
Career Fire Fighter Dies and Three Are Injured In a Residential Garage Fire - Utah
 Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty…A summary of a NIOSH fire fighter fatality investigation
F2000-23 Date Released: July 28, 2000
SUMMARY
On March 31, 2000, a 36-year-old male career fire fighter (the victim) died, and three other fire fighters were injured while fighting a residential garage fire. The fire fighters had responded to a call that had come in from Central Dispatch at 2200 hours. As Engine 1 approached the scene from the south, at 2207 hours, the Captain assumed Incident Command (IC) and conducted a quick size-up of the south, east, and north sides of the structure as Engine 1’s driver drove past and parked the apparatus just north of the scene. The IC reported to Central Dispatch smoke and flames showing at the garage window on the south side of the structure and smoke coming from around the edges of the closed garage door. The IC proceeded to the garage door where he kicked in one corner of the door while the two fire fighters from Engine 1 (victim and Fire Fighter #1) stood at the door with 200 feet of charged 1 3/4-inch hose line. They quickly knocked down most of the fire in the garage. Believing that the fire was knocked down, the IC instructed the victim and Fire Fighter #1 to enter the structure, go upstairs, search for any civilians who may be inside, and open some windows for ventilation. The victim and Fire Fighter #1 proceeded with their 1 3/4-inch hose line through the front door. The smoke just inside the front door was thick and black and was banked from the ceiling to just above floor level. The Lieutenant from Engine 2 (Lieutenant and two fire fighters), who had just arrived on the scene, was directed by the IC to follow the 1 3/4-inch line into the structure and provide assistance to the two fire fighters (victim and Fire Fighter #1) who had just entered the structure. The Lieutenant followed the hose line until he reached the two fire fighters upstairs at the end of the hall, in front of the master bedroom door. The Lieutenant noticed a glow at the end of the hall near the stairway and that the heat had dramatically increased. He then turned and sprayed water down the hall, hoping to knock down the heat. Unsuccessful at knocking down the heat, the Lieutenant, Fire Fighter #1, and the victim moved farther down the hall to try and escape the heat. The Lieutenant then decided that they had to exit by following the hose line back to the front door. Fire Fighter #1 came out the front door followed by the Lieutenant, who believed that the victim was following him, but the victim never came out. A Rapid Intervention Team (RIT) consisting of two fire fighters from Ambulance 1 were assembled and were able to enter through bedroom #2’s window (see Diagram 1, Photo 1, and Photo 2). At approximately 2239 hours, the RIT located the victim in the master bedroom and dragged him back through bedroom #2 and out the window to the fire fighters waiting on the garage roof and in the driveway. The victim was transported by ambulance to a nearby hospital where he was pronounced dead at 2317 hours. NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
- establish and implement written standard operating procedures (SOPs) regarding emergency operations on the fireground
- ensure that the Incident Command conducts a complete size-up of the incident before initiating fire fighting efforts, and continually evaluates the risk versus gain during operations at an incident
- ensure that fire fighters conducting a search above a fire take safety precautions to reduce the risk of being trapped
- ensure that a separate Incident Safety Officer (ISO), independent from the Incident Commander, is appointed
- ensure that Incident Command always maintains close accountability for all personnel at the fire scene
- ensure that a Rapid Intervention Team (RIT) stand by with equipment, ready to provide assistance or rescue
- consider providing fire fighters with a Personal Alert Safety System (PASS) integrated into their Self-Contained Breathing Apparatus (SCBA)
- ensure that the Incident Commander be clearly identified as the only individual responsible for the overall coordination and direction of all activities at an incident
- ensure that the Incident Commander maintains the role of director and does not become involved as a laborer

Incident Scene
INTRODUCTION
On March 31, 2000, one fire fighter (the victim) died and three fire fighters were injured at an incident involving a residential garage fire. The Incident Commander was one of the three injured fire fighters, and he sustained third-degree burns to his hands. The other two injured fire fighters had been with the victim when they received second- and third-degree burns to their hands. They also suffered from heat exhaustion. The victim became separated from the two fire fighters and died as a result of smoke inhalation.
The National Institute for Occupational Safety and Health (NIOSH) was notified of this incident by the U.S. Fire Administration (USFA) on April 3, 2000. On April 26, 2000, two Safety and Occupational Health Specialists and the Team Leader from NIOSH’s Fire Fighter Fatality Investigation and Prevention Program investigated this incident. Meetings were conducted with the Chief, Assistant Chief, and the Arson Investigator from the fire department involved in the incident and with the Chief of the fire department where the victim was a full-time fire fighter. Interviews were conducted with the IC, officers, and fire fighters involved in this incident. NIOSH investigators obtained from the Arson Investigator copies of photographs, structural drawings, and reports completed by the fire department’s Arson Investigator and the State Fire Marshal’s Office. The victim’s SCBA was sent to the NIOSH Respirator Branch in Morgantown, West Virginia, for testing. The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations (CFR), Part 84, Subpart H. Further testing was conducted to determine conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, 1997 Edition. A series of tests utilizing a Biosystems PosiChek3 computerized SCBA performance tester were also conducted. The SCBA met the requirements of all six NIOSH SCBA Certification tests performed. The SCBA also met the requirements of the NFPA Air Flow Performance Test and all tests performed using the Biosystems Posichek3 (a summary of this report is included as Appendix A). A site visit was also conducted. The site is a multi-level, single-family residential structure located in a subdivision. The structure has a poured-in-place concrete foundation with a half basement. The frame of the structure is constructed of wood studs with brick facing on the front and aluminum siding on the remainder of the exterior.
