
Volunteer Fire Chief Dies After Being Crushed Between Two Fire Trucks - Kansas
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2010-07 Date Released: August 23, 2010
Executive Summary
On February 10, 2010, a 69-year-old male Fire Chief (the victim) died after being crushed between a parked tanker and a pumper being backed into the fire station. The fire fighter reported that he observed the Fire Chief outside of the station as he was backing the pumper into the station. The fire fighter then realized he had backed the pumper too close to the tanker parked inside of the station, pulled forward to reposition the pumper, and then finished backing it into the station. The fire fighter exited the pumper and yelled for the Chief. The Chief did not respond. When the fire fighter searched for the Chief he found him unconscious and unresponsive on the station floor next to the pump panel of the tanker. The fire fighter called 911 and started CPR on the Chief. Emergency medical services responded and the Chief was pronounced dead by the coroner at the scene.

|
|
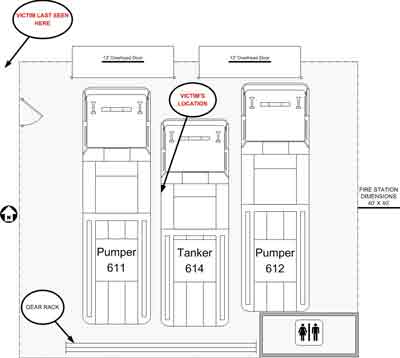
Position of the apparatus involved in this incident. |
Contributing Factors
- Inadequate policies for backing apparatus.
- Inadequate facility space for the number of apparatus.
- Inoperative backup warning system and possibly obscured side view mirror.
Key Recommendations
- Ensure that standard operating procedures are developed, implemented, and enforced on safe backing of fire apparatus and include adequate training to ensure fire fighter comprehension.
- Ensure that apparatus storage bays are well lit and have adequate room to store apparatus.
- Implement procedures for inspection, use, and maintenance of safety equipment used to assist in the backing of fire apparatus to ensure the equipment functions properly when needed.
- Ensure that fire apparatus drivers have unobstructed views from their rear view mirrors.
- Consider replacing fire apparatus more than 25 years old.
- Be aware of programs that provide assistance in obtaining alternate funding for replacing or purchasing fire apparatus and equipment and for facility modification.

|
|
Driver’s view of apparatus bay through passenger side rear-view mirror. Note vent window frame obstructing view. |
Introduction
On February 10, 2010, a 69-year-old male volunteer Fire Chief (the victim) died after being crushed between two fire trucks as a truck backed into the fire station. On March 5–7, 2010, a Safety and Occupational Health Specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated this incident. The NIOSH investigator met with the new Fire Chief, officers of the fire department, the fire fighter who backed the pumper into the station and the victim’s wife. The investigator met with the town police officer and spoke with the local coroner and the investigating officer from the Kansas State Police. The NIOSH investigator reviewed the State Police investigative findings, witness statements, and preliminary investigative report.
The NIOSH investigator reviewed training records of the Chief and the fire fighter (driver of the apparatus) and fire department records and visited the incident scene. The NIOSH investigator also spoke with the director of the Kansas Fire & Rescue Training Institute.
Fire Department
The department involved in this incident was a volunteer fire department consisting of two stations, with two pumpers and one tanker in the main station (incident site) and two brush trucks housed at an auxiliary station. The department had 14 members serving a population of approximately 900 residents in a geographical area of about 6 square miles and responded to approximately 83 incidents annually.
The fire department did not have any formal standard operating procedures for driving or operating fire apparatus. The department lacked a program for the regular inspection of the apparatus, and no formal records (e.g., check-off sheets, driver logs) were kept on any of the apparatus.
Training and Experience
The victim had been with this department for more than 14 years, all of which were served as the Chief. The driver of the apparatus involved in this incident had been a volunteer fire fighter with this department for 8 years, and in October 2008 he attended and received credit for a 24-hour driver/operator class administered by the Kansas Fire & Rescue Training Institute.1 The fire fighter also held a commercial driver’s license and was considered to be a qualified driver of all apparatus assigned to the department. No other formal training records were available for either the Chief or the fire fighter.
