
Maintenance Worker Dies After Pinned Between Overhead Bridge Crane and Roof Truss
Wisconsin Case Report 05WI054
Summary
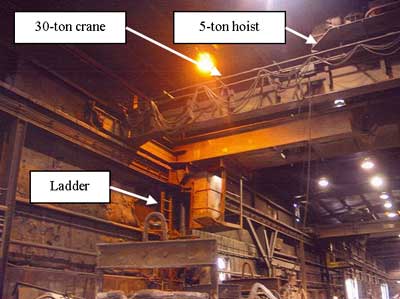
On August 2, 2005, a 55-year-old maintenance worker (the victim) was pinned between an overhead bridge crane and a roof truss. The victim was part of a two-man maintenance team that ascended 20 feet up a ladder and climbed onto a 30-ton Whitney bridge crane. The victim and another maintenance man were going to adjust the brakes on the 5-ton hoist on the crane (Figure 1). While the operator of the Whitney crane had his back turned from the controls, a second operator came over and moved the crane. He did not know that the victim and another maintenance man were working on the crane above. The first operator realized what was happening and yelled to stop the movement, but it was too late. Management notified the Emergency Medical Services (EMS) at 8:28 a.m. EMS arrived at 8:31 a.m. The conditions the rescue personnel worked in included extreme heat, poor illumination, noise, and the accident site that was located over 25 feet above them. The FACE investigator concluded that to help prevent similar occurrences, employers should:
- ensure that employees follow proper lockout tagout procedures on machinery before performing any repair, maintenance, or adjustments.
- ensure that the employer conducts annual or more frequent inspections of the energy control procedures.
- ensure that all controls are placed at the off position when adjustments and repairs are started on cranes.
- ensure that warnings or “out of order” signs are placed on the cranes as well as on the floor beneath or on the hood where they are visible from the floor.
|
|
Figure 1. 30-ton Whitney bridge crane with 5-ton hoist.
|
Introduction
On August 2, 2005, a 55-year-old maintenance worker (the victim) suffered a fatal injury when he was pinned between an overhead bridge crane and a roof truss (steel I-Beam). The FACE investigator learned about the incident from the death certificate. The FACE investigator reviewed official reports. On July 11 the investigator met with the owner of the company for an on-site interview.
The company consisted of a foundry and patter shop that produced Gray Iron castings, ranging from 1 to 40,000 pounds. These castings were made of brass, aluminum, or were ductile iron. The company employed 58 workers with the greater number of employees in castings production. The foundry was in business since 1969 and was under the control of the current owner since 1990. The victim had been employed as a maintenance worker for the past year and a half.
An outside safety consultant provided both classroom and on-the-job training. The company had a written safety and health program and provided training for the employees on lockout/tagout procedures. Regular monthly safety meetings were documented. The program procedures were task-specific for the employees to follow. The company did not do an annual audit of lockout tagout as required by OSHA.
Back to Top
Investigation
The victim was an experienced mechanic employed by the company for the past 18 months. On the day of the incident, the victim started work at 5:00 a.m. and was going about his normal maintenance duties. The victim’s supervisor decided to show him how to adjust the brakes on a 5-ton hoist that was mounted on a 30-ton Whitney overhead bridge crane.
The Whitney crane was manufactured in 1976 and was purchased as a used crane in 1996. No operating manuals were received at the time of purchase. The 30-ton Whitney crane had two hoists for lifting. The main hoist had a 30-ton capacity and the auxiliary hoist was 5-ton. The crane had both a mechanical and electrical braking system. The overhead bridge crane was controlled by the crane operator who used a remote control pendant to move the crane. The crane was moving forward when the incident occurred.
The foundry had two other cranes in the bay. One crane was located on each side of the one involved in the incident. The area had poor lighting and visibility was further limited by foundry soot. The area was very hot and noisy due to the furnaces and other foundry equipment.
The victim and his supervisor climbed up a 20-foot ladder to the overhead bridge crane. They went across the bridge to where the 5-ton hoist was located. The crane operator was located on the floor of the foundry (Figure 2). The pendant control moved the 5 and 30-ton hoists up and down or in a side to side motion (Figure 3). The pendant also controlled the movement east and west on the track rails. The power to the crane needed to be in the “on” position to provide for adjustment of the brakes on the 5-ton hoist.