The fire department involved in this incident consists of three fire stations with a total of 66 employees, of which 64 are uniformed fire fighters (the victim was a paid, part-time fire fighter with this department). The department serves a population of approximately 62,500 in a geographic area of 25 square miles. The fire department requires all new fire fighters to receive International Fire Service Training Association fire training for Fire Fighter-1/Utah certification. Each fire fighter is also trained and certified as an Emergency Medical Technician (EMT). The victim’s training records were reviewed and were found to be sufficient. The victim was certified as Fire Fighter-1 and Fire Fighter-2, Utah apparatus driver, EMT, and EMT-IV. The victim had also received Utah Fire and Rescue Academy-Flashover training. The victim had 10 years of fire fighting experience (2 years prior to this department, and a combination of 8 years as a part-time fire fighter with this department and 2 years as a full-time fire fighter with a nearby department).
INVESTIGATION
On March 31, 2000, at 2200 hours, a call came into Central Dispatch reporting a garage fire at a residence. The units responding at 2200 hours included Engine 1 (Captain, Lieutenant [Engine/Operator [E/O]], and two fire fighters), Engine 2 (Lieutenant and two fire fighters), Engine 3 (fire fighter [Acting Officer], one E/O, and three fire fighters), Ambulance 3 (Lieutenant, and two fire fighters). Upon arriving on the scene at 2207 hours, the Captain from Engine 1 assumed Incident Command (IC). The IC conducted a quick size-up of the south, east, and north sides of the structure as Engine 1’s driver drove past and parked the apparatus just north of the scene. He reported to Central Dispatch smoke and flames showing at the garage window on the south side of the structure and smoke coming from around the edges of the closed garage door (see Diagram 2). Fire Fighter #1 and the victim pulled a 200-foot, 1 3/4-inch cross lay preconnect line from Engine 1. The IC then attempted to open the garage door, and while doing so received third-degree burns to his hands (he was wearing leather gloves), as burning gasoline ran down the driveway from underneath the garage door. The IC then proceeded to kick one corner of the garage door in while the two fire fighters (victim and Fire Fighter #1) stood ready at the door with charged hose line. They quickly knocked down most of the fire in the back of the garage (see Diagram 2) and moved back from the garage door and onto the front lawn. Engine 2 arrived on the scene at 2208 hours and staged approximately 50 feet behind Engine 1. The IC radioed Engine 2 to lay a 5-inch water supply line to Engine 1. At approximately 2210 hours, the IC directed the victim and Fire Fighter #1 to enter the structure, go upstairs, and conduct a search for any civilians who may be inside. Note: The IC was informed that the occupants had vacated the structure and were across the street at a neighbor’s house. The IC was also given conflicting reports from civilians in the area that people had gone back inside the building. It is the department’s policy to conduct a search of the building in case someone entered the building before the department’s arrival. The victim and Fire Fighter #1 were also instructed by the IC to open some windows to help ventilate the smoke from the structure. Believing that the fire was knocked down, the victim and Fire Fighter #1 proceeded with the 1 3/4-inch hose line through the open front door (see Diagram 1). At approximately 2211 hours, Engine 3, followed by Ambulance 3, arrived on the scene. The victim and Fire Fighter #1 had to crawl due to the heavy black smoke they encountered on the first level. Fire Fighter #1 was on the nozzle and was followed by the victim. They conducted a left-hand search and checked the closet near the main entrance. The closet was clear. They proceeded forward, up the stairs, and to the hallway on the second level. Continuing to do a left-hand search, the victim searched bedroom #1 and bedroom #2 while Fire Fighter #1 manned the nozzle in the hallway (see Diagram #1). At this time, the Lieutenant from Engine 2 was directed by the IC to follow the line in and provide assistance for the two fire fighters (victim and Fire Fighter #1) who had just entered the structure. The search proceeded to the bathroom at the end of the hall and then on to the master bedroom. The IC also directed a fire fighter from Engine 2 to take a 1 3/4-inch preconnect and hit the remaining fire in the garage. The fire fighter from Engine 2 who was hitting the garage fire reported that the water running down the driveway was mixed with burning gasoline. He also reported that there were spot fires throughout the garage and that he was unable to see the back of the garage due to the thick, black smoke. The Lieutenant from Ambulance 3 directed one of his fire fighters from Ambulance 3 to man the Personnel Accountability Report (PAR) board while the other fire fighter from his crew put on his bunker gear. The fire fighter from Ambulance 3 reported only two tags were on the board (tags belonging to the Lieutenant and fire fighter from Engine 2). He then updated the board with the tags he was given. The victim’s tag was not included, and it wasn’t until the fire fighter from Ambulance 3 became aware that the victim was missing that he was able to add the victim’s name to the board. The Lieutenant from Ambulance 3 reported to the IC and the IC informed the Lieutenant that the fire was hard to knock down and that it kept flaring up. The driver from Engine 2 charged the 5-inch supply line. He then took over as the Engine Operator E/O for Engine 1 and had difficulty getting an exact pressure, so he kept it between 160-165 psi.
