
Residential Fire Claims the Lives of Two Volunteer Fire Fighters and Seriously Injures an Assistant Chief - Missouri
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2001-15 Date Released: November 23, 2001
SUMMARY
On March 18, 2001, two volunteer fire fighters, a 36-year-old male lieutenant (Victim #1) and a 39-year-old male fire fighter (Victim #2) died, and an Assistant Chief was injured while trying to exit the first floor of a private residence after a partial collapse of the second floor. At approximately 0025 hours, Central Dispatch received a call from the owner of the residence stating that the upstairs was on fire. Central Dispatch immediately notified the volunteer department of the incident. The Assistant Police Chief was the first to arrive on the scene and noticed smoke venting from the second floor roof on both the east and west sides of the structure. At 0029 hours, the Assistant Police Chief confirmed that all occupants were out of the house and proceeded with traffic control. Engine 78 arrived on the scene at 0033 hours with an Engine Operator (Victim #1) and was positioned to the north side of the structure. The Assistant Chief arrived on the scene at 0041 hours and shortly thereafter entered the structure to man the nozzle of a 1½-inch handline already inside from an initial assessment conducted by Victim #1 and a fire fighter. Victim #1 and Victim #2 entered the structure just after the Assistant Chief to provide backup for an aggressive fire search and interior suppression. Both the Assistant Chief and Victim #2 became low on air. The Assistant Chief instructed Victim #1 to lead Victim #2 out of the structure by following the hoseline. The Assistant Chief continued to fight the fire while the two victims attempted to exit. The two victims left the area together, but apparently became disoriented from a partial collapse of the second floor and ended up in the laundry room. When the Assistant Chief tried to exit, it is believed that he was knocked down in the living room by part of the second-floor collapse. Crew members on the scene were able to pull the Assistant Chief from the structure, but the intensity of the fire and the lack of backup self-contained breathing apparatus (SCBAs) hindered additional rescue attempts. The mutual-aid departments were able to get the fire under control for the removal of the two victims at approximately 0146 hours. Both victims were found on the floor of the laundry room at the east end of the hallway. They were removed from the structure by a mutual-aid company and later pronounced dead at the hospital. NIOSH investigators concluded that to minimize the risk of similar occurrences, fire departments should
- ensure that an adequate number of staff are available to immediately respond to emergency incidents
- ensure that Incident Command conducts a complete size-up of the incident before initiating fire-fighting efforts, and continually evaluates the risk versus gain during operations at the incident
- ensure that officers enforce and fire fighters wear their SCBAs whenever there is a chance they might be exposed to a toxic or oxygen deficient atmosphere, including the initial assessment
- ensure consistent use of personal alert safety system (PASS) devices at all incidents and consider providing fire fighters with a PASS integrated into their self-contained breathing apparatus which provides for automatic activation
- ensure vertical ventilation takes place to release any heat, smoke, and fire
- ensure supervisors remain accountable for all who operate under their supervision and ensure that a team continuity of at least two fire fighters is maintained
- provide adequate on-scene communications including fireground tactical channels
- implement an emergency notification system to rapidly warn all persons who might be in danger if an imminent hazard is identified or if a change in strategy is made
- ensure that adequate personal protective equipment is available while fire fighters are engaged in fire activity
- develop and implement a preventative maintenance program to ensure that all self- contained breathing apparatus (SCBAs) are adequately maintained

Incident Site
INTRODUCTION
On March 18, 2001, two volunteer fire fighters, Victim #1 (36-year-old male Lieutenant) and Victim #2, (39-year-old male fire fighter) died and an Assistant Chief was injured during an interior fire attack at a local residence. The Assistant Chief and the two victims agreed to exit the structure when the Assistant Chief’s and Victim #2’s low-air alarms sounded. The Assistant Chief continued to fight the fire as the two victims attempted to follow the hoseline outside. As the crew was exiting, a partial collapse of the second floor disoriented and trapped the two victims inside the structure. The Assistant Chief was knocked down in the living room approximately 3 feet from the exit and was pulled out by crew members. Mutual-aid departments were dispatched to the scene and located and removed the two victims at approximately 0146 hours. All three fire fighters were transported to the local hospital where the victims were pronounced dead. The Assistant Chief was treated for his injuries then flown to an area burn unit.
