
Career Fire Fighter Dies in Fall from Roof at Apartment Building Fire - New York
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2007-19 Date Released: June 11, 2009
SUMMARY
On June 21, 2007, a 23-year-old male career fire fighter (the victim) died after falling from the roof at a four-story apartment building fire. When fire fighters arrived on scene, light smoke and fire was showing from a 4th floor window. The victim had just climbed the truck ladder to the roof bulkhead and was attempting to lower himself to the main roof when he fell. The roof saw (slung on the victim’s back) shifted causing the victim to lose his balance and fall to the ground. Fire fighters had been on scene less than 3 minutes when the victim fell. The victim was transported to a metropolitan hospital where he succumbed to his injuries. Key contributing factors to this incident include: judgment of the fire fighter in deciding on a riskier means of moving from the roof bulkhead to the main roof, the placement of the ladder against the roof bulkhead rather than the main roof which introduced additional fall risks for fire fighters, the hazardous task of climbing a ladder while laden with tools and equipment, and the method in which the saw was carried which allowed the shifting saw to put the fire fighter off balance.
NIOSH has concluded that, to minimize the risk of similar occurrences, fire departments should:
- stress to fire fighters the importance of exercising caution when working at elevation
- consider the location and placement of aerial ladders to prevent fire fighters from climbing from different elevations during fireground operations
- consider the use of portable scissor ladders to facilitate access from an aerial ladder to the roof
- ensure that fire fighters communicate any potential hazards to one another and ensure that team continuity is maintained during roof operations
- evaluate the manner in which equipment is harnessed or carried by fire fighters to prevent loss of balance
- consider reducing the amount of equipment that fire fighters must carry while climbing ladders
Manufacturers of fire service saws should:
- consider ergonomic design principles to reduce the weight of ventilation saws
- consider developing improved carrying slings
INTRODUCTION
On June 21, 2007, a 23-year-old male career fire fighter was fatally injured when he fell from the roof during a fire at a four- story apartment building. On June 25, 2007, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On July 24-26, 2007, a safety and occupational health specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated this incident. The NIOSH investigator met with officials of the fire department and with representatives from the Uniformed Fire Officers Association (UFOA) and the Uniformed Firefighters Association (UFA) which are affiliated with the International Association of Fire Fighters (IAFF). The investigator reviewed witness statements of fire fighters and officers involved in the incident, examined photographs and video of the fireground, and reviewed the victim’s training records and death certificate. The NIOSH investigator also reviewed the department’s fireground standard operating procedures (SOPs)1 and listened to the dispatch tape of this incident. The incident site was visited, measured, and photographed.
FIRE DEPARTMENT
The fire department involved in this incident consists of approximately 11,500 career fire fighters that serve a population of over eight million in a geographic area of approximately 322 square miles.
TRAINING and EXPERIENCE
The State of New York requires that fire departments train career fire fighters to a level equivalent to National Fire Protection Association (NFPA) Level II. The state also requires 100 hours of annual in-service training.
The fire department requires all fire fighters to complete a 23-week training program at the department’s fire academy. (Note: At the time the victim graduated from the academy the program was 13 weeks). Fire fighter recruits are instructed in the basics of fire suppression systems and fire fighting tactics. After graduating from the fire academy, the recruits go through a one year probationary period.
The victim graduated from the department’s fire academy in September 2005 and had almost two years of fire fighting experience with a truck company.
EQUIPMENT and PERSONNEL
There were 5 apparatus and 30 fire fighters dispatched to the fire. The 911 call was received at 1654 hours and fire fighters were dispatched at 1655 hours. Response listed in order of arrival included:
- 1657 hours
- Engine 216 (officer and 4 fire fighters)
Ladder 108 (officer and 5 fire fighters)
- Engine 216 (officer and 4 fire fighters)
- 1658 hours
- Engine 229 (officer and 4 fire fighters)
Ladder 146 (officer, the victim, and 4 fire fighters)
- Engine 229 (officer and 4 fire fighters)
- 1659 hours
- Battalion Chief 35 (Incident Commander) and battalion fire fighter
Engine 230 (officer and 5 fire fighters)
- Battalion Chief 35 (Incident Commander) and battalion fire fighter
PERSONAL PROTECTIVE EQUIPMENT
At the time of the incident, the victim was wearing the full array of personal protective clothing and equipment, consisting of turnout gear (coat and pants), helmet, Nomex® hood, gloves, boots, and a self-contained breathing apparatus (SCBA) with an integrated personal alert safety system (PASS). The victim was carrying a Halligan hook, a Halligan bar, and a gasoline-powered roof saw in a harness slung over his shoulder in bandolier fashion. The victim was also equipped with a portable radio, flashlight, safety harness and personal safety rope. This equipment weighs approximately 110 pounds.