Although the state of Kansas does not require minimum fire fighter training, the state does encourage and offer training through the Kansas Fire & Rescue Training Institute under a “mobile fire academy” philosophy in which they provide training to fire departments in their local communities. The Kansas Fire & Rescue Training Institute reported that most of this training (including Fire Fighter 1, 2 and driver/operator classes) is offered at no cost to the fire departments.
Equipment
The apparatus involved in this incident was a 1977, 750-gallon-per-minute commercial pumper (see Photo 1). In 1994, the fire department purchased this pumper as a used vehicle from another department, and the pumper was in service with this department from 1994 until after this incident. The gross vehicle weight rating of the pumper was 27,500 lbs. The pumper had a manual transmission, gasoline engine, and two axles with six wheels (two in the front and four in the rear). The pumper had an audible reverse warning device and lights, which were found by the state police investigators to be not operating after the incident. The right side rear view mirror was rigidly mounted and a frame for the vent window possibly caused a partial obstruction to the driver’s view (see Photo 2 and Photo 3). Note: The department hired a private firm to inspect the apparatus after this incident and corrosion problems were found on the main frame rails. After the inspection, the apparatus was removed from service permanently.

|
|
Photo 1. Pumper involved in this incident is on the right. |
Timeline
The timeline for this incident includes approximate times obtained from witness interviews and time recordings from the dispatch report, police report, and the coroner.
- 1502 Hours
Department is alerted to send a tanker to assist with a mutual aid structure fire. The Chief (victim) picks up a fire fighter at the fire fighter’s house, and they respond to the station in the Chief’s private vehicle. - 1512 Hours
Chief pulls Pumper 611 out of fire station, and the fire fighter pulls Tanker 614 out of the station and responds to the incident by himself. Chief remains at the fire station. - 1519 Hours
Tanker 614 is canceled by dispatch and directed to return to the fire station. - 1532 Hours
Tanker 614 arrives back at the fire station. The fire fighter observes the Chief pull Pumper 611 out of the fire station, and then the fire fighter backed Tanker 614 into the middle of the fire station. The fire fighter then got out of Tanker 614 and walked over to Pumper 611, got in on the driver’s side, and proceeded to back Pumper 611 into the station. The fire fighter then realized he had backed the pumper too close to the tanker parked inside of the station, pulled forward to reposition the pumper, and then finished backing it into the station. The fire fighter stated during interviews that he observed the Chief (line of sight) standing outside the station next to the man door (see Diagram) and that there were no verbal communications between the two. - 1543 Hours
Dispatch pages out emergency incident for an unresponsive fire fighter trapped between two fire trucks. - 1548 Hours
Police en route. - 1551 Hours
Police on scene and report by radio that CPR is in progress. - 1607 Hours
Advance life support (ALS) ambulance on scene. - 1609 Hours
Air ambulance helicopter landing zone is established. - 1616 Hours
Second ALS ambulance arrives on scene. - 1620 Hours
Air ambulance helicopter canceled. - 1622 Hours
Police request Kansas State Patrol to respond. - 1625 Hours
Chief pronounced dead by coroner. - 1635 Hours
Chief placed in back of ambulance. - 1920 Hours
Coroner cleared scene.
Weather
The weather on the day of the incident was clear and sunny with an approximate temperature of 37°F and light winds out of the west at 1.3 miles per hour.2 This incident occurred at approximately 1543 hours. The fire fighter driving the pumper stated the sun light was causing glare and a reduction in his ability to see into the fire station.
Investigation
On February 10, 2010, at approximately 1543 hours, a volunteer Fire Chief (the victim) was crushed between two fire trucks while one of the trucks was being backed into the fire station. The Chief died from his injuries at the scene.