The National Institute for Occupational Safety and Health (NIOSH) was notified of this incident by the U.S. Fire Administration (USFA) on March 22, 2001. On April 26, 2001, a safety and occupational health specialist and the team leader from NIOSH’s Fire Fighter Fatality Investigation and Prevention Program investigated this incident. Meetings were conducted with the Chief, Assistant Chief, fire fighters, the Mayor, the Assistant Police Chief and the investigators for the State Fire Marshal’s Office. Interviews were conducted with the officers, fire fighters, and police officer involved in this incident. NIOSH investigators reviewed copies of photographs, structural drawings, and reports completed by the State Fire Marshal’s Office. The State Fire Marshal’s Office determined the cause to be electrical and listed the fire as accidental. A site visit was also conducted and the site photographed. The site was a single-family home consisting of a two-story structure in the front (north) with a single story attached on the back (south) side. The frame of the structure was constructed of wood studs with plaster lath on the interior and aluminum siding on the exterior. The roof was layered asphalt shingles over plywood sheeting.
The fire department involved in this incident consists of one fire station with a total of 27 volunteer fire fighters. The department serves a population of approximately 900 in a geographic area of 149 square miles.
The State of Missouri and the fire department do not require any specialized training for their fire fighters. The fire department provides training opportunities both in-house and through the University of Missouri at Columbia. Victim #1 had more than 2½ years of service and received the following training through the University of Missouri: fire cause determination, emergency vehicle response safety, clandestine drug labs, basic fire fighting foam, farm accident rescue, rural water supply, and fire cause determination. Victim #2 had more than 1 ½ years of service and received the following training through the University of Missouri: survival techniques in interior operations, killer in the attic, emergency control of natural gas and carbon monoxide response, electrical problems at emergency incidents, survival techniques in interior operations, vehicle fire-fighting strategy and tactics. The injured fire fighter had more than 7 years of service and received the following training through the University of Missouri: handling LP gas emergencies, introduction to the fire service, hazardous materials decontamination, auto rescue, personal protective equipment and breathing apparatus, fire cause determination, farm accident rescue, hose and firestream practices.
INVESTIGATION
On March 18, 2001, at approximately 0025 hours, Central Dispatch received a call from the owner of the residence stating that the upstairs was on fire. Central Dispatch immediately notified the volunteer department of the incident. The Assistant Police Chief was the first to arrive on the scene and noticed smoke venting from the second-floor roof on both the east and west sides of the structure. At 0029 hours, the Assistant Police Chief confirmed that all occupants were out of the house and proceeded with traffic control. At approximately 0033 hours Engine 78 arrived on the scene with an engine operator (Victim #1) and met a fire fighter who had just arrived in his privately owned vehicle (POV). Wearing turnouts but no self-contained breathing apparatus, they advanced a 1½-inch handline into the first floor of the structure to assess the fire situation. Upon entering, they encountered moderate smoke and a small amount of fire on the stairwell coming from the second floor, which they extinguished without a problem (see Diagram). After exiting, fire fighters reentered the structure with SCBAs in order to make an aggressive attack and extinguish the fire. The Safety Officer was on the scene at approximately 0034 and was coordinating the disconnection of the propane tank and electrical service with the available fire fighters and a representative from the local power company. The Chief and the Assistant Safety Officer arrived on the scene together at approximately 0035, and the Chief assumed Incident Command (IC). The IC began hooking the pumper to a hydrant with a 2½-inch line and the Assistant Safety Officer began operating the engine. Victim #2 arrived on the scene via POV at 0034 and met up with Victim #1 to locate the SCBAs for reentry into the structure. The Assistant Chief arrived on the scene at 0041 hours and prepared to enter the structure. Victim #1, Victim #2 and the Assistant Chief received assistance from the Assistant Safety Officer with locating and donning their SCBAs. The interior attack crew and the IC had radios but did not establish communications before or during entry. Note: Although seven firefighters were on the scene, only five SCBAs were available. During the time the Assistant Safety Officer was assisting the fire fighters with donning their SCBAs, it was determined that only three SCBAs were functioning properly. This eliminated any rescue attempts until additional units arrived.