STRUCTURE
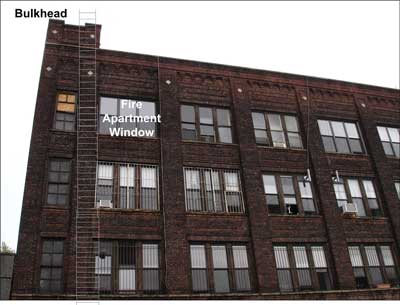
The structure involved in this incident was a four-story industrial brick building of class III construction, originally built in the 1920s (see Photo 1). The building was originally a sewing machine factory and had been illegally converted into residential loft apartments in 2000. The building was 75 feet wide by 100 feet long and was equipped with sprinklers, some of which were blocked because of the illegal conversions. Each floor had four apartments and interior construction was drywall over metal studs. Exterior construction was solid brick with a flat tar and asphalt roof. The building had two internal stairwells, one of which was blocked on every floor, with bulkheads on the roof at diagonal corners.
According to the fire department, the cause and origin of the fire was an unattended cigarette left on a 4th floor window sill that ignited the wooden window frame. The fire was confined to the window sill and adjacent interior furnishings, but the plumes of smoke made the blaze appear larger than it actually was. Some of the occupants of the apartment building had already evacuated as fire department apparatus arrived on scene.
WEATHER
The weather at the time of the incident was clear with a temperature of 79°F and an average wind speed of 9 mph from the west. The weather was not a factor in this incident.
INVESTIGATION
On June 21, 2007, at approximately 1654 hours, a fire was reported on the 4th floor of a 4-story apartment building. On arrival, fire fighters saw fire and moderate white smoke in a window on the top floor of the apartment building.
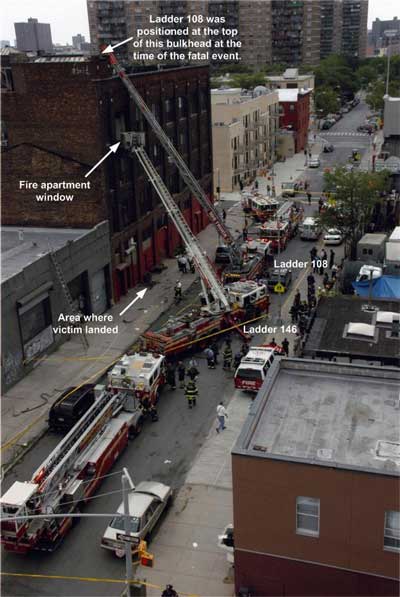
Ladder 108 (L108), the 1st due truck company, arrived at 1657 hours. After positioning in front of the building, the L108 roof fire fighter raised and placed the aerial ladder to the roof at the center of the bulk head (see Photo 2). (Note: A roof fire fighter is responsible for ventilating the roof if necessary and checking all sides of a building for trapped residents). The victim (another roof fire fighter) arrived on scene in Ladder 146 at 1658 hours. He dismounted the apparatus, grabbed his tools and went to Ladder 108 to access the roof.
