
Truck Driver Killed After Falling Through Unprotected Skylight
Michigan Case Report: 06MI006
Summary
On February 3, 2006, a 44-year-old male truck driver/crane operator was killed when he fell through a 3 x 8-foot unprotected corrugated fiberglass skylight that was approximately 1/8 to 3/16 inch thick (Photo 1). The decedent was delivering roofing materials to a firm contracted to re-roof the southwest section of a warehouse. He climbed a ladder to the roof and spoke with three roofing contractors about placement of the roofing materials. For reasons unknown, the decedent stepped over a roof parapet wall onto the low-sloped metal warehouse #2 roof that was not near the area where the roofing was to occur. (Figure 1). One of the roofing contractor employees warned the decedent of the skylights on warehouse #2 roof. The decedent took several steps and then fell through a skylight that was flush with the roof. He landed on the concrete floor 20 feet below. The business owner called 911. Emergency response arrived and transported him to a local hospital. After evaluation at this hospital, the decedent was transferred to a second hospital where he died.

|
|
Photo 1. Picture of broken skylight
|
Recommendations:
- Employers should develop, implement, and enforce a comprehensive accident prevention program that includes, but is not limited to, job site hazard surveys and worker training in fall hazard recognition.
- Building owners should install protective guard over skylights to prevent falls through skylights by maintenance or other personnel who may access the roof.
Introduction
On February 3, 2006, a 44-year-old male truck driver/crane operator was killed when he fell through a 3 x 8-foot unprotected corrugated fiberglass skylight. On February 6, 2006, MIFACE investigators were informed by the Michigan Occupational Safety and Health Administration (MIOSHA) personnel who had received a report on their 24-hour-a-day hotline, that a work-related fatal injury had occurred on February 3, 2006. On September 21, 2006, MIFACE visited the site of the incident, but the business owner declined to permit MIFACE to view the incident site. Later that same day, MIFACE drove to the home office location in another state to interview the operations manager of the decedent’s employer. During the course of writing this report, the police report, medical examiner’s report, and MIOSHA file and citations were reviewed. Pictures used in this report are courtesy of the responding police department.
The decedent worked for a multi-state firm that supplied roofing materials. The business location out of which the decedent worked had six employees. The decedent was one of two truck drivers/crane operators. He was employed as a full time, hourly worker and was certified as a crane operator. The decedent had been employed with his current employer for five years, and he had worked at the same location for a different employer driving a crane truck and conducting roofing activities for an additional seven years (thus giving him 12 years of crane truck driving/unloading experience).
The employer had an employee handbook that included employment policies and practices, some general health and safety policies, such as accident reporting and first aid, an explanation of employee benefits, etc. The firm did not have a written health and safety program. Safety meetings were not held with employees. The employer did not have a safety training program, although employees, like the decedent, had attended outside training to become certified operator of the crane truck. The employee handbook did not address inspection of a construction site or recognition of roof hazards such as skylights. The decedent had not been instructed on how to recognize the danger of unsafe conditions on job sites or in fall protection.
MIOSHA Construction Safety and Health Division issued the following alleged Serious citations to the decedent’s employer at the conclusion of their investigation:
- General Rules, Part 1.
- Rule 114(1) – Employer did not develop, maintain, and coordinate with employees an accident prevention program, a copy of which was not available at the worksite.
- Rule 114(2)(c) – No inspection of the worksite to assure unsafe conditions were eliminated.
- Rule 114(2)(d) – Employer did not provide instruction to each employee in the recognition and avoidance of hazards and the regulations applicable to his or her work environment to control or eliminate any hazards or other exposure to illness or injury as part of an accident prevention program.
- MIOSHA Construction Safety Standard – Fall Protection, Part 45.
- Rule 4502, REF OSHA 1926.501(b)(1) – The employee was unprotected from falling by the use of guardrail systems, safety net systems, or personal fall arrest system while on a walking/working surface (horizontal and vertical surface) with an unprotected side or edge which was six feet (1.8 m) or more above a lower level.
- Rule 4502, REF OSHA 1926.503(a)(1) – Employer did not provide a training program for each employee who might be exposed to fall hazards. Thus, the employee did not recognize the hazards of falling and the procedures to be followed in order to minimize these hazards.
- Rule 4502, REF OSHA 1926.501(b)(4)(i) – Each employee on walking working surfaces was not protected from falling through holes (including skylights) more than six feet (1.8 m) above lower levels, by personal fall arrest systems, covers, or guardrail systems erected around such holes.