The Assistant Chief entered first to locate and man the nozzle that was left inside the structure from the initial entry by Victim #1 and a fire fighter. Victim #1 and Victim #2 followed after donning their SCBAs. Visibility inside of the hallway deteriorated as they were advancing toward the stairwell. Note: While fighting the fire, the Assistant Chief noticed the only fire on the first floor was in a wall just off the hallway. He also noticed a ceiling fan had fallen through the hole at the top of this wall (see Diagram). At that time, the low air alarms sounded for the Assistant Chief and Victim #2. Through face-to-face contact, the Assistant Chief gave instructions for Victim #1 to lead Victim #2 out of the structure by following the hoseline, and upon exiting, to tug on the handline twice to indicate they had made it out safely. The Assistant Chief informed them that he would sit on the hose and keep the temperature down to assist with their exit. The Assistant Chief continued suppressing the fire for approximately 3 minutes but did not receive a tug on the handline. He shut the hose down and took it with him while he tried to exit. Note: It is believed that the second floor of the structure, previously damaged by fire, partially collapsed, disorienting the two victims and injuring the Assistant Chief. When he reached the door from the hallway into the living room, the Assistant Chief was knocked down from falling debris. While on his stomach, he threw his helmet at a figure he saw on the front porch. The crew members on the front porch saw the helmet, entered the structure, and were able to reach the Assistant Chief to pull him from the structure. The Chief requested mutual aid at 0055 hours, just before the victims became trapped. The mutual-aid departments arrived on the scene at 0124 hours and began to suppress the fire. They were able to gain control of the fire to reach and remove the victims by 0146 hours. Victim #1 and Victim #2 were unresponsive upon removal, and advanced life-saving procedures were initiated en route to the local hospital where the victims were pronounced dead on arrival. The Assistant Chief suffered second- and third-degree burns to his head, face, and hands.
CAUSE OF DEATH
The cause of death for both victims as listed by the medical examiner was asphyxiation due to smoke inhalation.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Fire departments should ensure that an adequate number of staff are available to immediately respond to emergency incidents.1
Discussion: As stated in NFPA 1500
(6-4.3) “Members operating in hazardous areas at emergency incidents shall operate in teams of two or more. Team members operating in hazardous areas shall be in communication with each other through visual, audible, or physical means or safety guide rope, in order to coordinate their activities. Team members shall be in close proximity to each other to provide assistance in case of emergency.”
(6-4.4) “In the initial stages of an incident where only one team is operating in the hazardous area at a working structural fire, a minimum of four individuals is required, consisting of two individuals working as a team in the hazard area and two individuals outside this hazard area for assistance or rescue at emergency operations where entry into the danger area is required. The staged members shall be responsible for maintaining a constant awareness of the number and identity of members operating in the hazardous area, their location and function, and time of entry. The standby members shall remain in radio, visual, voice, or signal line communications with the team.”
(6-4.4.2) “One standby member shall be permitted to perform other duties outside of the hazardous area, such as apparatus operator, incident commander, or technician or aide, provided constant communication is maintained between the standby member and the members of the team. The assignment of any personnel, including the incident commander, the safety officer, or operators of fire apparatus, shall not be permitted as standby personnel if by abandoning their critical task(s) to assist or, if necessary, perform rescue, they clearly jeopardize the safety and health of any fire fighter working at the incident. No one shall be permitted to serve as a standby member of the fire-fighting team when the other activities in which he/she is engaged inhibit his/her ability to assist in or perform rescue, if necessary, or are of such importance that they cannot be abandoned without placing other fire fighters in danger.”
Recommendation #2: Fire departments should ensure that Incident Command conducts a complete size-up of the incident before initiating fire fighting efforts, and continually evaluates the risk versus gain during operations at an incident.2-9
Discussion: One of the most important size-up duties of the first-in officers is locating the fire and determining its severity. This information lays the foundation for the entire operation. First, it determines the number of fire fighters and the amount of apparatus and equipment needed to control the fire. Second, it assists in determining the most effective point of fire extinguishment attack and the most effective method of venting heat and smoke.