The Chief and a fire fighter had traveled to the fire station to respond with a tanker truck to a mutual aid incident. The Chief and the fire fighter arrived at the station, and the Chief pulled Pumper 611 out of the way to allow the fire fighter to pull Tanker 614 out of the station. The Chief then backed Pumper 611 back into the station. Note: Two pumpers and one tanker occupied the two-bay station (see Diagram); one of the pumpers had to be moved to access and remove the tanker, which was stored between the two pumpers. The Chief and the fire fighter were the only department personnel that responded to the mutual aid call.
The fire fighter responded to the mutual aid call with Tanker 614. Shortly after leaving the station, the response was canceled and Tanker 614 was directed to return to the station. The fire fighter stated during interviews that when he returned to the station he observed the Chief get into Pumper 611 and pull it out of the station. The fire fighter backed Tanker 614 into the station, then walked over to Pumper 611 and got into the driver’s seat to back it into the station. The fire fighter told the NIOSH investigator that he had trouble seeing the inside of the station bay due to poor lighting and glare from the sun. The fire fighter stated that when he was backing Pumper 611 into the station he observed, by line of sight, the Chief standing outside the station next to a man door (see Diagram). The fire fighter realized that he was too close to Tanker 614 (parked in the middle of the two station bays), and he pulled the pumper forward to straighten up and then backed into the station. He did not have a spotter helping him to back in, and there was no verbal communication between the Chief and himself. He then got out of Pumper 611 and came around the front of the truck and yelled for the Chief. He did not get a response. He then walked between Pumper 611 and Tanker 614 and found the Chief lying on the bay floor beside the pump panel of Tanker 614, unresponsive (see Photo 2 ). The fire fighter called 911 and started CPR on the victim.

|
|
|
Diagram. Layout of the incident scene. |
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatalities:
- Inadequate policies for backing apparatus.
- Inadequate facility space for the number of apparatus.
- Inoperative backup warning system and possibly obscured side view mirror.
Cause of Death
According to the coroner, the victim died from blunt force trauma.
Recommendations
Recommendation #1: Fire departments should ensure that standard operating procedures are developed, implemented, and enforced on safe backing of fire apparatus and include adequate training to ensure fire fighter comprehension.
Discussion: The National Fire Protection Association (NFPA) 1500 Standard on Fire Department Occupational Safety and Health Program states, “The fire department shall develop standard operating procedures for safely driving fire apparatus during nonemergency travel and emergency response and shall include specific criteria for vehicle speed, crossing intersections, traversing railroad grade crossings, the use of emergency warning devices, and backing of fire apparatus.”3 A standard operating procedure (SOP) on backing fire apparatus should include driver responsibilities (i.e., mirror adjustment and safe path of travel) and the use of a spotter(s). Backing a fire apparatus is a challenge regardless of the conditions and should be avoided whenever possible. If backing is unavoidable, then spotters should be used to safely direct the operation from outside the vehicle. The spotter(s) should discuss a backing plan (consistent with the SOP) with the driver and agree on the communication or warning process prior to beginning. At least one crew member, preferably two crew members, should be positioned to assist a driver during backing operations. A spotter should be positioned at the rear of the fire apparatus on either the driver’s or officer’s side so that they are visible in the side-view mirrors. If more than one spotter is available, one can be positioned at the rear of the fire apparatus and one at the front or both can be positioned at the rear, on either side of the apparatus. The use of more than one spotter will assist the driver in negotiating tight spaces such as alleyways. The SOP should state that members assigned to assist in backing apparatus should be in communication with the driver/operator through the use of department-approved hand signals, one-on-one communication, an intercom system, or two-way radio devices. To avoid confusion when more than one spotter is used, it is important to designate only one spotter to communicate with the driver.