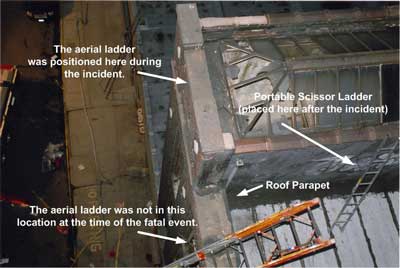
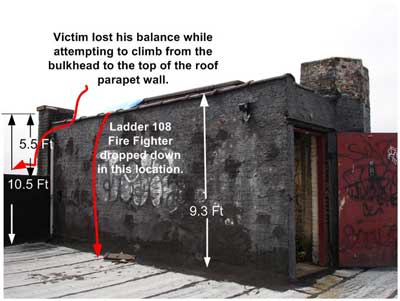
The L108 roof fire fighter climbed the ladder to the roof with the victim climbing about 20 feet behind. He threw his Haligan bar and hook to the roof when he reached the level of the roof while still on the aerial ladder. The L108 roof fire fighter dismounted the aerial ladder onto the top of the bulkhead; he squatted between the bulkhead parapet and the skylight (see Photo 3). He vented some of the glass panes in the bulkhead skylight and observed very light smoke. He maneuvered to a safe area and lowered himself onto the roof by hanging and dropping (see Photo 4). (Note: From the top of the bulkhead to the roof was approximately 9 feet). He called to the victim, still climbing up the ladder that he may need to bring the folding scissor ladder on the tip of the aerial to access the roof from the bulkhead. He proceeded to the opposite side of the roof to provide vertical ventilation, looked over, opened the other bulkhead door, and then heard a scream followed by a MayDay radio transmission.
At 1701 hours, the victim fell approximately 60 feet to the ground while attempting to maneuver down from the top of the bulkhead to the top of the main roof parapet wall. He continued to hold a hand tool in each hand. (Note: It was 5’6” feet from the top of the bulkhead coping to the top of the roof parapet wall). The chauffeur of Ladder 108 observed that the roof saw (slung over the victim’s shoulder) shifted during the climb down from the bulkhead and the victim lost his balance. The victim fell to the ground and landed on his side and upper torso and sustained massive trauma to his head, torso, and extremities. (Note: Besides the weight shift from the saw, a loss of grip or footing could have contributed to the fall).
During this time, fire fighters from the 1st due engine company (Engine 216) were stretching a 2½ inch hose line to the 4th floor fire apartment. Fire fighters from the 2nd due engine company (Engine 229) were assisting with the hose line stretch. (Note: Since this was formerly an industrial building, departmental SOPs mandate a 2½ inch hose line). Fire fighters from the 3rd due engine company (Engine 230) also assisted with the stretch from Engine 216. The building’s sprinkler system was containing the spread of the fire and the hose line was not charged until after the fatal event.
Immediately after the victim fell, a fire fighter from Ladder 108 radioed a MayDay and rushed to aid the victim. Most of the members of Engine 230 saw the victim fall. Fire fighters on the ground immediately administered first aid/CPR/stabilization and rushed the victim to an awaiting ambulance. The victim was transported to a metropolitan hospital where he succumbed to his injuries.
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:
- judgment of the fire fighter in deciding on a riskier means of moving from the roof bulkhead to the main roof,
- the placement of the ladder against the roof bulkhead rather than the main roof which introduced additional fall risks for fire fighters,
- the hazardous task of climbing a ladder while laden with tools and equipment, and
- the method in which the saw was carried which allowed the shifting saw to put the fire fighter off balance.
CAUSE OF DEATH
According to the medical examiner’s findings, the cause of death was “blunt impact of head, torso and extremity with fractures and visceral injuries.”
RECOMMENDATIONS
Recommendation #1: Fire departments should stress to fire fighters the importance of exercising caution when working at elevation.
Discussion: Ascending and descending ground or aerial truck ladders are a common occurrence on the fireground.2 Ground and aerial ladders are used for fire fighting activities like roof access, window and fire escape rescues, ventilation, and fire suppression.3, 4 Fire fighters are expected to be in full structural fire fighting gear and carry needed equipment and tools while climbing ladders.5 This causes a safety concern when trying to maintain three-point contact on a ladder while climbing with tools.6 (Note: 3-point contact means you have 2 hands and 1 foot or 1 hand and 2 feet in contact with the ladder at all times). During this incident, the victim was exposed to a four-story fall. He ascended the aerial ladder with required structural fire fighting gear and equipment/tools. Once exiting the tip of the aerial ladder, he was on top of a bulkhead that was over nine feet above the roof line. He made a decision to try and lower himself to the roof instead of climbing down and repositioning the ladder.