A proper size-up begins from the moment the alarm is received, and it continues until the emergency is under control. Several factors must be evaluated in conducting the size-up-e.g., type of structure, time of day, contents of the structure, potential hazards, etc. The size-up should also include risk versus gain during incident operations.
The following general factors are important considerations:
Occupancy type involved. The type of occupancy can have a great effect on the aspects of the fire attack. The type of occupancy could assist in determining the structure’s layout, hazardous materials, previous fire damage and the possibility of civilians.
Smoke conditions. The smoke conditions can provide the Incident Commander with information to make ventilation and other tactical decisions when arriving on the scene. Smoke conditions will vary according to how the burning has progressed. The density of the smoke is in direct ratio to the amount of suspended particles. The smoke from a fire that is just beginning will not have as much density as the smoke from a fire that is fully developed. As burning progresses, the density will likely increase. This may make the smoke become darker due to the large quantities of carbon particles.
Type of construction. The type of construction will be one of the most important areas to identify. The type of structure could provide information such as how the building will hold up under fire conditions or if the building is generally subject to collapse under fire conditions.
Type of roof system. The roof system should be one of the first things that is determined before fire fighters enter a burning structure.
Age of structure. The Incident Commander should acknowledge the age of the building when determining strategy or tactics. The age of the structure can provide the Incident Commander with information to determine the building’s integrity or other areas previously mentioned.
Exposures. The Incident Commander should evaluate the whole picture. The protection of exposures near or connected to a burning building should be included in the strategic plan.
Time considerations. Information such as time of incident, time fire was burning before arrival, time fire was burning after arrival, and type of attack are some of the most important information the Incident Commander should have.
Upon arrival on the scene, an initial walk around of the structure should have been conducted to locate the seat of the fire, assess the degree of the involvement of the fire and hazards to fire fighters, and to identify where fire suppression activities should be initiated.
Additionally, fire departments should ensure that the first officer or fire fighter inside evaluates interior conditions and reports them immediately to the Incident Commander.
Interior conditions along with a past history of fire and its location within the structure could change the IC’s strategy or tactics. For example, if heavy smoke is emitting from the exterior roof system, but fire fighters cannot find any sizable fire in the interior, it is a good possibility that the fire is in a concealed space such as the floor joists or roofing system. It is important for the Incident Commander to immediately obtain this type of information to make the proper decisions.
Recommendation #3: Fire departments should ensure that officers enforce and fire fighters wear their SCBAs whenever there is a chance they might be exposed to a toxic or oxygen deficient atmosphere, including the initial assessment.1,2,10,11
Discussion: Far more fire deaths occur from carbon monoxide than from any other toxic product of combustion. This colorless, odorless gas is present in every fire. The poorer the ventilation and the more inefficient the burning, the greater the quantity of carbon monoxide formed. SCBAs should be worn while conducting the initial assessment inside a burning structure, not only to protect the fire fighters from a potential hazardous atmosphere, but to allow the fire spread, intensity, and location to be determined. This information gathered from the initial assessment is imperative so that the IC can utilize the proper procedures and tactics to control and extinguish the fire.
Recommendation #4: Fire departments should ensure consistent use of personal alert safety system (PASS) devices at all incidents and consider providing fire fighters with a PASS integrated into their self-contained breathing apparatus which provides for automatic activation.12
Discussion: PASS devices are electronic devices worn by the fire fighter, which will emit a loud and distinctive alarm if the fire fighter becomes motionless for more than 30 seconds. Fire fighters entering hazardous areas should be equipped with a PASS device. There are several types of PASS devices available. One device that could be used is a PASS that is integrated into the SCBA. “Such automatic activation shall be permitted to be, but not limited to, linked to activation of SCBA, linked to removal from storage or transportation positions, by pull-away tether to a fixed position, or by remote activation.” Manual PASS devices are also used throughout the fire service. These devices require fire fighters to manually turn on the device each time they use it.