As the victim was completing his search of the master bedroom, the Lieutenant from Engine 2 met up with Fire Fighter #1 outside the doorway to the master bedroom. At this time a second crew was sent in to conduct a primary search of the first level and to ventilate by opening windows. The second crew went in through the front door and proceeded toward the dining room (see Diagram 1). Having zero visibility, they broke out the dining room window to help ventilate some of the smoke from the structure. The fire fighters from the second crew reported that the heat intensified after they broke out the window. At approximately the same time, the fire fighter from Engine 2 saw a glow in the back of the garage and was concerned about pushing fire onto the crews inside. He reported this to the IC and was told to hold off on attacking the garage fire. It was at approximately this same time that the victim was exiting the master bedroom and the Lieutenant turned and saw a glow at the end of the hallway near the stairway. The heat was building rapidly, so the Lieutenant took the nozzle from Fire Fighter #1 and attempted to spray water toward the end of the hallway. Note: Unknown to the Lieutenant and the fire fighters, an open swamp cooler vent was directly above them in the ceiling (see Diagram 1, Diagram 3, Photo 2, and Figure). The Lieutenant was on his knees and had to turn his upper body, pulling the hose line around his mid-section. The charge on the line dropped just as the Lieutenant turned to spray water toward the end of the hall. When he opened up the nozzle, the water pressure was inadequate, making it impossible to knock down the heat. Note: The reason for the sudden decrease in the water pressure was not determined. The driver of Engine 2 reported that no problems were ever encountered with either the water supply or Engine 1. The heat was building rapidly upstairs, so the Lieutenant, Fire Fighter #1, and the victim attempted to move toward the end of the hall away from the heat. Note: The Lieutenant and Fire Fighter #1 reported that the heat was so intense, it became difficult to think or function. Due to the intense heat, the Lieutenant, Fire Fighter #1, and the victim moved farther down the hall toward the door to bedroom #2. The Lieutenant attempted to radio for help but received no response. Believing he may not have keyed the radio, he took off his glove and tried to call out again. This is when he received third-degree burns to his hand. The IC stated he never received a call for help. The Lieutenant, Fire Fighter #1, and the victim moved back down the hall to in front of the doorway to the master bedroom. The Lieutenant then decided that they had to follow the hose line back down the hall toward the front door to get out. Note: No communication conveyed this decision to Fire Fighter #1 or the victim. The Lieutenant felt that they understood what he wanted them to do. Fire Fighter #1 preceded the Lieutenant on the hose line, and the Lieutenant believed the victim was following him. The Lieutenant and Fire Fighter #1 reported hearing a positive pressure fan as they neared the end of the hall. The fan had been placed at the front door after the second crew had entered the structure. When Fire Fighter #1 reached the top of the stairs, he stopped due to the intense heat traveling up the open stairway (see Figure). The Lieutenant grabbed Fire Fighter #1 and pushed him down the steps. The second crew, feeling the extreme heat after breaking out the dining room window, decided to backtrack and exit out the front door. The second crew reported to the IC that they didn’t see any fire but felt extreme heat. A third crew (one fire fighter and the E/O from Engine 3) were sent in with a 100-foot, 1 3/4-inch preconnect hose line from the front of Engine 1 to provide backup for the first crew. The third crew’s line, when stretched completely out, would only reach the first set of steps of the stairway to the hallway (see Diagram 1 and Figure). Having zero visibility, the third crew heard someone falling down the stairs behind them but never saw who it was. The third crew then saw fire moving up the stairs from the basement, and due to the extreme heat, had to drop to their bellies (the stairs extended from ground level upward; see Diagram 1, Diagram 2, and Figure). At approximately 2221 hours, Fire Fighter #1 fell over the positive pressure fan as he came out the front door followed by the Lieutenant. The third crew applied a straight stream with their 1 3/4-inch hose line down the stairs and then went to a fog stream to try and protect themselves from the heat. The Lieutenant asked the IC if the victim had come out behind him, and the IC replied that he hadn’t come out. The Lieutenant and Fire Fighter #1 then received medical attention for their burns and for heat exhaustion. The IC then ordered a Personnel Accountability Report (PAR), and everyone was accounted for except the victim. The IC didn’t know if the victim was still inside the structure or if he had possibly exited the building on the west side. The Lieutenant from Ambulance 3 directed a fire fighter from Engine 3 and a fire fighter from Ambulance 3 to do a search of the outside of the building for the victim. They didn’t find the victim but reported to the IC fire showing on the back side of the structure. The initial third crew-one fire fighter and the E/O from Engine 3 along with one fire fighter from Engine 2-were directed by the IC to reenter the structure to search for the victim who might still be upstairs. Note: This crew was never a designated Rapid Intervention Team (RIT). The crew entered through the front door and proceeded to the stairway. The fire fighter from Engine 2, accompanying the third crew, tried to go up the stairs but was concerned about proceeding any further because the stairs felt “spongy.” The third crew found the nozzle from the first crew’s hose line. The line felt charged but when they attempted to use it, the water would only spray about 3 feet. The third crew then proceeded with the hose line they originally had with them until they saw fire starting to move up the stairs. They applied water to the stairs leading toward the family room. The crew did not proceed any further due to their belief that the floor might collapse. The third crew then heard someone yell for everyone to get out, so all three of them exited the structure. The third crew reported to the IC that the stairs felt “spongy” and that they believed the top of the landing may have burned out. The Lieutenant from Ambulance 3 assembled a Rapid Intervention Team (RIT) with two fire fighters from Ambulance 1 who had just arrived on the scene. The IC, having received a report that the stairway may be compromised, was concerned about sending the RIT into the structure to look for the victim. The IC was also concerned about the stability of the roof over the garage, so he was hesitant about sending fire fighters in through the front bedroom windows above the garage. The Lieutenant from Ambulance 3 directed a fire fighter from Engine 3 and a fire fighter from Ambulance 3 to pull the 1 