Drivers need to make sure they maintain visual contact with the spotter(s) and immediately stop backing when visual contact is lost. Backing should only be resumed when visual contact is reestablished and the designated spotter gives appropriate direction to continue (spotter(s) should make sure they can see the driver in the mirrors). It is important that the driver focuses on backing, is not distracted by dispatch traffic, and is not using a cell phone or handheld radio communication device while engaged in backing maneuvers. When spotters are assisting with backing a fire truck they need to stay visible within the designated side-view mirrors, stay away from the driver’s blind spots, stay clear of the fire truck’s path of travel, avoid walking backwards, and signal the driver to stop when a person or object comes within the truck’s path of travel or when the spotter needs to change positions.4,5 Fire apparatus could be equipped or retrofitted with additional mirrors, commercially available video cameras, or sensing devices. This would help to alleviate some of the risk involved with backing operations; however, these devices cannot take the place of spotters, who are not riding on the apparatus, but assisting and directing the driver while backing.6
Fire departments should ensure their members are thoroughly trained on the SOPs and programs that are developed for backing fire apparatus. The United States Fire Administration’s (USFA) manual, Safe Operation of Fire Tankers, states, “One of the most common types of crashes that can be traced to failure to follow SOPs is those that involve backing the apparatus.”7 The National Fire Protection Association (NFPA) 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications8 provides minimum job performance requirements (JPR) for career and volunteer fire fighters who drive and operate fire apparatus. Each JPR consists of the task to be performed; the tools, equipment, or materials that must be provided to successfully complete the task; evaluation parameters and/or performance outcomes; and list of requisite knowledge and skills one must have to be able to perform the task. Fire departments should ensure that fire apparatus driver /operator training programs meet the minimum requirements described in NFPA 1002 and that personnel are provided opportunities for continuing education.
In this incident, the Chief and the fire fighter had no communication regarding backing responsibilities, and the driver did not know the victim was going to go behind or between the trucks. The Chief was last seen by the fire fighter standing by the main door outside the station (see Diagram), and his intentions were unknown to the fire fighter. The fire department did not have any formal standard operating procedures or policies for driving or operating fire apparatus at the time of the incident, but has since instituted a backing policy.
Recommendation #2: Fire departments should ensure that apparatus storage bays are well lit and have adequate room to store apparatus.
Discussion: Many older fire stations were designed to hold less apparatus than they currently hold. To store larger and greater numbers of fire apparatus in these fire stations requires proper planning, not only to ensure adequate space for the apparatus, but to ensure the safety of the personnel having to walk around and between these vehicles. The station bays also need to be well lit so the apparatus drivers can sufficiently see inside the bay when backing a vehicle in from the outside.
In this incident, the fire station was a two-bay station designed to accommodate two pieces of fire apparatus. The department added a third piece of apparatus to the bay area, which required squeezing the tanker between the two pumpers. This resulted in limited room between the trucks and very little space for a spotter or backer to work safely. The fire fighter had to maneuver the apparatus on an angle to fit into the space (see Photo 1 and Photo 2). The fire fighter stated that he had trouble seeing the inside of the station bay due to poor lighting and glare from the sun..
Recommendation #3: Fire departments should implement proper procedures for inspection, use, and maintenance of safety equipment used to assist in the backing of fire apparatus to ensure the equipment functions properly when needed.
Discussion: NFPA 1500 Standard on Fire Department Occupational Safety and Health Program section 6.4.1 states, “All fire apparatus shall be inspected at least weekly, within 24 hours after any use or repair, and prior to being placed in service or used for emergency purposes, in order to identify and correct unsafe conditions.”3 Written policies and procedures should incorporate a preventative maintenance program that will provide information on proper inspection, maintenance, and repair of apparatus and its equipment. This program should also provide guidance for documenting, notifying, filing, and securing maintenance checks and records, including requirements to place an apparatus out of service. Also, all operating and maintenance instructions and manuals shall be provided and maintained for those performing routine tests, inspections, and servicing functions.9
After the incident, the Kansas State Police inspected the involved apparatus and found that its audible warning alarm and reverse lights were not working. The department lacked a program for the regular inspection of the apparatus, and no formal records (e.g., check-off sheets, driver logs) were kept on any of the apparatus. It is possible that the victim did not see or hear the truck repositioning after the first backing attempt and for an unknown reason walked between the two trucks. If the audible warning device had been operating, the victim may have heard the backup alarm or seen the lights and moved out of the way.