Recommendation #5: Fire departments should ensure that vertical ventilation takes place to release any heat, smoke, and fire.2,3,13
Discussion: Ventilation is necessary to improve the fire environment for fire fighters to approach a fire with a hoseline for extinguishment. Additionally, smoke, heat, and gases should be vented above the fire to prohibit conditions necessary for a flashover. This should be completed as soon as possible. Vertical ventilation will delay heat buildup at the ceiling level of the burning room; it may also delay flashover long enough to allow a quick search for a victim, and it may assist in the advancement of an attack hoseline. Ventilation decisions should be a part of the initial size-up. If it is determined that ventilation cannot be completed because of unsafe areas or conditions (e.g., spongy roof, trusses exposed to fire, etc.), then fire fighters should not be exposed or operate under the unsafe areas or conditions.
Recommendation #6: Fire departments should ensure supervisors remain accountable for all who operate under their supervision and ensure that a team continuity of at least two fire fighters is maintained.2,14
Discussion: Each fire fighter should be assigned to a team of two or more and given specific assignments to help reduce the chance of injuries. Team continuity relies on some very important key factors: knowing who is on your team and the team leader, staying within visual contact at all times (if visibility is obscured then teams should remain within touch or voice distance of each other), communicating your needs and observations to the team leader, rotation to rehabilitation and staging as a team, and watching your team members (practice a strong “buddy-care” approach). These key factors help to reduce serious injury or even death resulting from the risks involved in fire fighting operations by providing personnel with the added safety net of fellow team members. The company or line officer should remain with his or her crew and provide the appropriate level of supervision. Fire fighters should enter and exit together and no fire fighter should operate alone.
Recommendation #7: Fire departments should provide adequate on-scene communications including fireground tactical channels.5,15,16
Discussion: Communication should be an ongoing component of on-scene operations. NFPA 1561 states that the communications system shall meet the requirements of the fire department for routine and large-scale emergencies. Emergency scenes become very hectic within a short period of time. Radio communications occurring between incident command, attack crews, pumper operators, mutual-aid companies, and dispatch can easily be missed. It is imperative that on-scene operations be given fireground tactical radio channels which are separate from the normal dispatch frequencies. Fire fighters operating on the scene must be capable of communicating between themselves and incident command without being “talked over” by dispatch or other companies. In a small fire department, one radio channel for dispatch and one fireground communications channel might be sufficient for most situations. A larger fire department requires several additional radio channels to provide for the volume of communications relating to routine incidents and for the complexity of multiple alarm situations. Interior attack crews should have adequate radio communication with Incident Command and with other attack crews to provide for personnel accountability, coordination of efforts, report on flame spread, fire extinguishment, and other pertinent information. As Incident Command becomes aware of changing conditions, vital information can be given directly to the attack crews. The radio capabilities should also provide for communications with mutual-aid resources or other agencies that could be expected to respond to a major incident. The system should be developed to provide reserve capacity for unusually complex situations where effective communications could become critical.
Recommendation #8: Fire departments should implement an emergency notification system to rapidly warn all persons who might be in danger if an imminent hazard is identified or if a change in strategy is made.3,16
Discussion: There is a difference between withdrawing fire fighters and calling for an emergency evacuation of fire fighters. A normal withdraw action is ordered when a fire is spreading beyond the ability of fire fighters’ control. An emergency evacuation is ordered when an extremely serious emergency has occurred or is about to happen, such as a missing fire fighter(s), explosion, or collapse. In an emergency evacuation, unlike a withdrawal, fire department tools and hoses are left behind and a roll call or a head count must be conducted as there may be a missing fire fighter. An emergency evacuation is a rare occurrence in the fire service, and because of its rarity, confusion and delay may occur when it is ordered. For this reason, there should be a prearranged signal, tone, or sound to alert fire fighters of an emergency withdraw; fire departments should train their members for an emergency evacuation upon receipt of the signal. Fire fighters should immediately exit the structure upon receipt of the prearranged signal, leaving behind tools and equipment, which can be removed later. If fire fighters are performing an interior attack with the possibility of a ceiling collapse and hear the prearranged tone or signal, they should attempt to exit immediately. If fire fighters are unable to exit, they should attempt to establish a collapse shelter. Incident Commanders should use the prearranged emergency evacuation signal or tone whenever they decide conditions are unsafe for interior fire fighting or an emergency has occurred with a fire fighter.
Recommendation #9: Fire departments should ensure adequate personal protective equipment is available while fire fighters are engaged in fire activity.1
Discussion: Sufficient SCBAs should be available at the incident to provide one unit for each member who might be exposed to respiratory hazards. Reserve cylinders or an on-scene refill capability should be available to provide a reserve air supply.
