
Construction Laborer Electrocuted After Accessing Primary Side of Transformer Box
DATE: April 22, 1994
MN FACE Investigation 93MN07901
SUMMARY
A 27-year-old male construction laborer (victim) was electrocuted when he made direct contact with an 8000-volt conductor inside a transformer box. He was not using any personal protective equipment at the time of the incident. He and a coworker were laying plastic conduit for underground cables beneath and up to the bottom of the box. An employee from the local electrical utility company had unlocked the box’s outer metal cover earlier so the construction workers could open it and visually monitor conduit positioning by way of its uncovered, secondary, 240-volt, side. Its primary, 8000-volt, side was double covered with an unlocked red fiberglass hood. After unlocking the box, the utility company employee left the site and instructed the workers not to access the primary side of the box. As the victim and coworker attempted to place the 90-degree elbow piece beneath the box’s primary side, it entered the box and got hung-up on a ground wire. The victim opened the fiberglass hood covering the primary side and reached inside to move the wire or conduit. As he withdrew his hand, he made direct contact with the 8000-volt conductor inside the transformer box, completed a path to ground, and was electrocuted. MN FACE investigators concluded that, in order to prevent similar occurrences, employers should
- ensure that energized components inside transformer boxes are inaccessible to unqualified employees; and
- provide employees with adequate training to ensure that they can recognize potential hazardous exposures.
INTRODUCTION
MN FACE was notified of a November 30, 1993 work-related electrocution of a construction laborer on the same day as the incident. MN OSHA and the county coroner were contacted and releasable information was taken. A police report of the incident was obtained. The victim’s employer and the safety director of the electrical utility company were interviewed. Photos taken by the utility company of the site and box were provided to MN FACE during the course of the investigation. A site investigation was conducted on December 9, 1993 with assistance from a National Institute for Occupational Safety and Health, Division of Safety Research investigator.
The victim worked as a laborer for a construction company contracted by a local electrical utility company to lay new plastic conduit for underground cables beneath transformer boxes. The construction company had performed this type work for the utility company for the past 15 years. The victim had worked in the construction industry for six to seven years, the last three in his present position. He had been provided verbal instruction and on-the-job training by his current employer.
INVESTIGATION
A 27-year-old male construction laborer (victim) was electrocuted while he and a coworker were installing a 4-inch diameter plastic (PVC) conduit for underground cables beneath a transformer box. They had upgraded several boxes at an apartment complex in the same manner, and were about one hour from job completion on the last box; it was located just outside of one of the apartment buildings. They had been working on site for about five weeks.
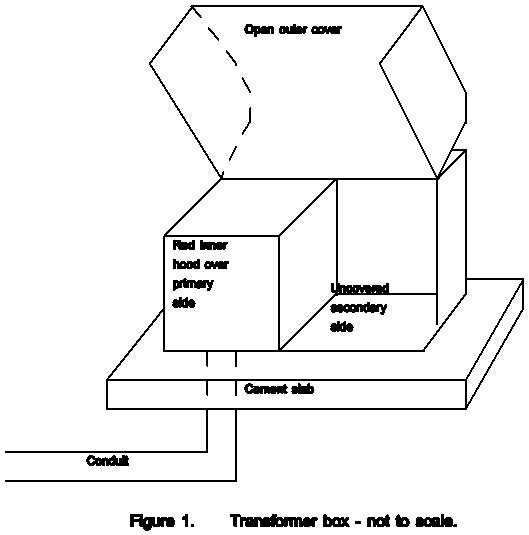
The 22-year-old transformer box, about 3-feet square, sat on top of an 8- to 10-inch thick cement slab. The slab was open directly beneath the box for running underground cables into it. A locked outer metal box covered both the transformer’s primary (8000-volt) side and its secondary (120-240-volt) side. Its primary side was, in addition, double covered with an unlocked inner fiberglass hood. The inner hood was red and had a yellow warning label attached which read “Warning-high voltage-operate hood with hot stick.” The inner hood completely enclosed the primary side of the box but did not extend over the box’s secondary side. See Figure 1.
The transformer’s outer metal cover was normally locked with a padlock. During conduit installation, however, it was unlocked by the utility company so the construction workers could open it and visually monitor conduit positioning by way of its uncovered secondary side. Construction workers were not to access any energized components inside the box during monitoring. The utility company’s policy required that their employee remain at a construction site until work was complete if a transformer was not double covered. If a transformer was double covered, their employee was free to leave a site after unlocking the box, provided that the inner fiberglass hood was left in place. Construction workers on site were then responsible for relocking the outer cover after work was complete.
On the day of the incident, a utility company employee unlocked the box and departed after reminding the construction workers that the fiberglass hood should not be opened. The workers excavated a trench for laying conduit up to the box with a back hoe, continued it under the cement slab by hand, and installation proceeded. As the victim and coworker attempted to place the 90-degree elbow piece beneath and up to the bottom of the box as specified by the utility company, it entered the box and got hung up on a ground wire. The victim, at the box, and his coworker, in the trench, could not dislodge the conduit. The victim lifted the inner hood and reached inside to move the wire or conduit. He was kneeling on the ground, supporting himself on the box’s outer cover with his left hand as he reached inside the inner hood with his right hand. As he withdrew his hand, he made direct contact with the angle bar connecting the 8000-volt primary conductor to the transformer, completed a path to ground, and was electrocuted. An exit wound was later found on his left hand.
His coworker pushed him away from the box and ran to a nearby apartment to tell its occupant to call 911. He then returned to the site and began CPR on the victim. A police officer arrived about six minutes later; the victim had no pulse and was not breathing at this time. An ambulance crew, arriving about the same time, continued resuscitation efforts. The victim was transported to a hospital where he was later pronounced dead.
CAUSE OF DEATH
The cause of death reported by the county coroner was electrocution.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Ensure that energized components inside transformer boxes are inaccessible to unqualified employees. This recommendation is in accordance with CFR 1926.403(j)(2)(i).
Discussion: The victim of this incident was not qualified to access energized components inside the transformer box. Under these or similar conditions, employers should ensure that energized components are strictly inaccessible to unqualified workers and/or enforce rules prohibiting access without the presence of a qualified person.
Recommendation #2: Provide employees with adequate training to ensure that they can recognize potential hazardous exposures. This recommendation is in accordance with CFR 1926.21(b)(2).
Discussion: OSHA Standard 1926.21 (b)(2) states that “the employer shall instruct each employee in the recognition and avoidance of unsafe conditions and the regulations applicable to his work environment to control or eliminate any hazards or other exposure to illness or injury.” Employers should provide employees with adequate training to ensure that they can recognize potential hazardous exposures. When new company procedures or guidelines are developed or existing ones modified, employers should ensure that workers are provided with appropriate supplemental training.
REFERENCES
- Office of the Federal Register, Code of Federal Regulations, Labor, 29 CFR Part 1926.21(b)(2) and 1926.403(j)(2)(i), U.S. Department of Labor, Occupational Safety and Health Administration, Washington, D.C., July 1, 1992.
- NIOSH – Division of Safety Research, FACE Report 90-31, Laborer dies from electrical injuries sustained in an electrical distribution system substation in Virginia. Morgantown, West Virginia, August 29, 1994.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.