Recommendation #4: Fire departments should ensure that fire apparatus drivers have unobstructed views from their rear view mirrors.
The proper combination of seat adjustment and mirror placement and mirror adjustment are important to provide the driver of the apparatus an unobstructed view of the outside rear view mirrors while all passengers are in their seated positions. The 2009 edition of NFPA 1901 Standard for Automotive Fire Apparatus10 states, “The passenger side mirror shall be so mounted that the driver has a clear view of the mirror when the passengers are in their normal seated positions.”
In this incident, the driver’s view of the passenger side rear view mirror was possibly obstructed by a window vent frame. The mirror was a fixed mounted assembly and may not have allowed adequate adjustment to alleviate the obstruction due to its age (see Photo 3).

|
|
Photo 3. Driver’s view of apparatus bay through officer’s side rear-view mirror. Note vent window frame obstructing view. |
Recommendation #5: Fire departments should consider replacing fire apparatus more than 25 years old.
Discussion: To maximize fire fighter safety as well as the safety of the traveling public, it is important that fire apparatus be equipped with the latest safety features and operating capabilities. In the last 15 to 20 years, much progress has been made in upgrading the safety features and capabilities of fire apparatus. Significant improvements in fire apparatus safety have been the standard since 1991, and fire departments should consider the value (or risk) to fire fighters of keeping pre-1991 fire apparatus in first-line service. Apparatus manufactured prior to 1991 usually conformed to only a few of the safety standards for fire apparatus set by the NFPA.11 The length of a vehicle’s life depends on many factors, including mileage and engine hours, quality of the preventive maintenance program, quality of the driver training program, whether the fire apparatus was used within the design parameters, whether the apparatus was manufactured on a custom or commercial chassis, quality of workmanship by the original manufacturer, quality of the components used, and the availability of replacement parts, to name a few.11
Fire departments should consider upgrading older fire apparatus in accordance with NFPA 1912, Standard for Fire Apparatus Refurbishing, latest edition,12 and retire or replace older apparatus in accordance with current standards such as NFPA 1911, Standard for the Inspection, Maintenance, Testing, and Retirement of In-service Automotive Fire Apparatus11. Fire departments should also consider retiring apparatus sooner if the apparatus becomes obsolete or unreliable due to age or use.
In this incident the truck was over 25 years old and had the original mirrors that were not adjustable by the driver. The drivers view of the passenger side rear view mirror was possibly obscured by the window vent frame (see Photo 3). The audible and visual back-up alarms were not operational at the time of the incident. After the incident the fire department hired a private firm to inspect the apparatus and corrosion problems were found on the main frame rails. After the inspection, the apparatus was removed from service permanently.
Recommendation #6: Fire departments should be aware of programs that provide assistance in obtaining alternative funding for replacing or purchasing fire apparatus and equipment and for facility modification.
Discussion: While it is important that fire departments seek constant improvements and upgrades to their fire apparatus, equipment, and facilities, some departments may not have the resources or programs to replace or upgrade as often as they should. Alternative funding sources, such as federal grants, are available to purchase fire apparatus, equipment, and facilities. Additionally, there are organizations that can assist fire departments in researching, requesting, and writing grant applications. The following is a list of useful resources:
Federal Emergency Management Agency (FEMA), Assistance to Firefighters Grant (AFG) Programexternal icon
www.firegrantsupport.com
FEMA grants are awarded to fire departments to enhance their ability to protect the public and fire service personnel from fire and related hazards. This Web site offers resources to help fire departments prepare and submit grant requests. The primary goal of the Assistance to Fire Fighters Grant (AFG) Program is to provide critically needed resources such as emergency vehicles and apparatus, equipment, protective gear, training for responders, and other needs to help fire departments protect the public and emergency workers from fire and related hazards. The Grant Programs Directorate of FEMA administers the grants in cooperation with the United States Fire Administration.