Recommendation #2: Fire departments should consider location and placement of aerial ladders to prevent fire fighters from climbing from different elevations during fireground operations.
Discussion: Basic aerial ladder placement on the fireground is determined by the incident commander or ladder company officer.2 Proper ladder placement can be written into departmental SOPs. These SOPs should stress awareness of items like overhead structures, loose and irregular terrain, ground obstructions, and soft ground.2 The ladder operator should also pay close attention to the proper placement to achieve maximum stability and correct ladder climbing angle, which can be met by following manufacturer’s recommendations.2,7 During ventilation operations, a ladder may need to be placed to access the roof of the building. The ladder should be extended at least 6 feet above the roof line.4 During this incident, the aerial ladder was placed against a bulkhead parapet wall instead of the roof parapet. This may have been done to avoid placing the ladder too close to the window on fire. The bulkhead parapet wall was 5.5 feet higher than the roof parapet thus exposing fire fighters to a fall risk while descending to the roof. While both locations posed a fall risk while climbing down to the roof, it would have been preferable to locate the aerial ladder at the roof parapet rather than the bulkhead.
Recommendation #3: Fire departments should consider the use of portable scissor ladders to facilitate access from an aerial ladder to a roof.
Discussion: During this incident, the aerial ladder was initially placed at a bulkhead on the roof. This bulkhead measured approximately 9 feet above the roof. The first fire fighter lowered himself over the side of the bulkhead and then dropped to the roof without incident. The second fire fighter (the victim) attempted to lower himself to the adjacent roof parapet wall 5.5 feet below and fell to his death. The aerial apparatus had a portable scissor ladder mounted at the tip of the aerial. Using the portable scissor ladder in this incident would have been safer. It is recommended that these portable ladders be used to assist in the transition from an aerial ladder to a roof, especially when the distance to the roof is 5 feet or more.2, 4
Recommendation #4: Fire departments should ensure that fire fighters communicate any potential hazards to one another and ensure that team continuity is maintained during roof operations.
Discussion: Team continuity involves knowing who is on the team and who is the team leader; staying within visual contact at all times; communicating personal needs and observations to the team leader; rotating to rehab and staging as a team; and watching out for other team members.3 Following these basic rules helps prevent serious injury and death by providing personnel with the added safety net of fellow team members. Teams that enter a hazardous environment together should leave together to ensure that team continuity is maintained.8 During this incident, two fire fighters ascended an aerial ladder to perform roof operations. The first fire fighter arrived and exited the tip of the aerial ladder onto the roof’s bulkhead. He lowered himself down from the top of the bulkhead and went to the opposite side of the roof, breaking visual and voice contact with the victim. Fire fighters should communicate potential hazards to their crew, ladder operator, and the incident commander.
Recommendation #5: Fire departments should evaluate the manner in which equipment is harnessed or carried by fire fighters to prevent loss of balance.
Discussion: This fire department uses a strap/sling made from a section of nylon webbing.1 This allows for a roof saw to be carried over the fire fighter’s gear to permit the use of both hands while climbing a ladder (see Photo 5). This practice is taught at their fire academy.1 Their training included proper attachment of a 50 inch sling to each end of the saw and donning of it.1 While the victim was trying to descend to the roof parapet from the bulkhead his roof saw shifted, throwing him off balance, causing him to fall. In lieu of having fire fighters sling the saw over their body, they could possibly hoist it up to the roof with rope or if an aerial ladder has attachments for securing tools at the tip, these attachments could be used to elevate the tools for roof operations.
Recommendation #6: Fire departments should consider reducing the amount of equipment that fire fighters must carry while climbing ladders.
