of religion in AD use and how that may vary among populations. By presenting the first national look at racial differences in use of ADs across long-term care populations, this report highlights the importance of research to give long-term care providers the information needed to implement the PSDA in culturally sensitive ways.
Definitions
Home health care patient: A patient on the home health care agency’s roster as of midnight the night before the interview.
Nursing home resident: A resident on the nursing home’s roster as of the night before the interview. Included were all residents for whom beds were maintained, even though they might have been away on overnight leave or in a hospital.
Discharged hospice care patient: A patient formally discharged from care by the hospice agency during a designated 3-month reference period prior to the month of the interview. Both live and dead discharges were included. A patient might be represented more than once in the data if the patient was discharged more than once in the prior 12 months; therefore, discharges represent episodes of care rather than patients.
Age at time of interview: Variable used to calculate age for home health care patients and nursing home residents.
Age at time of discharge: Variable used to calculate age for discharged hospice care patients.
Race: The patient’s or resident’s race as reported by agency or facility staff. The race categories in this report are white and black.
Home health care: A range of medical and therapeutic services as well as other services delivered at a patient’s home or in a residential setting for the purpose of promoting, maintaining, or restoring health, or maximizing the level of independence, while minimizing the effects of disability and illness, including terminal illness.
Hospice care: Focused on relieving pain and uncomfortable symptoms of persons with terminal illness and providing emotional and spiritual support to both the terminally ill and their families.
Living will: A written document that allows a person to state in advance his or her wishes regarding the use or removal of life-sustaining procedures in the event of illness or injury.
Do not resuscitate (DNR) order: A written order from a doctor that resuscitation should not be attempted if a person suffers cardiac or respiratory arrest. A DNR order may be instituted on the basis of an AD from a patient or from someone entitled to make decisions on the patient’s behalf, such as a health care proxy.
Data sources, methods, and limitations
Data for these analyses come from the 2004 National Nursing Home Survey (NNHS) resident file and the 2007 National Home and Hospice Care Survey (NHHCS) current patient and discharge file. The 2004 NNHS and 2007 NHHCS are periodic cross-sectional surveys of nationally representative samples of U.S. nursing homes, home health agencies, and hospice care organizations.
To measure “any advance directive,” the analyses for Figures 1–3 included all AD types collected-all six common to NNHS and NHHCS as well as ones unique to each survey. ADs common to both NNHS and NHHCS are living will, DNR order, do not hospitalize, feeding restrictions, medical restrictions, and organ donation. In addition to the six common types of ADs, NNHS collected one other type of AD-autopsy; less than 1% requested an autopsy. NHHCS collected three other types of ADs-durable power of attorney, health care proxy/surrogate, and comfort measures. For home health care patients, 14% requested power of attorney, 5% requested health care proxy/surrogate, and less than 1% requested comfort measures. For discharged hospice care patients, 36% requested power of attorney, 16% requested health care proxy, and 12% requested comfort measures.
Differences between subgroups were evaluated with two-tailed t tests using p<0.05 as the level of significance. All comparisons reported in the text are statistically significant unless otherwise indicated. Data analyses were performed using SAS version 9.1 (SAS Institute, Cary, N.C.) and SUDAAN version 9.0 (RTI, Research Triangle Park, N.C.).
About the authors
Adrienne L. Jones, Abigail J. Moss, and Lauren D. Harris-Kojetin are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health Care Statistics.
References
- Smith AK, McCarthy EP, Paulk E, Balboni TA, Maciejewski PK, Block SD, Prigerson HG. Racial and ethnic differences in advance care planning among patients with cancer: Impact of terminal illness acknowledgment, religiousness, and treatment preferences. J Clin Oncol 26 (25):4131–7. 2008.
- U.S. Department of Health and Human Services; Office of the Assistant Secretary for Planning and Evaluation; Office of Disability, Aging and Long-Term Care Policy. Advance directives and advance care planning: Report to Congress. 2008 [PDF – 3.8 MB]. Accessed August 9, 2010.
- Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality of end-of-life care: A national study. J Am Geriatr Soc 55(2):189–94. 2007.
- Troyer JL, McAuley WJ. Environmental contexts of ultimate decisions: Why white nursing home residents are twice as likely as African American residents to have an advance directive. J Gerontol B Psychol Sci Soc Sci 61(4):S194–S202. 2006.
- Resnick HE, Schuur JD, Heineman J, Stone R, Weissman JS. Advance directives in nursing home residents aged ≥ 65 years: United States 2004. Am J Hosp Palliat Care. Sage Publications DOI 10.1177/1049909108322295:1–7 (online). 2008.
- Bergman-Evans B, Kuhnel L, McNitt D, Myers S. Uncovering beliefs and barriers: Staff attitudes related to advance directives. Am J Hosp Palliat Care 25(5):347–53. 2008.
- Ramsaroop SD, Reid MC, Adelman RD. Completing an advance directive in the primary care setting: What do we need for success? J Am Geriatr Soc 55(2):277–83. 2007.
- Johnson KS, Kuchibhatla M, Tulsky JA. What explains racial differences in the use of advance directives and attitudes toward hospice care? J Am Geriatr Soc 56(10):1953–8. 2008.
- Ott BB. Views of African American nursing home residents and living wills. Geriatr Nurs 29(2):117–24. 2008.
- Sabatino C. Advance directives and advance care planning: Legal and policy issues. Report prepared for the U.S. Department of Health and Human Services; Assistant Secretary for Planning and Evaluation; Office of Disability, Aging and Long-Term Care Policy: Washington, DC. 2007.
- Wilkinson A, Wenger N, Shugarman LR. Literature review on advance directives. Report prepared for the U.S. Department of Health and Human Services; Assistant Secretary for Planning and Evaluation; Office of Disability, Aging and Long-Term Care Policy: Washington, DC. 2007.
- Kirschner KL. When written advance directives are not enough. Clin Geriatr Med 21(1):193–209. 2005.
Suggested citation
Jones AL, Moss AJ, Harris-Kojetin LD. Use of advance directives in long-term care populations. NCHS data brief, no 54. Hyattsville, MD: National Center for Health Statistics. 2011.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Jane E. Sisk, Ph.D., Director