National Fire Protection Association (NFPA), Safer Act Grantexternal icon
www.nfpa.org/codes-and-standards/standards-development-process/safer-act-grant NFPA provides excerpts from NFPA 1710 and NFPA 1720 and other online resources to assist fire departments with the grant application process. (Link updated 8/13/2013)
National Volunteer Fire Council (NVFC), Grants & Fundingexternal icon
www.nvfc.org/hot-topics/grants-and-funding (Link Updated 1/28/2013)
The NVFC provides an online resource center to assist departments applying for SAFER grants, including narratives from successful past grant applications and a listing of federal grant and funding opportunities.
FireGrantsHelp.comexternal icon
www.firegrantshelp.com
A nongovernmental group, FireGrantsHelp.com provides an extensive database of information on federal, state, local, and corporate grant opportunities for first responders.
References
- Kansas Fire & Rescue Training Instituteexternal icon, 1515 St. Andrews Drive, Lawrence, KS 60647-1619. http://kufire.ku.edu/ Date Accessed: June 15, 2010. (Link updated 8/12/2013)
- Weather Underground [2010]. Weather history for Kansas, February 10, 2010external icon [http://www.wunderground.com/weatherstation/WXDailyHistory.asp?ID=KMOAMSTE2&month=2&day=10&year=2010]. Date Accessed: April 17, 2010.
- NFPA [2007]. NFPA 1500 Standard on fire department occupational safety and health program. 2007 ed. Quincy, MA: National Fire Protection Association.
- NIOSH [1994]. NIOSH alert: preventing worker injuries and deaths from moving refuse collection vehicles. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 97-110 [https://www.cdc.gov/Niosh/docs/97-110/]. (Link updated 5/13/2015)
- NIOSH [2009]. Career fire fighter dies when backed over while spotting an apparatus – New Jersey. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2009-10. https://www.cdc.gov/niosh/fire/reports/face200910.html.
- NIOSH [2005]. Career fire fighter dies after falling from tailboard and being backed over by engine – California. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2005-01. https://www.cdc.gov/niosh/fire/reports/face200501.html.
- USFA/FEMA [2003]. Safe operation of fire tankers.pdf iconexternal icon Emmitsburg, MD: U.S. Fire Administration, Publication No. FA 248 [http://www.iaff.org/hs/evsp/usfa%20safe%20operation%20of%20fire%20tankers.pdf].
- NFPA [2009]. NFPA 1002 Standard for fire apparatus driver/operator professional qualifications. 2009 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1451 Standard for a fire service vehicle operations training program. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2009]. NFPA 1901 Standard for automotive fire apparatus. 2009 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1911 Standard for the inspection, maintenance, testing, and retirement of in-service automotive fire apparatus. 2007 ed. Annex D guidelines for first-line and reserve apparatus. Quincy, MA: National Fire Protection Association.
- NFPA [2006]. NFPA 1912 Standard for fire apparatus refurbishing. 2006 ed. Quincy, MA: National Fire Protection Association.
Investigator Information
This investigation was conducted by Stephen T. Miles, Safety and Occupational Health Specialist with the Fire Fighter Fatality Investigation and Prevention Program, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. This report was authored by Stephen T. Miles. A technical review was provided by Deputy Fire Chief William Goldfeder of the Loveland-Symmes (OH) Fire Department and editor of FireFighterCloseCalls.comexternal icon, and Division Chief W. Edward Buchanan of the Hanover (Virginia) Fire and EMS Department. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
|
The National Institute for Occupational Safety and Health (NIOSH) initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim.
|
For further information, visit the program Web site at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
This page was last updated on 09/09/2010.