
Career Fire Fighter Drowns While Conducting Training Dive - New Hampshire
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2004-36 Date Released: July 13, 2005
SUMMARY
On March 11, 2004, a 43-year–old male career fire fighter drowned while training for fire department dive rescue operations. The victim was diving with another dive rescue team member in a large, partially ice-covered lake when, after his partner lost visual track of him, the victim failed to surface. The dive partner notified authorities through a pedestrian and a commercial dock attendant while he continued searching from the land docks and parking area. Multiple governmental agencies and private commercial divers conducted an organized search for the missing diver, but the victim’s body was not found or recovered until the next day. He was pronounced dead on-scene.
NIOSH Investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
- ensure that an experienced backup diver, a safety boat, extra air tanks, and a medical unit is on the scene of all training dives
- ensure that Standard Operating Guidelines (SOG’s) establish and enforce separate but parallel diver training guidelines along with emergency rescue diving guidelines
INTRODUCTION
On March 11, 2004, a 43-year-old male career firefighter drowned while training with another fire department dive rescue team member. The National Institute for Occupational Safety and Health (NIOSH) was notified of this incident on March 15, 2004 by the U.S. Fire Administration (USFA). On August 20, 2004, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated the incident. The NIOSH team met with the Chief of the department and interviewed the victim’s diving partner. The NIOSH team then visited the site of the fatality with the diving partner and the Chief. A representative from the New Hampshire Marine Patrol also met the team at the site. The diving partner pointed out relevant landmarks and the approximate location where the victim’s body was found. NIOSH reviewed the State of New Hampshire Department of Safety Marine Patrol investigation report, the fire department’s Underwater Response Team Standard Operating Guidelines (SOGs), a copy of the victim’s dive log and training records, the dry suit user’s manual, the Chief Medical Examiner’s Report and the Certificate of Death. The State of New Hampshire Department of Safety Marine Patrol maintained possession of the diving suit and gear worn by the victim. An evaluation of the dry suit was conducted by the U.S. Navy Experimental Diving Unit located in Panama City, Florida at the request of the victim’s fire department.
Dive Equipment
Both divers were equipped with full self-contained underwater breathing apparatus (SCUBA) and new dry suits. They were also equipped with compasses, dive computers, a camera and other miscellaneous tools.
The State of New Hampshire Department of Safety Marine Patrol’s report concluded that there had been manufacturer-authorized trimming of the neck seal on the new dry suit. The outlet valve was found in a fully open position and there had been replacement of a factory one-hole inlet valve nipple with a two-hole inlet valve nipple. The two-hole inlet valve was not an authorized manufacturer recall replacement or retrofit. The report suggested that the neck seal may not have been trimmed to the proper size and could have led to a condition of carotid sinus reflex causing the victim to lose consciousness. The State report also speculated that an open outlet valve would have let air escape from the suit and would have allowed a condition of hypothermia. NIOSH was not able to examine the victim’s suit.
An evaluation of the dry suit was conducted by the U.S. Navy Experimental Diving Unit located in Panama City, Florida at the request of the victim’s fire department. The initial observations and findings listed in the report describe a dry suit that was clean, dry, and in good condition with no apparent damage and little wear. The latex neck seal had been trimmed to a circumference of approximately 12.75 inches. The latex wrist seals had also been trimmed. Both the inflation and deflation valves were clean and in good working order. The investigator, who was similar in size to the victim with the same neck circumference, donned the dry suit and found it to be tight. He noted that additional trimming of the neck seal would have been necessary to provide a comfortable fit. The Navy evaluator did not feel that the two-hole inlet valve was a contributing factor in this incident.
Weather
The sky was clear and sunny, the winds were calm and the air temperature was approximately 28 degrees Fahrenheit at the time of the incident.