3/4-inch cross lay to hit the fire showing in the back of the structure. The E/O from Engine 3 and a fire fighter from Engine 3 accompanied them around to the back of the structure. They brought a ladder with them and began pulling siding down and hitting the fire on the southwest corner of the ground floor. While on the ladder, they did not hear any Personal Alert Safety System (PASS) device or low air bells (they were directly below the master bedroom window where the victim was found). The RIT stood by on the front lawn for approximately 2 minutes until the IC decided to have the RIT attempt a search through the upstairs bedroom windows over the garage. The IC instructed the RIT to stay near the edge of the garage roof and to use an ax to “sound” the roof for weak spots. The RIT threw a ladder to the garage roof in front of bedrooms #1 and #2 (see Diagram 1, Photo 1, and Photo 2). They used an ax to “sound” their way to bedroom #1’s window. The window had been broken out by a water stream from the 2½-inch line that was positioned in the driveway. As one of the fire fighters looked and yelled into the bedroom window, the other fire fighter proceeded toward bedroom #2’s window. A fire fighter from Engine 2 climbed onto the garage roof to assist the RIT. They continued to yell into the window but did not hear any verbal response or PASS device sounding. One of the RIT fire fighters had just broken out the window of bedroom #2 when he heard what he believed to be a PASS device going off. He yelled to the other RIT member, who was still at bedroom #1’s window, that he could hear a PASS device. The RIT entered through bedroom #2’s window while the fire fighter from Engine 2 stayed at the window and kept verbal contact with the RIT (see Diagram 1, Photo 1, and Photo 2). They immediately began searching the room when they realized that the alarm they were hearing was actually the audible alarm on the smoke detector in the house. They searched out into the hallway and to their right, which led them into bedroom #1. While searching bedroom #1, one of the fire fighters spotted a light on the floor of the room across the hall (the master bedroom). Believing it was the victim’s flashlight, they proceeded immediately to the master bedroom. They located the victim’s flashlight and his helmet on the floor near the wall. They both continued searching and simultaneously felt the air pack on the victim. The victim was in a crawling position with his face down in the corner. They never heard his PASS device sounding. The victim was found with his mask off. He apparently took his mask off and had turned his hood around, covering his face, in an attempt to filter out the smoke. The victim was unresponsive and not breathing. The two fire fighters immediately began dragging the victim by his shoulder harness across the hall toward the window in bedroom #2. One RIT member ran out of air and had to leave the other fire fighter to continue dragging the victim by himself. The fire fighter from Engine 2, still at the window, then entered and helped drag the victim to the bedroom window. The fire fighters who were waiting on the roof and in the driveway assisted in bringing the victim down from the garage roof. The victim was then transported by medical helicopter to a nearby hospital where he was pronounced dead at 2317 hours.
CAUSE OF DEATH
According to the Medical Examiner, the victim died as a result of smoke and soot inhalation and acute carbon monoxide intoxication (CO levels were at 25% saturation but may not accurately reflect his level due to intubation and resuscitation efforts).
RECOMMENDATIONS AND DISCUSSION
Recommendation #1: Fire departments should establish and implement written standard operating procedures (SOPs) regarding emergency operations on the fireground.1,2,3
Discussion: SOPs are a set of organizational directives that establish a standard course of action on the fireground to increase the effectiveness of the fire fighting team. SOPs are characterized as being written and official. They are applied to all situations, enforced, and integrated into the management model. Unwritten directives are difficult to learn, remember, and apply. One approach to establishing SOPs is to have officers and fire fighters decide how all operations will be conducted and then commit those decisions to writing. At the time of the incident, the department did not have written SOPs regarding fireground operations.
Recommendation #2: Fire departments should ensure that the Incident Command conducts a complete size-up of the incident before initiating fire fighting efforts, and continually evaluates the risk versus gain during operations at an incident.3,4
Discussion: The initial size-up conducted by the first-arriving officer allows the officer to make an assessment of the conditions, allowing his decisions to be proactive as opposed to reactive. The following general factors are important considerations: (1) occupancy type involved; (2) smoke conditions; (3) type of construction; (4) age of structure; (5) exposures; and (6) time considerations such as time of incident, time fire was burning before arrival, time fire was burning after arrival, and type of attack. The IC’s initial size-up involved all available information received prior to his arrival and what he saw upon his arrival on the scene (the south, east, and north sides of the structure). A view of the west side of the structure may have revealed fire extension in the family room located directly behind the garage. A view of the swamp cooler vent located on the roof may have revealed self-venting as evident from the soot stains on the outside of the vent (see Photo 2). This information would have given the IC a better understanding of the risks and hazards involved with this incident. The additional information would have helped in the decision-making process and the development of an effective attack plan.
Recommendation #3: Fire departments should ensure that fire fighters conducting a search above a fire take safety precautions to reduce the risk of being trapped.4,5
Discussion: Vincent Dunn’s Safety and Survival on the Fireground lists several precautions that fire fighters can take to reduce the risk of being trapped. These precautions include, but are not limited to the following:
1. Notifying your officer when you go above a fire. Even if your assignment has been preplanned, inform your officer by portable radio. This information is a form of fireground control that increases fire fighter safety. An IC should know where all of his assigned fire fighters are operating during a fire.
2. Sizing up the fire. Most fire fighters are trapped on a floor above a fire because they failed to size up the fire below them. The condition on the fire floor should be analyzed before going above. The fire fighter should attempt to determine the approximate location of the fire. Next, the size and intensity of the fire should be observed to see if the fire can be extinguished by the hose attack team. If the fire appears beyond control of the fire fighters operating the hose line, they should not go above.