- Administrative Rule 2139, Recording & Reporting Of Occupational Injuries & Illnesses.
- Rule 1139(1) – Employer did not report orally, work related fatalities, or hospitalization of three or more employees as described in rule 408.2110 within eight hours to the Michigan Department of Labor and Economic Growth, Michigan Occupational Safety and Health Administration.
Back to Top
Investigation
The decedent arrived at his employer’s business location at about 6:30 a.m. and warmed up the crane truck, which was purchased new within the last six months. The truck had been loaded with 4×8-foot membrane sheets and 10-foot rubber rolls. His first delivery of the day was to the incident site. The business owner at the incident site had hired a local roofing company to re-deck part of the rusted, corrugated warehouse roof of his business located on the southwest end of the building. The roofing company subcontracted the decedent’s employer to deliver roofing materials. The decedent arrived at the job site at approximately 8:00 a.m. with the truck crane loaded with materials for the re-roof job.
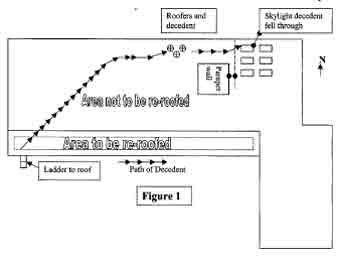 |
The decedent exited the crane truck. The outriggers had not yet been placed. He climbed a ladder to get onto the roof (Figure 1). It was common practice for the decedent to go onto roofs when delivering material, as stated by an employee of both the roofing contractor and the employer’s operations manager. The operation manager stated that the work practice at the time required the crane truck driver to go up on the roof to look for obstructions, wires, and to make sure the roof could handle the load. The operation manager stated that the contract language at the time of the incident stated that that if the roofing material was attached to the crane, the responsibility for the load was the decedent’s employer, not the roofing contractor. Therefore, the company’s individuals who delivered the roofing materials would check the roof prior to unloading the truck.
On the roof were employees of the roofing company that subcontracted the decedent’s employer. While walking on the roof with the roofing company employees, the decedent discussed the location of roofing material placement. When the discussion was completed, the decedent continued walking northbound on the roof stepping over a parapet wall onto the roof of warehouse #2.
Warehouse #2 had six skylights that were installed to provide additional lighting for the building. The roof was dry and not snow-covered. Both the roof and fiberglass panel were weathered and dark in color. Although no work was to be performed in the area, neither the roofing company nor the owner of the building had installed visual markers or barriers to identify the skylight area nor covered the skylights in accordance with MIOSHA requirements.
As the decedent was walking northbound toward the Warehouse #2 roof, one of the roofing company employees warned him about the presence of the skylights. After stepping over the parapet, the decedent took several steps and fell through one of the 3×8-foot corrugated fiberglass panels that were flush with low-sloped metal roof (Photo 2). He landed on the concrete floor 20 feet below. The fiberglass panels were not designed as a weight-bearing skylight. It is unknown why the decedent continued northbound and walked on Warehouse #2 roof, which was so far away from the construction area. The roofing company employees stated to the police that they were not hired to repair that section of the roof. They were contracted to repair the front section or the section to the south/southwest of the building
 |
|
Photo 2. Broken skylight
|
The business owner stated that he was in his office when he was told to call 911 after being advised that one of the roofers had fallen through the roof on the north end of the building. The business owner called 911 and then went to the incident scene. Emergency response arrived and transported the decedent to a local hospital. After evaluation at this hospital, the decedent was transferred to a second hospital where he died.
Three days after the incident, the MIOSHA compliance officer climbed a ladder on the north side of warehouse #2 and observed the metal roof and existing skylights. His report stated that the metal roof and skylights “blended together” making it difficult to distinguish between the two, especially if you were not looking for skylights.
After the incident, the decedent’s employer instituted two new policies to protect their employees from fall hazards:
- No employees, including drivers, are allowed on roofs. Prior to the incident, the employer permitted the crane truck drivers to go up on a roof with unprotected sides and edges without fall protection and conduct a site inspection.
- Changed their boom delivery ticket to read that the employer is not responsible for determining structural integrity of the roof being loaded. Prior to the incident, the roofing supplier was responsible to determine material placement and roof structural integrity. It is now the responsibility of the roofing contractor to determine material placement within parameters of equipment being used.