Dive Site
The dive site was located at a lake with a rocky shoreline and bottom, little vegetation in the shallow regions, and flood controlled by a dam. The lake is at an elevation of 504 feet above sea level, is approximately 44,590 acres in size and has a shoreline of about 180 miles. The lake has a mean depth of 43 feet and a maximum depth of 180 feet. The water temperature at the time of the incident was approximately 35 degrees Fahrenheit, with water visibility reported to be about 15 feet.
Fire Department
The career department involved in this incident consists of 28 uniformed fire fighters serving a population of about 17,000 in a geographical area of about 26 square miles. The geographical area contains about 44 miles of the lake shoreline.
Training
The victim had 17 years of fire fighting experience with this fire department. The victim had 22 years of diver training and diving experience. He also had extensive diver rescue training, with certifications including the International Rescue Instructors Association, Professional Association of Diving Instructors (PADI) Ice Diver, PADI Dry Suit Diver, National Association of Underwater Instructors (NAUI) Master Scuba Diver and Fathom Diver, Scuba Diving International Public Safety Diver and Rescue Diver.
INVESTIGATION
On March 11, 2004, at approximately 1200 hours, the victim and his dive partner went on a dive rescue training exercise in a local lake. They both had completed a 24 hour work shift at 0700 hours. The purpose of the dive was to continue practicing with their newer dry suits. They had previously worn their dry suits at least eight times in other drills including dry land and swimming pool exercises. The fire fighter divers notified the Chief about their diving plans via telephone. The divers also requested and received permission from the local commercial cruise operator of the dock area about conducting their training near the dock.
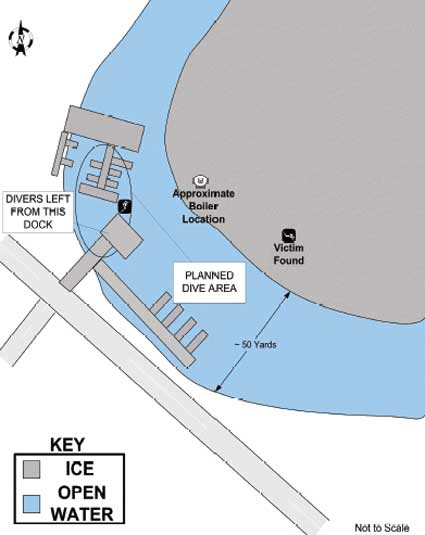
The two divers performed a mutual equipment check and discussed a basic route plan that included a compass heading. The victim was using a borrowed mask as he had experienced problems with his seal on a previous dive, the day before. He left his own mask on the edge of the dock in case he needed to use it later. The divers’ general plan was to stay in open water along the docks to observe the area around the pier pilings for hazards (Diagram). They specifically decided to stay away from the iced over area of the lake which was prevalent to about 50 feet away from the docks. Two large water circulators, which helped control ice build-up around the docks from the piers, were effective and running at the time of the incident.
At approximately 1400 hours, the victim entered the shallow (approximately 12 feet) water first and surfaced without problems. The dive partner entered next and also surfaced without problems. They proceeded to follow the dock piers north along the shoreline and were under the water for about 20 minutes when the victim went in a Southeast direction where he found what the partner described to investigators as an abandoned boiler. The dive partner took a posed picture of the victim next to the boiler.
Shortly after the picture was taken, the partner lost visual track of the victim. He looked for the victim in all directions, but thinking that he may have returned to the dock area to get the other mask, the partner proceeded to another location underwater. When he surfaced he still did not see the victim and looked for surface bubbles to indicate his location. No bubbles were visible. He also looked for wet areas near the dock where the victim may have exited the water, but the area was completely dry. Realizing his dive partner may have been experiencing problems, he proceeded to call for the victim and notified a passing pedestrian that he needed help with a missing diver and requested that she call 911. He then went directly to a commercial cruise employee to inform her of the situation and also requested that she also call 911. He then walked over to the parking area to see if the victim had returned to the parked vehicle while he continued to scan the lake for surface bubbles.