3. Sizing up the stairway design. The type of stairway leading to the floor above must also be evaluated by the fire fighter. An open stairway, such as the one found in this structure, is the most dangerous stairway a fire fighter can climb when searching above a fire. It becomes a chimney flue, allowing the flame, heat, smoke, and toxic gases generated by the fire below to flow up the open stairway leading to the second-floor bedrooms.
4. Sizing up a second exit for escape. If the interior stairs used by fire fighters to go above a fire suddenly becomes filled with heat and flames, they cannot use this path to get back down. They must locate a second exit for their emergency escape. Before entering a burning building to search above the fire, fire fighters should examine the front of the structure and look for a second exit. A portable ladder already raised to a second floor bedroom window, a porch roof, or fire escape may provide an escape if the interior stairs become impassable because of fire.
5. Building construction size-up. The degree of danger or threat of being trapped above a fire is greatly influenced by the construction of the building. A wood-frame building poses the greatest threat to fire fighters who must search above a fire. Vertical fire spread is more rapid in this type of structure. The three common types of vertical fire spread are stairways, windows, and concealed spaces. In addition to these three, the wood-frame construction offers a combustible exterior that would also allow vertical fire spread on the exterior of the building.
When fire fighters are killed above a fire, a careful analysis may reveal a chain of events as the cause of the fatality, not a single event or mishap. Typically, fire fighters first become disoriented. They are lost in smoke, entangled in some object, or confused by the sudden increase in heat or flame. Next, fire fighters are unable to find an exit from which to escape, and thus are overcome by smoke or toxic gases after their SCBAs have run out of air.
The findings of the State Fire Marshal’s report and the fire department’s fire investigation report both concur that the family room on the ground floor flashed over, with the contents of the room being totally consumed by fire (see Diagram 2). This flashover would have produced the sudden increase in temperature reported by all of the fire fighters who were inside the structure just before exiting. The open swamp cooler vent located above the fire fighters at the end of the hallway (see Diagram 1) was vertically ventilating the upper portion of the structure. The vent cover in the ceiling was not in place. The ventilation system had been recently serviced by a technician. This created a chimney effect, drawing heat from the family room, up the open stairway, and in the direction of the opening for the swamp cooler vent directly above the Lieutenant, Fire Fighter #1, and the victim (see Diagram 3). The Lieutenant who was assigned to provide assistance to Fire Fighter #1 and the victim was equipped with a portable radio but did not attempt to communicate with the IC until they were in need of assistance when they were overwhelmed by the heat. When the Lieutenant attempted to radio out a call for help, the signal from the portable radio was not received by the IC or Central Dispatch.
Recommendation #4: Fire departments should ensure that a separate Incident Safety Officer (ISO), independent from the Incident Commander, is appointed.6, 7, 8
Discussion: According to NFPA 1561, paragraph 4-1.1, “the Incident Commander (IC) shall be responsible for the overall coordination and direction of all activities at an incident. This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the IC is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished.” According to NFPA 1500, paragraph 6-1.3, “as incidents escalate in size and complexity, the IC shall divide the incident into tactical-level management units and assign an ISO to assess the incident scene for hazards or potential hazards.” The most effective ISOs are those who operate as a consultant to the IC. The ISO establishes a relationship with the IC by asking what the action plan is, followed by a summary of the current situation status and resource status. With this information, the ISO can collect more information in the form of a reconnaissance or 360-degree size-up of the incident. With this additional information, the ISO can report concerns and possible solutions to the IC. During this incident, the IC was also acting as the Safety Officer and thus was limited in being able to perform the additional functions of a separate ISO.
Recommendation #5: Fire departments should ensure that Incident Command always maintains close accountability for all personnel at the fire scene.6, 7, 8, 9, 10
Discussion: Accountability on the fireground is paramount and may be accomplished by several methods. In this particular incident, the tag system was utilized. The tag system can aid in accounting for personnel within the fireground perimeter. Personnel can be equipped with a personal identification tag. Upon entering the fireground perimeter, fire fighters leave their tags at a given location or with a designated person (command post, apparatus compartment, company officer, control officer, or sector officer). After arriving on the scene, the Lieutenant from Ambulance 3 directed one of his fire fighters from Ambulance 3 to man the PAR board. The fire fighter from Ambulance 3 reported that only two tags were on the board. The tags were those of the Lieutenant and fire fighter from Engine 2. He then updated the board with the tags he was given. The victim’s tag was not included, and it wasn’t until the fire fighter from Ambulance 3 became aware that the victim was missing that he was able to add the victim’s name to the board.
Recommendation #6: Fire departments should ensure that a Rapid Intervention Team (RIT) stand by with equipment, ready to provide assistance or rescue.7, 9, 10
Discussion: In the early stages of an incident, which includes the deployment of a fire department’s initial attack assignment, the Rapid Intervention Team(s) should be in compliance with NFPA 1500 paragraph 6-4.4 and 6-4.4.2 and be either one of the following: (a) on-scene members designated and dedicated as a Rapid Intervention Team(s), or (b) on-scene members performing other functions but ready to redeploy to perform RIT functions. A RIT was not established until the Lieutenant from Ambulance 3 assembled two fire fighters as a RIT. This was done upon discovering that a fire fighter (victim) was not accounted for and might still be inside the structure.
Recommendation #7: Fire departments should consider providing fire fighters with a Personal Alert Safety System (PASS) integrated into their Self-Contained Breathing Apparatus (SCBA).