|
|
Figure 2. Pendant control operated from the floor.
|

|
|
Figure 3. Close-up of pendant control.
|
The crane operator left the pendant control and walked a distance of about 5 feet to talk to his supervisor. While the crane operator’s back was toward the pendant controls, another operator from another crane approached the controls. The second crane operator needed to move the Whitney 30-ton crane. The second operator, not knowing that two maintenance personnel were working 20 feet above him on the 30-ton Whitney crane, grabbed the controls to move it out of the way. The Whitney crane was not locked out.
The crane did not have any warning tags about any pending hazards. Consequently, the second operator pushed the button on the pendant control to move the crane. When the second operator pushed the button, the two maintenance men working on the overhead bridge crane were pinned by the roof truss (steel I-Beam) and steel superstructure of the crane. The victim, who was taller than the other maintenance man, was caught and pinned between the steel I-Beam and the crane superstructure. Both the Whitney operator and the supervisor yelled to stop the movement of the crane, but it was too late. The crane had moved only a short distance causing the victim to be pinned.
Cause of Death
The official cause of death was multiple injuries caused by an industrial accident.
Recommendations/Discussion
Recommendation #1: Ensure that employees follow proper lockout tagout procedures on machinery before performing any repair, maintenance, or adjustments.
Discussion: Without the benefit of an effective lockout/tagout program, employees cannot be assured of their safety when working on, around, or above machinery such as an overhead bridge crane. In this case, the victim and the maintenance supervisor relied on the crane operator to maintain control of the pendant. The bridge crane power was not de-energized because power was needed to adjust the 5-ton hoist motor brake. Methods could have been developed to take into account the need to adjust brakes with the power on. Although the company had a lockout/tagout program, in this case the program failed to address the following issues:
- All forms of hazardous energy should be de-energized, isolated, blocked and/or dissipated before work begins.
- Workers should be assigned a lock with one key to secure energy control devices.
- Locks used to secure the energy control devices should be clearly labeled with durable tags to identify the worker assigned to the lock.
- Inventory of all equipment should be conducted for energy sources
- Verification by test and/or observation that all energy sources should be de-energized before work begins.
- All workers should be accounted for and clear of any danger points before reenergizing the system.
Recommendation #2: Ensure that the employer conducts annual or more frequent inspections of the energy control procedures.
Discussion: Reviews of the lockout/tagout program are needed on an annual basis to ensure that the employer provides adequate worker protection. As part of this review, employers must correct any deviations identified in the energy control procedures or its application. The review is conducted to assure that the employees are familiar with their responsibilities under the procedures established and continue to implement energy control procedures properly.
Recommendation #3: Ensure that all controls are placed at the off position when adjustments and repairs are started on cranes.
Discussion: The electrical controllers for the pendant controls of the crane need to be in the off position. This way an employee can safely work on the overhead bridge crane with the power “off.”
Recommendation #4: Ensure that the warning or “out of order” signs are placed on the cranes as well as on the floor beneath or on the hood where they are visible from the floor.
Discussion: By placing highly visible signs, other employees will be warned about the impending danger of employees working above. Arrows pointing up or other signage needs to be used with florescent lettering stating “Danger Men Working Above.” This will alert employees about their surroundings.
References
- Code of Federal Regulations, 29 CFR 1910.147, Lockout/Tagout. Washington, D.C.: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations, 29 CFR 1910.179, Overhead Cranes. Washington, D.C.: U.S. Government Printing Office, Office of the Federal Register.
- OSHA Pamphlet 3120: Control of Hazardous Energy. Revised 2002. Available at https://www.osha.gov/external icon. Date Accessed: July 14, 2006.
Wisconsin Fatality Assessment and Control Evaluation (FACE) Program
Staff members of the FACE Project of the Wisconsin Division of Public Health, Bureau of Occupational Health, conduct FACE investigations when a machine-related, youth worker, Hispanic worker, highway work-zone death, farmers with disabilities or cultural and faith-based community’s work-related fatality is reported. The goal of these investigations is to prevent fatal work injuries studying: the working environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury and the role of management in controlling how these factors interact.
To contact Wisconsin State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.