Recommendation #10: Fire departments should develop and implement a preventative maintenance program to ensure that all self-contained breathing apparatus (SCBAs) are adequately maintained.17
Discussion: Fire departments should establish respirator service and maintenance procedures and rigidly enforce them to provide respirators that are dependable and are constantly evaluated, tested, and maintained. Equally important is record keeping, a critical element of any respirator maintenance program.
REFERENCES
1. NFPA [1997]. NFPA 1500: Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
2. International Fire Service Training Association [1998]. Essentials of fire fighting 4th ed. Stillwater, OK: Fire Protection Publications.
3. Dunn V [1988]. Collapse of burning buildings, a guide to fireground safety. Saddle Brook, NJ: Fire Engineering Books and Videos.
4. NIOSH [1999]. NIOSH alert: request for assistance in preventing injuries and deaths of fire fighters due to structural collapse. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 99-146.
5. Dunn V [1992]. Safety and survival on the fireground. Saddle Brook, NJ: Fire Engineering Books & Videos
6. Kipp JD, Loflin ME [1996]. Emergency incident risk management: safety & health perspective. New York: Van Nostrand Reinhold Publishing.
7. Norman J [1998]. Fire officer’s handbook of tactics. Saddle Brook, NJ: Fire Engineering Books and Videos.
8. Dunn V [1996]. Systems analysis, size-up: Part 1. Firehouse, October Issue.
9. Brunacini A [1985]. Fire command. Quincy, MA:National Fire Protection Association.
10. Occupational Safety and Health (OSHA). February 1, 2000. 29 CFR 1910.134 (g),(4). Procedures for interior structural firefighting.
11. NFPA [1995]. NFPA 1404: Fire department self-contained breathing apparatus program. Quincy, MA: National Fire Protection Association.
12. NFPA [1998]. NFPA 1982, Personal Alert Safety System. Quincy, MA: National Fire Protection Association.
13. Brannigan FL [1999]. Building construction for the fire service. Quincy, MA: National Fire Protection Association
14. Fire Fighter’s Handbook [2000]. Essentials of fire fighting and emergency response. New York: Delmar Publishers.
15. Essentials of fire Fighting, 3rd ed, Fire Protection Publications, 1998. (Incident Command, Back Up Hose Crew, Rapid Intervention Team, Communications).
16. NFPA [1995]. NFPA 1561: Standard on fire department incident management system. Quincy, MA: National Fire Protection Association
17. NIOSH [1999]. Status investigation report of four self-contained breathing apparatus. NIOSH task No. TN-10856. Certification and Quality Assurance Branch, Division of Respiratory Disease Studies, NIOSH, Morgantown, WV.
INVESTIGATOR INFORMATION
This investigation was conducted by Jay L. Tarley, Safety and Occupational Health Specialist, and Richard W. Braddee, Team Leader, Fire Fighter Fatality Investigation and Prevention Program, Division of Safety Research, Surveillance and Field Investigations Branch, NIOSH.

Photo. West Side of Structure Involved in Incident
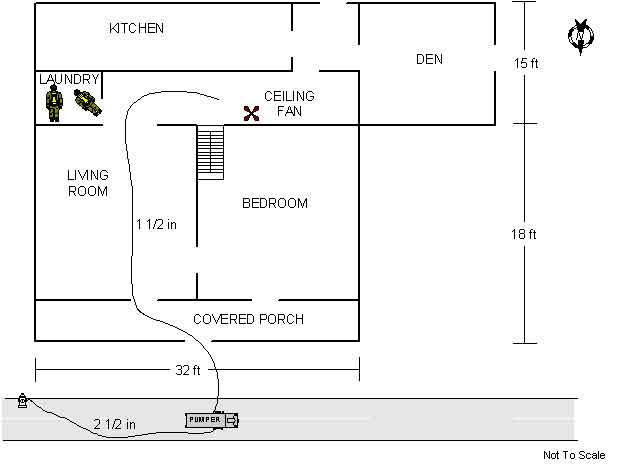
Diagram. Residential Floor Plan
This page was last updated on 1/10/02