Discussion: A PASS that is integrated into the fire fighter’s SCBA would activate when the fire fighter turns on his air supply. The victim had a manually activated PASS device. The victim’s PASS device was not activated at the time of the incident. The PASS device was manually operated by NIOSH investigators and found to be in good operational condition, emitting a loud and clear audible signal. The fire fighters who found the victim did not hear a PASS alarm when they found the victim. The fire department had purchased integrated PASS devices prior to the incident and is in the process of purchasing additional integrated PASS devices. Where fire departments utilize manually operated PASS devices as with this department, the fire fighters should be trained and routinely reminded to activate their PASS devices when operating on the fireground. Activation of manually operated PASS devices should be enforced to ensure the safety of all fire fighters on the fireground.
Recommendation #8: Fire departments should ensure that the Incident Commander be clearly identified as the only individual responsible for the overall coordination and direction of all activities at an incident.7
Discussion: The Incident Commander (IC) shall be responsible for the overall coordination and direction of all activities at an incident. The incident management system shall clearly identify who is in overall command at the scene for the duration of the incident. The IC shall make assignments based on the availability, qualifications, and expertise of individuals. It is imperative that the IC clearly be in charge of all operations on the fireground to ensure the successful completion of an operation. This particular incident had an established IC, but some of the operations at this particular incident were directed by personnel other than the IC and some efforts were not coordinated with those of the IC. An effective fireground operation revolves around one incident commander. If there is no command, or if there are multiple commands, fireground operations can quickly break down.
Recommendation #9: Fire departments should ensure that the Incident Commander maintains the role of director and does not become involved as a laborer.11
Discussion: Company officers who find themselves in the first-in leadership capacity will find a compulsion to get involved in handwork. This compulsion to get involved in fire fighter activities will be lessened if an IC can physically detach themself from the emergency. This detachment would allow the IC to assume the role as a director, not a laborer. If they are equipped with handheld radios, they can move to a vantage point away from the hands-on activities, thus allowing them the freedom to assign companies and delegate functions.
REFERENCES
1. NFPA [1997]. Fire protection handbook. Quincy, MA: National Fire Protection Association.
2. International Fire Service Training Association[1995]. Essentials of fire fighting. 3rd ed. Stillwater, OK: Oklahoma State University.
3. Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
4. Dunn V [1992]. Safety and survival on the fireground. Saddle Brook, NJ: Fire Engineering Books & Videos.
5. International Fire Service Training Association [1998]. Essentials of fire fighting. 4th ed. Fire Protection Publications.
6. Smoke CH [1999]. Company officer. New York: Delmar Publishers.
7. NFPA [1995]. NFPA 1561, standard on fire department incident management system. Quincy, MA: National Fire Protection Association.
8. NFPA [1997]. NFPA 1521, standard for fire department safety officer. Quincy, MA: National Fire Protection Association.
9. Dodson DW [1999]. Fire department: incident safety officer. New York: Delmar Publishers.
10. NFPA [1997]. NFPA 1500, standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
11. Page JO [1973]. Effective company command for company officers in the professional fire service. Alhambra, CA: Borden Publishing Co.
INVESTIGATOR INFORMATION
This incident was investigated by the following: Mark McFall, Safety and Occupational Health Specialist; Richard Braddee, Team Leader; and Tom Mezzanotte, Safety and Occupational Health Specialist, Division of Safety Research, NIOSH.
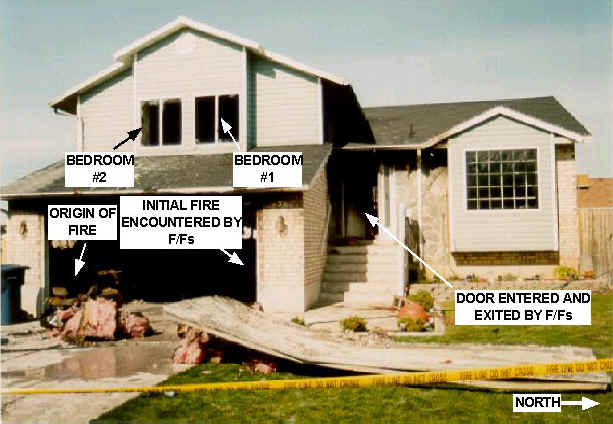
Photo 1. Photo of the front of the house taken from the street; photo shows Bedrooms #1 and #2, the door entered
and exited by the fire fighters, the origin of the fire, and the initial fire encountered by the fire fighters.
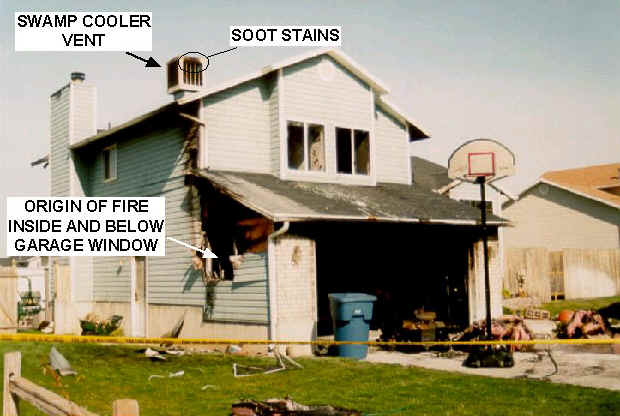
Photo 2. Photo showing the front and south end of the house taken from the street; photo shows
the origin of the fire, inside and below the garage window, and the swamp cooler vent with soot stains.