Engine 5 was dispatched and arrived on the scene at 1442 hours. The victim’s dive partner had about 1100 pounds of air left in his SCUBA tank. The engine crew tethered him with a rope to do a sweep search under the ice. There were no extra SCUBA air bottles or any other certified divers on scene at the time of the initial search.
Ultimately, it is estimated that there were 128 personnel from multiple government agencies and a local dive shop involved in the search. The Chief of the Department acted as the incident commander for the duration of the search. The victim’s body was found the following day at about 1250 hours. He was found almost 300 feet to the east from where he and his dive partner originally entered the water. The victim was at the bottom of the lake in about 20 feet of ice-covered water. All of the victim’s equipment was in place except for the regulator which was not in his mouth. He was pronounced dead on scene. It was later determined that his SCUBA tank was empty of air and the exhaust valve on his suit was in a fully open position.
Cause of Death
The death certificate listed the cause of death as drowning.
RECOMMENDATIONS/DISCUSSIONS
Recommendation #1: Fire departments should ensure that an experienced backup diver, a safety boat, extra air tanks, and a medical unit is on the scene of all training dives.
Discussion: A backup diver may be critically important in the case of a diving emergency, since they can provide a fresh, outside source of rescue.1, 2 In addition, personnel on the shore should be able to monitor communication among divers both above and below water through an electronic surface monitor. In this incident, a backup diver could have been instrumental in the attempted rescue. A safety boat could provide a critical and mobile landing for an emergency situation, and transport of additional personnel to the search location. A medic unit on scene or within a very short response time and dedicated to the training could provide oxygen and other critical medical aid and transport for emergency situations.1, 2
Recommendation #2: Fire departments should ensure that Standard Operating Guidelines (SOG’s) establish and enforce separate but parallel diver training guidelines along with emergency rescue diving guidelines.
Discussion: Fire departments should treat training dives with the same oversight as their standard general operating guidelines for emergency rescue diving, but specifically outline the unique safety needs for training dives.
In this situation, the fire department had well developed guidelines for dive rescue team membership and emergency procedures, but didn’t specifically address training operations as either the same or different than the guidelines. The department SOG’s required the training officer to ensure that all training exercises were conducted in accordance with the established guidelines, but these could create a situation that allows unclear procedures or lessened safety standards for training dives as opposed to emergency rescue dive situations. Well conceived SOG’s would ensure that there is positive communications between dive partners and the surface. The SOG’s should also outline the use of a backup diver and a ninety-percent-ready diver who are in position and ready to help for both training and rescue dives.1 For example, the fire department’s SOG’s included the use of an incident commander, a safety officer, team leader, and other positions that may not be needed, or may have different titles, on ancillary training dives. The SOG’s should include specific requirements to maintain team integrity through the “buddy system” on all dives, and designated position titles could be combined but still designated for all training dives.
REFERENCES
- NIOSH [2004]. NIOSH Workplace Solutions: Divers Beware: Training Dives Present Serious Hazards to Fire Fighters. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 2004-152.
- Hendrick W, Zaferes A, Nelson C [2000]. Public safety diving. Saddle Brook, NJ: Fire Engineering Books and Videos.Additional resources regarding SCUBA diving include the following:
NFPA 1670—Standard on operations and training for technical rescue incidents.
NFPA 1006—Standard for rescue technician professional qualifications.
PADI [1990]. PADI open water diver manual. Santa Ana, CA: Professional Association of Diving Instructors.
NAUI [2000]. NAUI SCUBA diver manual. Tampa, FL: National Association of Underwater Instructors.
INVESTIGATOR INFORMATION
This incident was investigated by Bruce Oerter and Mark McFall, Safety and Occupational Health Specialists with the Fatality Investigation Team of the Division of Safety Research, NIOSH.
Diagram
|
|
Diagram. Aerial view of dive area.
|
This page was last updated on 07/13/05.