Back to Top
Cause of Death
The death certificate stated that the cause of death was blunt force trauma injuries to the head. An autopsy was not performed.
Recommendations/Discussion
Employers should develop, implement, and enforce a written accident prevention program that complies with MIOSHA requirements and includes, but is not limited to, job site hazard surveys and worker training in fall hazard recognition.
The company that supplied the roofing material did not have a written accident prevention program as required in MIOSHA Construction Safety Standard, General Rules, Part 1. Although the company had some safety procedures, it provided minimal safety training. Employers should develop, implement, and enforce a comprehensive safety program that includes, but is not limited to, routine job site hazard surveys, the use of appropriate fall protection, and worker training on the recognition and the procedures to be followed in order to minimize these hazards.
MIOSHA Construction Safety Standard, Part 45, Fall Protection requires that employers provide a training program for each employee who might be exposed to fall hazards. Employees must be trained by a competent person qualified in the following areas:
- Nature of fall hazards in the area.
- Correct procedures for erecting, maintaining, disassembling, and inspecting the fall protection systems to be used.
- Use and operation of guardrail systems, personal fall arrest systems, safety net systems, warning line systems, safety monitoring systems, controlled access zones and other protection to be used.
- Role of each employee in the safety monitoring system when this system is used.
- Limitations on the use of mechanical equipment during the performance of roofing work on low-sloped roofs.
- Correct procedures for the handling and storage of equipment and materials and the erection of overhead protection. o Role of employees in fall protection plans.
- Appropriate standards.
Employers should also include provisions in the training program for new employee orientation to the hazards of their job before they begin work.
As listed above, one of the requirements of a fall protection training program is to train each worker in the nature of fall hazards in the work area. Specifically, employers should explain that many workers have died from falls through skylight or roof openings in addition to the more common type of fall – from a roof edge. Workers should be aware of all skylights and roof openings in their work area. They should be instructed:
- Not to sit or step on skylights because they may not support their weight..
- Use fall protection for any work that might result in falls.
- Make sure that all skylights and roof openings are appropriately guarded before work begins.
- Use nets, catch platforms, or fixed covers if guardrails, screens, protective grillwork, and safety belts are not practical.
- Read any safety decals affixed to skylights.
Building owners should install protective guards over skylights to prevent falls through skylights by maintenance or other personnel who may access the roof.
Although the employees of the building owner may rarely access the warehouse roof, the possibility of falling through one of the six skylights still exists if the skylights continue to be unprotected. MIOSHA General Industry Safety Standard, Part 2, Floor and Wall Openings, Stairways, and Skylights defines a skylight as an opening in a roof or floor covered by a translucent or transparent material not capable of supporting 300 pounds applied perpendicularly on any one area. Part 2, Rule 240 states that a skylight guard shall be designed and constructed to withstand a 200-pound load that is applied perpendicularly at any one area on the screen. The guard construction shall be of grillwork with openings not more than four inches long or slatwork with an opening not more than 2 inches wide with length unrestricted. An additional requirement for the guard is that ordinary loads or impacts shall not deflect the material downward to break the skylight glass.
Building owners should install protective guards over individual skylights meeting Part 2 requirements, or consider installing guardrail systems around the perimeter of the skylight area that comply with the requirements contained within Part 45 to eliminate the hazard of an employee falling through the skylight.
References
MIOSHA Standards cited in this report can be directly accessed from the Michigan Department of Labor and Economic Growth, MIOSHA website www.michigan.gov/mioshastandardsexternal icon. The Standards may also be obtained for a fee by writing to the following address: Michigan Department of Labor and Economic Growth, MIOSHA, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan, 48909-8143. MIOSHA Standard Section phone number is (517) 322-1845.
- MIOSHA Construction Safety General Rules, Part 1.
- MIOSHA Construction Safety Fall Protection, Part 45.
- MIOSHA General Industry Safety Standard, Part 2, Floor and Wall Openings, Stairways, and Skylights.
- MIOSHA Administrative Rule 2139, Recording & Reporting of Occupational Injuries & Illnesses, Rule 1139(1).
MIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicineexternal icon, 117 West Fee Hall, East Lansing, Michigan 48824-1315; http://www.oem.msu.edu/MiFACE_Program.aspx. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 5/17/07 (Link updated 8/5/2009)
Michigan FACE Program
MIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 5/17/07
MIFACE Investigation Report # 06MI006 Evaluation (see page 8 of report)
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.