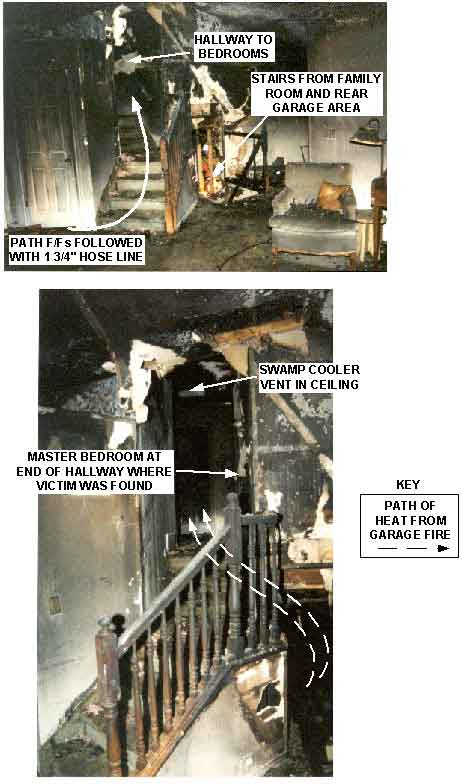
Figure. Two interior photos of the burned-out stairwell of the house; arrows indicate the path of heat produced by the fire, traveling from the garage and continuing up the stairwell. Another set of arrows indicate the path followed by the fire fighters entering the front door and traveling up the stairwell. Photos point out the location of the hallway to the bedrooms, the stairs from the family room and rear garage area, and the swamp cooler vent in the ceiling.
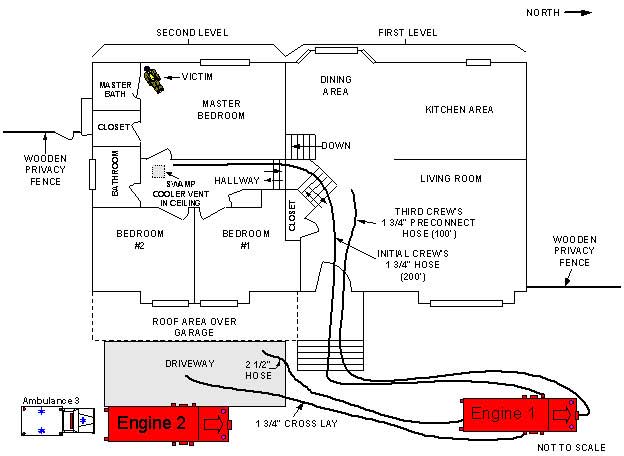
Diagram 1. Diagram depicting the floor plan of the first and second levels of the structure; diagram shows
the placement of Engines 1 and 2, the paths of the hoselines extending from each fire engine, and the position of the victim.
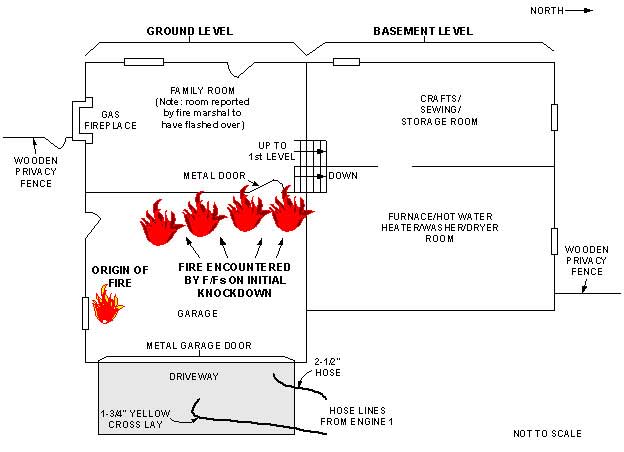
Diagram 2. Diagram depicting the floor plan of the ground and basement levels of the structure; diagram shows the origin of the fire and the fire encountered by fire fighters on the initial knockdown.
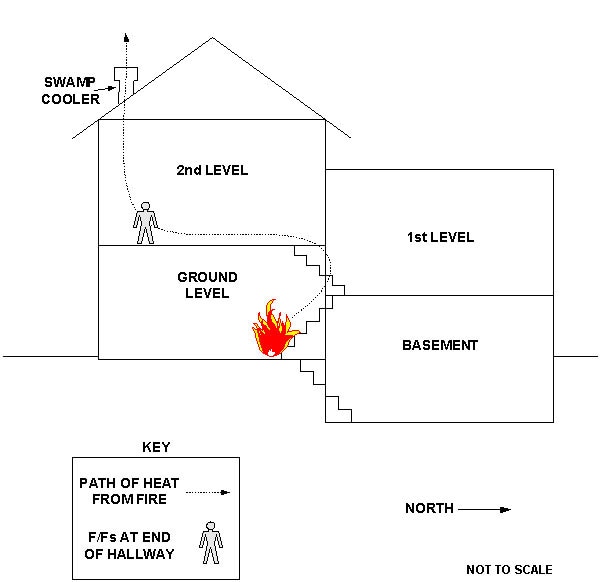
Diagram 3. Diagram depicting the three-dimensional, side view of the structure; diagram shows
the path of heat from the fire and the placement of the fire fighters in the upstairs hallway.
APPENDIX
The following is a summary of NIOSH Task No. TN-11502. For a full report, including photos, tables, and diagrams, contact NIOSH, Division of Respiratory Disease Studies, Respirator Branch at (304) 285-5907.
Status Investigation Report of One
Self-Contained Breathing Apparatus
NIOSH Task No. TN-11502
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Respirator Branch agreed to examine, test, and evaluate one Survivair 2216 psi, 30-minute, self-contained breathing apparatus (SCBA). This SCBA was last used by a fire fighter who died while fighting a fire on the evening of March 31, 2000.