Discussion: Fire departments determine what equipment will be carried and utilized on the fireground by means of SOPs. The equipment needed by one fire fighter for roof operations can weigh as much as 110 pounds.1 This consists of basic structural fire fighting gear (i.e., helmet, turnout gear, gloves, boots and SCBA), Halligan hook, Halligan bar, rescue rope, roof saw, and a portable radio. After being equipped with all of this gear, the fire fighter may have to climb a ground or aerial ladder to perform roof operations.2 The weight and bulk of the structural gear and tools may cause a hazard on ladders when trying to maintain three-point contact.6 The weight of the gear causes extra stress on the body while climbing the ladder and even on the fireground. Fire departments should consider alternative ways to get essential fire fighting equipment to the roof of a structure to perform roof operations. Aerial platform trucks provide an enclosed platform basket for fire fighters to stand with their equipment.4 The platform truck will elevate them to the roof line without imposing additional physical stress on the fire fighter. Alternatively, the platform truck could be used to elevate the equipment to the roof line for fire fighters to retrieve.
Recommendation #7: Manufacturers of fire service saws should consider ergonomic design principles to reduce the weight of ventilation saws.
Discussion: Everyday fire fighters encounter hazardous and unknown conditions. They are required to wear protective gear and carry equipment and tools needed to do their life-saving tasks.3,9 One of the contributing factors in this incident was the shifting of a ventilation saw that was worn over the shoulder of the victim with a sling. In addition to the weight of structural fire fighting gear and other necessary tools carried by the victim, the roof saw weighted an extra 23 pounds. Manufacturers of ventilation saws currently used by the fire service should consider applying ergonomic principles to reduce the weight and size of these tools. Using a compact, lightweight roof saw would reduce the physical loading to fire fighters.
Recommendation #8: Manufacturers of fire service saws should consider developing improved carrying slings.
Discussion: During this incident, a ventilation saw was outfitted by the fire department with an aftermarket carrying sling/waist strap harness. It was placed in the same manner as the manufacturers’, but served a dual purpose as a carrying sling and safety harness while cutting. It was observed that while the victim was climbing down from the bulkhead, the saw shifted, throwing him off balance. Manufacturers should consider working with the fire service to develop different sized slings for variations in saw size and fire fighter stature. The goal is to keep the saw as close to the body as possible, thus limiting movement which can effect a fire fighter’s balance.
REFERENCES
- Fire Department [2007]. Standard operating procedures.
- Mittendorf, J [1998]. Truck company operations. Saddle Brook, NJ: Fire Engineering Books and Videos.
- International Fire Service Training Association [1998]. Essentials of fire fighting. 4th ed. Stillwater, OK: Oklahoma State University, Fire Protection Publications.
- International Fire Service Training Association [2000]. Aerial apparatus driver/operator handbook. 1st ed. Stillwater, OK: International Fire Service Training Association.
- NFPA [2007]. NFPA 1500, Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
- CPWR [2005]. Fact Sheet #4, don’t fall for it! Climbing ladders safely. Washington. DC: Center to Protect Workers’ Rights. [http://www.cpwr.com/pdfs/Sheet%204.pdf] (Link no longer available 10/28/2013)
- NFPA [2003]. NFPA 1002, Standard on fire apparatus driver/operator professional qualification. Quincy, MA: National Fire Protection Association.
- National Fire Academy Alumni Association [2000]. Firefighter’s handbook: essentials of firefighting and emergency response. Albany, NY: Delmar.
- NFPA [2007]. NFPA 1971, Standard on protective ensembles for structural fire fighting and proximity fire fighting. Quincy, MA: National Fire Protection Association.
INVESTIGATOR INFORMATION
This investigation was conducted by CDR Steve Berardinelli, Safety and Occupational Health Specialist with the Fire Fighter Fatality Investigation and Prevention Program, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. Stacy Wertman, Safety and Occupational Health Specialist with the Fire Fighter Fatality Investigation and Prevention Program assisted in the preparation of this report. Technical reviews were provided by Dr. Thomas Bobick, PhD, PE, CSP, CPE, Research Safety Engineer, Protective Technology Branch, Division of Safety Research, NIOSH and Deputy Chief Colleen Walz, Pittsburgh Bureau of Fire.
photos and Diagrams

|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit the program website at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 06/11/09.