This SCBA status investigation was assigned NIOSH Task Number TN-11502. The tests and evaluations were conducted in accordance with selected performance tests as listed in the approval requirements of Title 42, Code of Federal Regulations (CFR), Part 84. Additional tests – the NFPA Air Flow Performance test and a series of Biosystems PosiChek3 performance tests – were also conducted. The Fire Department was further advised that NIOSH would provide a written report of the inspection and applicable test results. Test failures would be noted, but the SCBA would not be dis-assembled in an attempt to determine the cause of any noted test failure.
The SCBA, sealed inside a cardboard box, was shipped by the Fire Department to the NIOSH Appalachian Laboratory for Occupational Safety and Health (ALOSH). The package was received by NIOSH on May 4, 2000. Due to renovation work in and around the Firefighter SCBA Evaluation Lab, evaluation of the SCBA had to be postponed. During renovation, the SCBA was stored in its unopened box under lock in the lab. The box was opened on Friday, June 2, 2000, in order to perform a preliminary inspection of the SCBA. On the following Monday, June 5, 2000, the SCBA unit was un-boxed, inspected, and prepared for testing. Inspection of the unit was completed on June 5, 2000, and performance testing was conducted on June 6 and 7, 2000.
SCBA Inspection
The blue plastic SCBA carrying case from the Fire Department was opened on Friday, June 2, 2000, in room H-178A of the ALOSH Building in order to perform a preliminary inspection. The case was re-opened on the morning of Monday, June 5, 2000. The contents of the box were inspected by Thomas McDowell, Physical Scientist, of the Respirator Branch, Division of Respiratory Disease Studies (DRDS), NIOSH.
The carrying case contained one complete Survivair SCBA with a Personal Alert Safety System (PASS) unit attached to the waist belt.
The SCBA was examined component by component in the condition as received to determine its conformance to the NIOSH-approved configuration. Internal inspections of individual components requiring disassembly were not performed. The entire inspection process was videotaped. The condition of each major component was also photographed. Photos are contained in Attachment Three.
The SCBA inspection is summarized in Attachment One.
SCBA Testing
Testing of the SCBA was initiated on June 6, 2000, and was completed on June 7, 2000.
The SCBA was tested in the condition as received from the Fire Department. No maintenance was performed on the unit prior to testing. The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations (CFR), Part 84, Subpart H. Further testing was conducted to determine conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, 1997 Edition. A series of tests utilizing a Biosystems PosiChek3 computerized SCBA performance tester was also conducted.
The following performance tests were conducted:
NIOSH SCBA Certification Tests (in accordance with the performance requirements of Title 42, Code of Federal Regulations (CFR), Part 84):
-
-
-
-
- 1. Positive Pressure Test [84.70(a)(2)(ii)],
- 2. Rated Service Time (duration) [84.95],
- 3. Gas Flow Test [84.93],
- 4. Exhalation Breathing Resistance Test [84.91(c)],
- 5. Static Facepiece Pressure Test [84.91(d)],
- 6. Remaining Service Life Indicator Test (alarm) [84.83(f)].
-
-
-
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service – 1997 Edition):
-
-
-
-
- 7. Air Flow Performance Test
-
-
-
Biosystems PosiChek3 computerized SCBA performance tests:
-
-
-
-
- 8. Facepiece Leak Test
- 9. Activation/Static Pressure
- 10. High Pressure Leak Test
- 11. Breathing Test (Standard Work Rate: 40 liters per minute)
- 12. Breathing Test (Max Work Rate: 100 liters per minute)
- 13. Pressure Gauge Accuracy
- 14. Alarm Accuracy
- 15. Bypass Check
-
-
-
SCBA Test Results
The SCBA met the requirements of all six NIOSH SCBA Certification tests performed. The SCBA also met the requirements of the NFPA Air Flow Performance Test and all tests performed using the Biosystems Posichek3.
Attachment Two contains the complete NIOSH, NFPA, and Biosystems PosiChek3 test reports for the SCBA. Table One summarizes the NIOSH test results. Table Two summarizes the NFPA test results. Table Three summarizes the PosiChek3 test results.
Summary and Conclusions
Inspection of the SCBA shipped to NIOSH by the Fire Department was completed on June 5, 2000. The SCBA was worn and had the appearance of having seen considerable use. Although component part numbers could not be completely identified on a few component parts, the SCBA appeared to be in the approved condition for a Survivair SIGMA, 30-minute, 2216 psi, SCBA (NIOSH approval number TC-13F-285).
The SCBA was thoroughly inspected and determined to be in a condition safe for testing. The SCBA inspection is summarized in Attachment One.
The SCBA met the requirements of all performance tests conducted on the SCBA. The complete SCBA test report with results of all performance testing conducted on the SCBA is presented in Attachment Two.
A collection of digital photos taken following the inspection is contained in Attachment Three.
The status of the SCBA with regard to its conformance to the performance standards prior to the incident cannot be determined.
In light of the information obtained during this investigation, the Institute has proposed no further action at this time. Following inspection and testing, the SCBA was stored under lock in Room H-178A of the NIOSH ALOSH Building. At the request of the Fire Department, the SCBA was shipped via Federal Express on Friday, June 16, 2000.
Investigator Information
Inspections and SCBA performance tests were conducted by and the report was written by Thomas McDowell, Physical Scientist, Respirator Branch, Division of Respiratory Disease Studies, National Institute for Occupational Safety and Health, located in Morgantown, West Virginia.
This page was last updated on 11/21/05